
Abstract
Background:
Community hospitals account for over 84% of all hospitals and over 94% of hospital admissions in the United States. In academic settings, implementation of an Inpatient Diabetes Management Service (IDMS) model of care has been shown to reduce rates of hyper- and hypoglycemia, hospital length of stay (LOS), and associated hospital costs. However, few studies to date have evaluated the implementation of a dedicated IDMS in a community hospital setting.
Methods:
This retrospective study examined the effects of changing the model of inpatient diabetes consultations from a local, private endocrine practice to a full-time endocrine hospitalist on glycemic control, LOS, and 30-day readmission rates in a 267-bed community hospital.
Results:
Overall diabetes patient days for the hospital were similar pre- and post-intervention (20,191 vs 20,262); however, the volume of patients seen by IDMS increased significantly after changing models. Rates of hyperglycemia decreased both among patients seen by IDMS (53.8% to 42.5%, P < .0001) and those not consulted on by IDMS (33.2% to 29.9%; P < .0001). When examined over time, rates of hypoglycemia steadily decreased in the 24 months after dedicated IDMS initiation (P = .02); no such time effect was seen prior to IDMS (P = .34). LOS and 30DRR were not significantly different between IDMS models.
Conclusions:
Implementation of an endocrine hospitalist-based IDMS at a community hospital was associated with significantly decreased hyperglycemia, while avoiding concurrent increases in hypoglycemia. Further studies are needed to investigate whether these effects are associated with improvements in clinical outcomes, patient or staff satisfaction scores, or total cost of care.
Introduction
The hospitalist model of care came into prominence in the United States in the mid- to late-1990s, as insurance companies pushed hospitals to improve quality and reduce costs. Numerous studies demonstrated that hospitalist programs reduced inpatient length of stay, total costs of care, and in some cases, mortality.1-4 Simultaneously, physicians trained in general internal medicine began to gravitate in increasing numbers from the clinic to work full-time in the inpatient wards. 5
In recent years, the model of a dedicated inpatient provider has spread to other specialties within medicine as well.6,7 Inpatient diabetes management services (IDMS) in particular have increasingly been gaining acceptance, given the significant prevalence of diabetes among hospitalized patients 8 and the association of uncontrolled inpatient glycemia with worse clinical outcomes and increased costs.8,9 Indeed, implementation of an IDMS has been shown to reduce inpatient hypo- and hyperglycemia rates, post-operative infections, length of stay (LOS), and readmissions.9-13
However, the benefits of IDMSs have mostly been evaluated in the academic hospital setting 14 ; little is known about the effects of IDMS implementation in community hospitals. Yet, community hospitals represent over 84% of all hospitals and account for over 94% of hospital admissions in the United States. 15 We previously demonstrated that establishing an IDMS in a community hospital with no previous endocrine support resulted in significant improvements in glycemia, LOS, and readmission rates. 11 It is unknown whether changing from a local, private endocrine practice model to a dedicated IDMS (eg, “Endocrine Hospitalist” 16 ) model has similar benefits.
Methods
Study Population
This was a retrospective analysis of adult patients hospitalized at Howard County General Hospital (HCGH), a 267-bed non-academic community hospital within the Johns Hopkins Hospital System, between January 1, 2017 and August 31, 2020. The study protocol was approved by the HCGH Institutional Review Board. All research efforts were in compliance with the World Medical Association’s Declaration of Helsinki.
De-identified hospitalized patient data were extracted from the electronic medical record (EMR). Patients younger than age 18 were excluded from the analyses. The diagnosis codes listed either among the “Hospital Problems” list or “Medical History” in the patient’s EMR were used to define whether a patient had diabetes. The following International Statistical Classification of Diseases and Related Health Problems 10 (ICD-10) codes were used: E08 (Diabetes mellitus due to underlying condition), E09 (Drug or chemical induced diabetes mellitus), E10 (Type 1 diabetes), E11 (Type 2 diabetes), or E13 (Other specified diabetes). A “diabetes patient day” was defined as a day in which a hospitalized patient with diabetes had at least one blood glucose reading (either via lab draw or point-of-care fingerstick). A diabetes patient day “with insulin” was defined as having received at least one dose of either subcutaneous (eg, basal, nutritional, or correctional) or intravenous insulin that day.
For the purposes of this study, once a signed endocrine consult note was entered in the EMR for a hospitalization, every subsequent day in that particularly hospitalization was considered to have been “affected” by endocrinology’s input, and therefore was counted as having been seen by the endocrine service even if the consultant didn’t actually see the patient or signed off the case.
Inpatient Diabetes Management Model
For many years at HCGH a local, private outpatient endocrine practice consulted on hospitalized endocrine and diabetes cases. Practitioners in the group typically took a week on call at a time for the hospital, in addition to limited clinic duties during that week. In August 2018 this model switched when a full-time board-certified endocrine hospitalist was hired by the Johns Hopkins Health System to see all endocrine consultations, with part-time “moonlighter” endocrinologists to cover the weekends. An endocrine Nurse Practitioner (NP) joined the IDMS in September 2019.
Under the new model, in addition to patient care, IDMS responsibilities also included (1) diabetes education for staff, (2) development of Quality Improvement (QI) processes and projects based on best practices and evidence-based glucose management studies, and (3) assessment of process measures and glycemic control to determine intervention effectiveness. To this end, a hospital Glucose Steering Committee was established in September 2018, meeting monthly, with representatives from all disciplines of the hospital participating (eg, Patient Representative, Nursing, Patient Quality and Safety, Pharmacy, Dietary, Case Management, Population Health, Wound Care, Emergency Department, etc.), to examine and discuss potential pitfalls in the delivery of endocrine and diabetes care in the inpatient and immediate post-discharge settings. The EMR subcutaneous insulin order set was edited, and the timing of nutritional rapid-acting insulin dosing was moved to after, rather than before, meals (starting in June 2019). Lectures were given throughout the year to hospitalists, intensivists, emergency physicians, and nursing staff on topics related to diabetes and glycemia.
Outcomes
Primary outcomes included rates of hyperglycemia (defined as a mean daily blood glucose > 180 mg/dL) and hypoglycemia (mild: glucose ≤ 70 mg/dL, moderate: < 54 mg/dL, severe: ≤ 40 mg/dL). Secondary outcomes included hospital length of stay and 30-day readmission rates (30DRR).
For primary analyses, data from September 2017 to July 2018 (“pre-IDMS”) were compared with those from September 2018 to July 2019 (“post-IDMS”), to compare equivalent months of the year. August 2018 was omitted as both endocrine models overlapped at HCGH during this month. For secondary analyses, data from January 2017 to August 2020 were used.
Statistics
Data were transformed as necessary to maintain assumptions of normality. Independent samples t test and the chi-square test were used to compare differences in means and percentages, respectively, between groups. Linear regression was used to evaluate the slope of change of values over time. SPSS v25.0 (IBM Corp, Armonk, NY, USA) and GraphPad Prism 8.4.3 (GraphPad Software LLC, San Diego, CA, USA) were used for statistical analyses.
Results
A similar number of diabetes patient days per month were seen at HCGH from September 2018 to July 2019, as compared to September 2017 to July 2018 (Mean ± SD: 1842.5 ± 114.5 vs 1835.5 ± 175.4 days/month; P = .91). However, the Endocrine Hospitalist saw a significantly greater number of diabetes patient days per month as compared to the private outpatient group (306.8 ± 44.4 vs 192.8 ± 40.0 days/month; P < .0001; Figure 1).
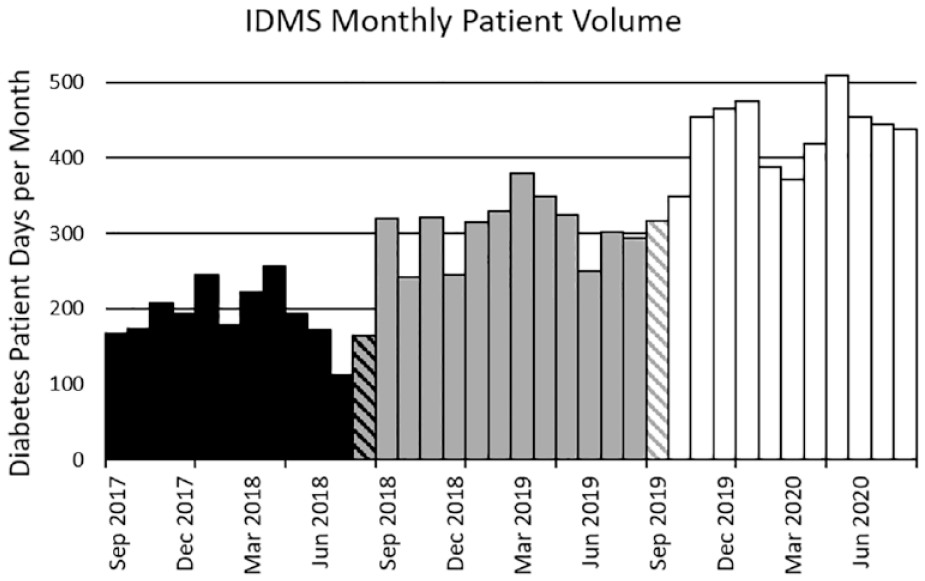
IDMS monthly patient volume. Diabetes patient days per month seen by the HCGH Inpatient Diabetes Management Service (IDMS): local private outpatient endocrine service (black bars), dedicated inpatient Endocrine Hospitalist (grey bars), and Endocrine Hospitalist + Endocrine Nurse Practitioner (white bars). Striped bars represent an overlap between two services for that month.
Among all patients with diabetes, hyperglycemia was significantly less frequent post-IDMS as compared to pre-IDMS (32.0% vs 35.4%; P < .0001). This was true both for patients seen by the endocrine service (42.5% vs 53.8%; P < .0001; Figure 2A), as well as those not seen by the endocrine service (29.9% vs 33.2%; P < .0001; Figure 2B).
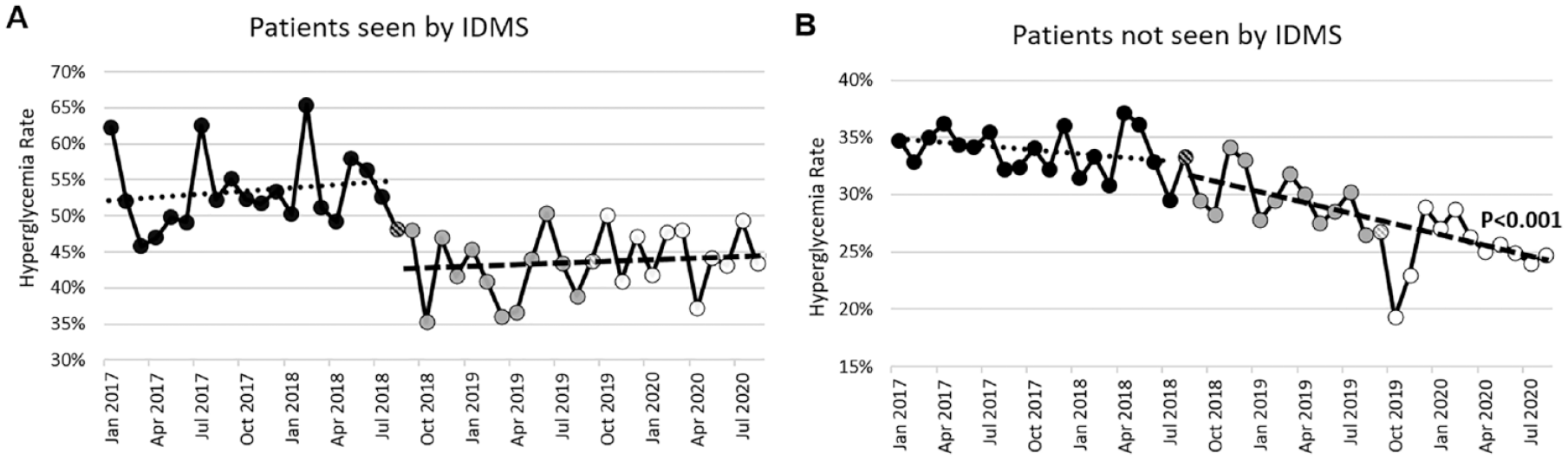
Inpatient hyperglycemia. Rates of inpatient hyperglycemia (defined as % of patient days with a mean blood glucose >180 mg/dL) among patients with diabetes. (A) Seen by IDMS. (B) Not seen by IDMS.
Rates of mild (10.9% vs 11.4%; P = .56), moderate (4.5% vs 5.0%; P = .43), and severe hypoglycemia (1.8% vs 2.3%; P = .21) among patients seen by the endocrine service were not significantly different post- vs pre-IDMS (Figure 3). Similarly, among patients not seen by IDMS, mild (4.9% vs 5.1%; P = .30) and moderate hypoglycemia rates (1.5% vs 1.7%; P = .053) did not change appreciably. Severe hypoglycemia rates slightly, albeit statistically significantly, improved post-IDMS (0.47% vs 0.65%; P = .03).
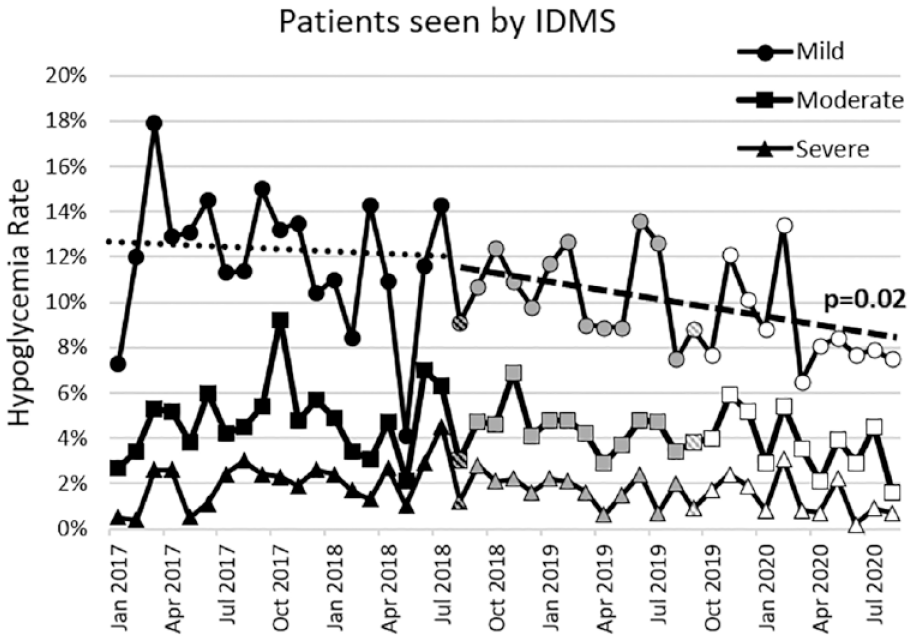
Inpatient hypoglycemia. Rates of inpatient mild (glucose <70 mg/dL), moderate (≤54 mg/dL), and severe (<40 mg/dL) hypoglycemia among patients with diabetes seen by IDMS.
After expanding the IDMS by hiring a dedicated endocrine NP, the volume of the endocrine service over the subsequent 11 months (September 2019 to July 2020) significantly increased to 422.5 ± 59.2 diabetes patient days/month, as compared to the same time period a year prior with only a dedicated Endocrine Hospitalist present (P < .0001; Figure 1). Hyperglycemia rates among patients seen by the IDMS increased slightly (44.7%; P = .047; Figure 2A), although when the sample was restricted to patients on insulin, no difference was seen (50.7% vs 49.0%; P = .13). Mild hypoglycemia rates among patients seen by IDMS continued to decline (9.1%; P = .007 as compared to September 2018 to July 2019), while moderate (4.0%; P = .26) and severe hypoglycemia rates (1.4%; P = .23) were not significantly affected. Moreover, when examined over time from January 2017 to July 2018, mild hypoglycemia was unchanged pre-IDMS (−0.1 ± 0.1%/month; P = .34 for slope significantly non-zero); however, for the 24 months post-IDMS (September 2018 to August 2020) mild hypoglycemia significantly declined with time (−0.13% ± 0.05%/month; P = .02; Figure 3).
Among patients not seen by the IDMS, hyperglycemia rates as measured over time were not significantly affected either in the 11 months pre- (−0.05% ± 0.24%/month; P = .82) or post-IDMS (−0.15% ± 0.21%/month; P = .47). However, when examining over the 24 months post-IDMS, hyperglycemia rates did significantly improve over time (−0.32% ± 0.07%/month; P < .001; Figure 2B). Hypoglycemia rates did not change over time.
LOS among all patients with diabetes was unchanged post- vs pre-IDMS (5.5 ± 0.4 vs 5.3 ± 0.2 days; P = .30). Likewise, restricting the cohort only to patients seen by IDMS also had no significant difference in LOS (6.1 ± 0.8 vs 6.2 ± 0.8; P = .59). 30DRR were also unchanged among all patients with diabetes (16.2% vs 16.0%; P = .80) or among those seen by IDMS (19.4% vs 15.6%; P = .13). Addition of an endocrine NP to the IDMS also had no significant effects on LOS or 30DRR.
Discussion
This study demonstrated that in a community hospital setting changing from a private endocrine consultant model to a dedicated inpatient Endocrine Hospitalist model resulted in significant improvements in hyperglycemia. When the data were examined for 24 months post-IDMS, hypoglycemia rates were significantly reduced as well. These glycemic results are in line with previous studies examining the implementation of an IDMS at large tertiary academic hospitals.9,17,18
Numerous previous studies have demonstrated that poor inpatient glycemic control is associated with worse clinical outcomes, including increased nosocomial and post-operative infections, 19 poor/delayed wound healing, 20 worsened neurologic recovery post-stroke,19,21 COVID-19-related complications, 22 and in certain patient populations, increased mortality.21-23 Not surprisingly, implementation of an IDMS, with resultant improvements in inpatient glycemia, have been associated with significant improvements in clinical outcomes, such as reduced central line-associated bloodstream infections (CLABSI), post-operative infections, and quality of life measures.9,24,25 Moreover, during the COVID-19 pandemic, IDMS has been shown to positively impact the care of patients with diabetes in the community hospital setting. 26
Therefore, it is somewhat surprising that in this study reductions in hyper- and hypoglycemia were not associated with improvements in hospital-related metrics such as LOS and 30DRR. Good inpatient glycemic control has been previously associated with reduced LOS and 30DRR, 27 while in-hospital hypoglycemia has been correlated with increased LOS, 30DRR, and 30-day mortality.28,29 However, the benefits of an IDMS on LOS in previous studies varied widely, with beneficial,9-11 mixed,30,31 or no effects, 17 likely reflecting the inherent variability between study setting characteristics such as hospital size, patient population, IDMS model, IDMS volume, or specialty service examined (eg, medical vs surgical). Similarly, IDMS effects on readmission rates have also shown improved, 11 mixed,31,32 or no effects, 33 depending on the study examined. Of course, inpatient glycemic control is just one piece of the puzzle to patient health, with other issues such as barriers to care, medical literacy, insurance (or lack thereof), demographics, and comorbidity burden also having significant influences on patient LOS and/or 30DRR.34-36
The Endocrine Hospitalist model succeeded in this study, not because of any difference in competence between the providers in the two models, but likely for the same reasons that the general hospitalist model succeeded 20 years ago as compared to the “classic” outpatient private practitioner model. 5 Time is limited, medicine is consistently growing more complex, physicians are only human, and it is very challenging to juggle and provide excellent care to both an outpatient clinic schedule as well as to new inpatient consultations and old follow-ups. An Endocrine Hospitalist, by definition, is only required to focus on the inpatients. In theory, this allows for either more time to be spent with each inpatient on the service or for a larger volume of inpatients seen. 37 Additionally, the Endocrine Hospitalist is present in the hospital during typical workday hours with other hospital staff, enabling participation in rounds and facilitating multidisciplinary communication with hospitalists, other consultants, case managers, and pharmacists. Anecdotally, the Endocrine Hospitalist in this study was consulted on numerous occasions simply because he had walked by or was sitting next to a hospitalist colleague. Visibility begets volume.
The Endocrine Hospitalist model also can incentivize and give protected time for inpatient diabetes-related QI projects. Discussed in detail in other excellent studies,9,38-41 improving inpatient diabetes care is more than simply just administering the correct insulin doses; it is inherently tied to improving systems delivery and fixing systematic errors. Such QI examples include the creation of a Glucose Steering Committee; implementation of standardized, evidence-based order sets and protocols (eg, basal-bolus insulin therapy, hypoglycemia management, insulin infusion, insulin pump, and continuous glucose monitoring); education of nursing and clinical staff; and evaluation and improvement of discharge procedures (eg, creation of diabetes discharge checklist and EMR template). One could posit that a private outpatient consultant may not have the time, resources, or incentives to pursue large QI projects, but with proper planning by hospital leadership, a dedicated inpatient Endocrine Hospitalist could.
Our data also demonstrated that expanding the service to include an endocrine NP increased consult volumes, maintained improvements in hyperglycemia, and continued reductions in hypoglycemia rates. In our particular model, the NP and Endocrine Hospitalist evenly split the consult list, with the NP for the most part only seeing patients with diabetes. Moreover, although not captured directly in the data, adding an NP also allowed for increased education of hospital staff. Having two providers on the team freed one to teach nurses during a monthly Diabetes Nurse Champion lecture series, 42 or give ad hoc lectures to hospitalists, intensivists, and emergency room physicians and nurses, while the other would take the majority of the new consults for that day. As both providers had a passion for education, the Endocrine Hospitalist and NP would take turns educating staff, although this model could be modified such that one provider would provide the majority of the education while the other could focus more on clinical care (and/or administrative tasks, QI project leadership, etc.).
Interestingly, patients that were not seen by the endocrine service also demonstrated profoundly decreased rates of hyperglycemia. This finding may potentially be explained by several factors. Hospitalist education in inpatient diabetes management, as well as updating the insulin order sets, by the Endocrine Hospitalist may have had an effect. Additionally, over time the hospitalists had a significantly fewer number of patients with diabetes which they saw on their own. Presumably the more complicated cases were seen by the IDMS, with only more straightforward diabetes cases being left to hospitalist management, freeing up the hospitalists to focus on other tasks. It would be interesting to assess hospitalist satisfaction and time saved with IDMS initiation.
A certified diabetes care and education specialist (CDCES), formerly known as certified diabetes educator, employed by the hospital was present during both phases of the study. Although her formal role or title did not change with the creation of an IDMS, the CDCES was more intimately integrated into a “team model” of inpatient diabetes care delivery. The IDMS team had more direct verbal communication with the CDCES regarding patients’ educational needs and barriers to care, reviewed and updated note templates and educational handouts together as a group, and worked collectively to obtain new product teaching and demonstration materials. While the effects of this team integration were not measured directly, it likely contributed to the positive effects seen in inpatient hyper- and hypoglycemia.
The strengths of the study include a relatively large number of patient days examined. Additionally, we investigated the changes in glycemic control for both patients seen and not seen by IDMS. The study also has several limitations. The retrospective study design inherently has biases that may not be accounting for other confounding variables. However, the patients with diabetes volumes overall did not change between examined time periods, and it is unlikely that the case mix significantly changed either. As this was a de-identified patient data set, we were not able to obtain other patient covariates, such as age, sex, hemoglobin A1c, or Severity of Illness Index that could have been included into the statistical analyses. Lastly, given the inherently unique characteristics of any particular hospital, the external validity and generalizability of our study results are unclear. However, multiple previous studies at large academic centers have demonstrated improvements glycemic control with IDMS implementation, so we would expect the same to hold true at non-academic community hospitals as well.
Conclusions
In conclusion, switching from a local private practice endocrine consult model to a dedicated IDMS model resulted in improvements in the rates of inpatient hyperglycemia and hypoglycemia in a non-academic community hospital setting. Further research is warranted to investigate the effects of IDMS implementation in a community hospital setting on clinical outcomes, patient and staff satisfaction, and total cost of care. Additionally, investigating and understanding the variables enabling the successful implementation of this program would be important to reproducing its successes at other community hospitals.
Footnotes
Abbreviations
30DRR, 30-day readmission rates; CDCES, Certified Diabetes Care and Education Specialist; EMR, Electronic Medical Record; HCGH, Howard County General Hospital; IDMS, Inpatient Diabetes Management Services; LOS, length of stay; NP, Nurse Practitioner; QI, quality improvement.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.Z. is a consultant for Guidepoint and G.L.G. All other authors declare that they have no conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.