
Abstract
Objective:
This purpose of this study was to conduct a rapid review and environmental scan of diabetes online communities (DOCs) to highlight the clinical impact of DOC engagement and provide guidance to health care providers for navigating and prescribing DOCs.
Methods:
This two-phase review included a rapid review of clinical outcomes and an assessment of DOC content. We conducted a literature search for studies evaluating DOC use and glucometric (glycated hemoglobin [A1C], time-in-range, hypoglycemia), behavioral, and psychosocial outcomes. The environmental scan of current DOC sites established key features, including available platforms, target population, content areas, and reach.
Results:
Twelve papers were included—eight reported DOC use within a context of do-it-yourself (DIY) noncommercial, opensource hybrid closed loop systems community and four were non-DYI related. In latter, all studies were cross-sectional, describing patient-reported outcomes. Two studies reported A1C lowering with DOC use, two DOC use was associated with high self-efficacy, one showed association with higher self-care levels, and one showed higher quality of life scores when compared with population norms. All DIY studies showed improvement in glucometrics after initiation of sensor augmented pump technology with DOC support. Of 54 DOC sites reviewed in the environmental scan, 29 were included. Diabetes online community sites were heterogenous in social media platform and type of diabetes targeted.
Conclusion:
Diabetes online communities have the potential to improve clinical, behavioral, and psychosocial outcomes. Randomized control trials and/or longitudinal prospective studies evaluating outcomes are needed to further examine the potential benefits of DOC use. Diabetes online communities are diverse and span a variety of social media platforms, providing clinicians opportunities to individualize recommendations for DOC use.
Keywords
Background
Diabetes is a chronic condition which is monitored and treated continuously by the person with diabetes; therefore, it is managed in a social context and ongoing support is necessary to optimize outcomes for this complex chronic condition. Family, a common source of support, can be helpful, though unhelpful behaviors (eg, nagging, controlling) have been identified. 1 Some people with diabetes (PWD) have no family for ongoing support.2,3 With the rise in social media and opportunity for social media to be a conduit and community for diabetes support, diabetes online communities (DOCs) emerged. 4 This article ascribes to the definition of an organic DOC as stated by Litchman et al,5 being a grassroots group of individuals living with or caring for someone with diabetes who gather in online spaces to interact with peers.
Diabetes online communities vary in type, function, and purpose. Some DOCs have been organically developed by people affected by diabetes, while others by professional organizations, nonprofit/for-profit organizations, health systems, and researchers. 5 Diabetes online communities traverse a myriad of online spaces, including Web sites with interactivity (eg, comments section), blogs, forums, Facebook, Twitter, Instagram, Snapchat, and TikTok, among others. Some DOCs target people with a specific type of diabetes, while others target specific age groups, gender, or language. Although not quantified, the rise in DOC use and other disease-specific online peer support communities correlates with the rise in general social media use.
The “S” in DMSES Is for Ongoing Support
The current standard of care for recognized diabetes education programs,as stated by the American Diabetes Association (ADA),is based upon diabetes self-management training, including a self-efficacy and support component called diabetes self management self efficacy (DMSES) 6 which calls for PWD to have an ongoing diabetes support plan. Peers with diabetes can address unique social support needs when compared with health care professionals (HCPs), family and friends, or community leaders. 7 Peer support can be provided via multiple venues, including attending classes and/or education visits with a PWD, participating in community support groups and DOCs. 7 A recent survey of US diabetes care and education specialists reported that one-third of respondents recommended participation in DOCs. 8 The Association of Diabetes Care and Education Specialists (ADCES) developed resources to guide clinicians on how to engage with DOCs noting the anecdotal benefits and provides a list of DOCs to explore. 9 Despite the rise in DOC research and professional organization encouragement of DOC integration as ongoing support, 10 navigation of DOCs remains a challenge and aside from suggestions to search DOC options by platform preference, 11 few resources are available for clinicians.
The overarching aim of this article is to distill the current DOC literature within the clinical context to provide insights for DOC use in the real world. We aim to provide a summary of clinical efficacy associated with DOC use and an expert opinion of application of DOC resources, based on specific needs of PWD. To accomplish these goals, we conducted a rapid systematic review of DOC studies with quantitative outcomes and an environmental scan reporting key features of DOCs to facilitate HCP navigation.
Methods
This review was conducted in two phases.
Phase 1: Rapid Review
The rapid review process was selected to meet the needs of clinicians in a timely manner and facilitate the adoption of the clinical guidelines which recommend DOC use. In addition, the literature available to review is retrospective and observational, not randomized clinical trials; thus, few of the studies would meet criteria for meta-analysis. This rapid review consisted of an initial literature search for studies establishing the association between DOC use and glucometrics (glycated hemoglobin [A1C], time-in-range, hypoglycemia), behavioral (self-care, self-efficacy), and psychosocial outcomes (quality of life, diabetes distress). Due to the limited number of publications and minimal evidence, as well as the observational nature of the evidence, this literature does not lend itself to meta-analysis. The authors agreed that a rapid review as opposed to a systematic review was appropriate for this subject, given the need for timely adoption of current ADA and ADCES guidelines indicating the benefits of using the DOC.
Eligibility criteria
We included randomized controlled trials and observational studies, in English, evaluating organic DOCs within the context of quantitative outcomes. Studies were excluded if they did not meet predefined definition of a DOC, did not review or report actual DOC use (eg, virtual remote monitoring programs and telemedicine), or if they were published in abstract form only. Reference lists of all included articles were screened for additional eligible studies.
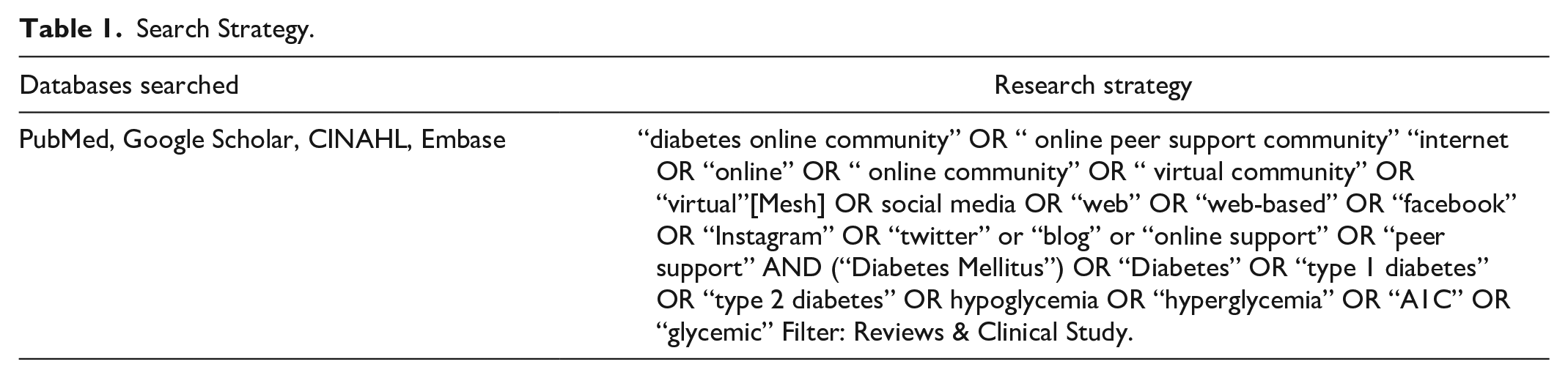
Search strategy
Following the rapid review process as described by HRQ.gov, the team followed the principles of Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations to identify all eligible studies.12,13 A medical librarian conducted the literature search (Table 1) on April 19, 2021.
Search Strategy.
Study selection
One author independently screened papers by evaluating titles and abstracts. Then, one author conducted a full-text review of all eligible papers for inclusion and data extraction. Data were synthesized across studies with critical attention to outcome measures (as seen in Figure 1).
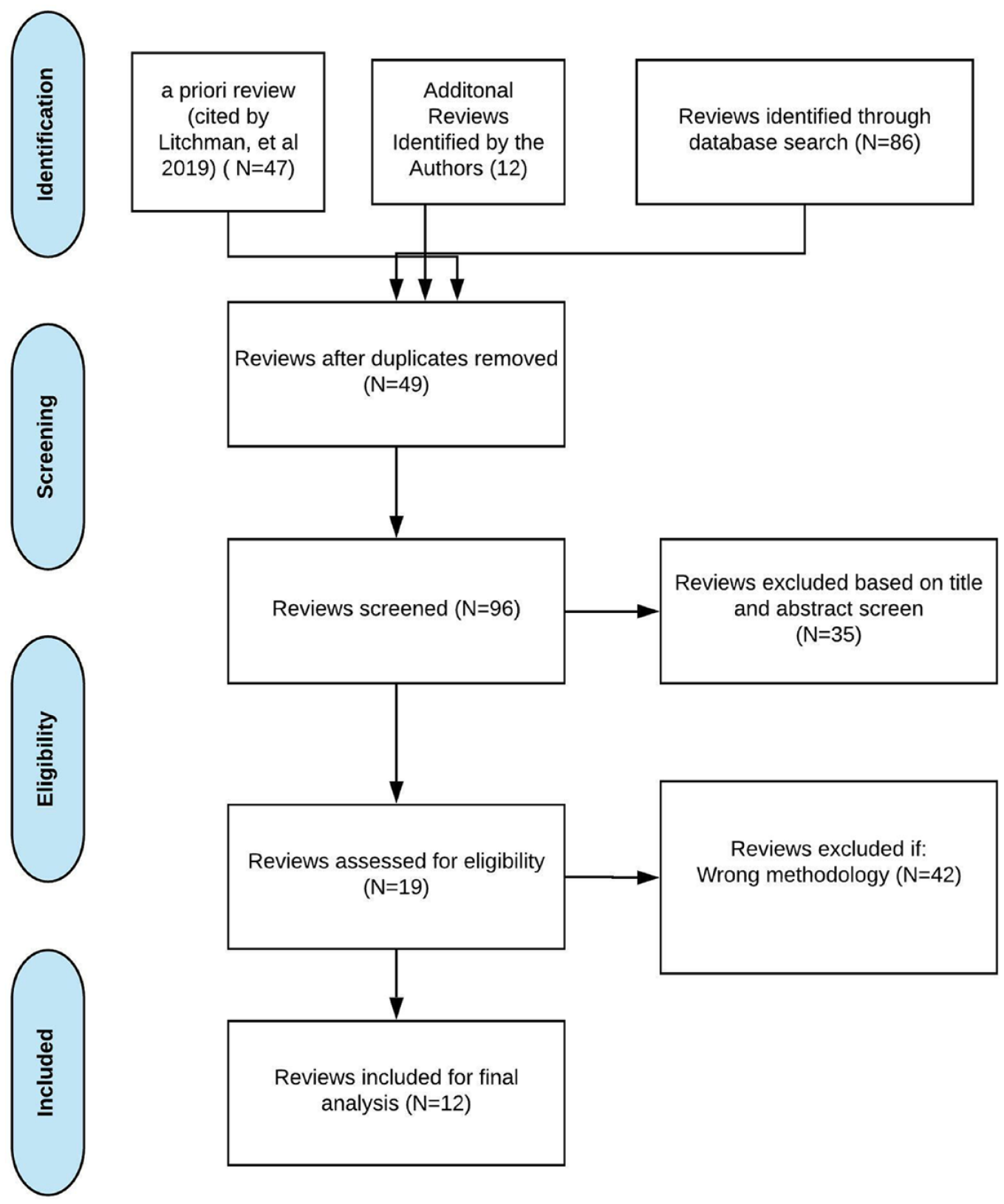
Phase 1 methods for rapid review.
Phase 2. DOC Environmental Scan
We conducted an environmental scan of a broad range of DOCs according to their key features including platform, population, subject matter, engagement, and number of followers/subscribers. The methods for phase 2 environmental scan and DOC review can be seen in Figure 2.
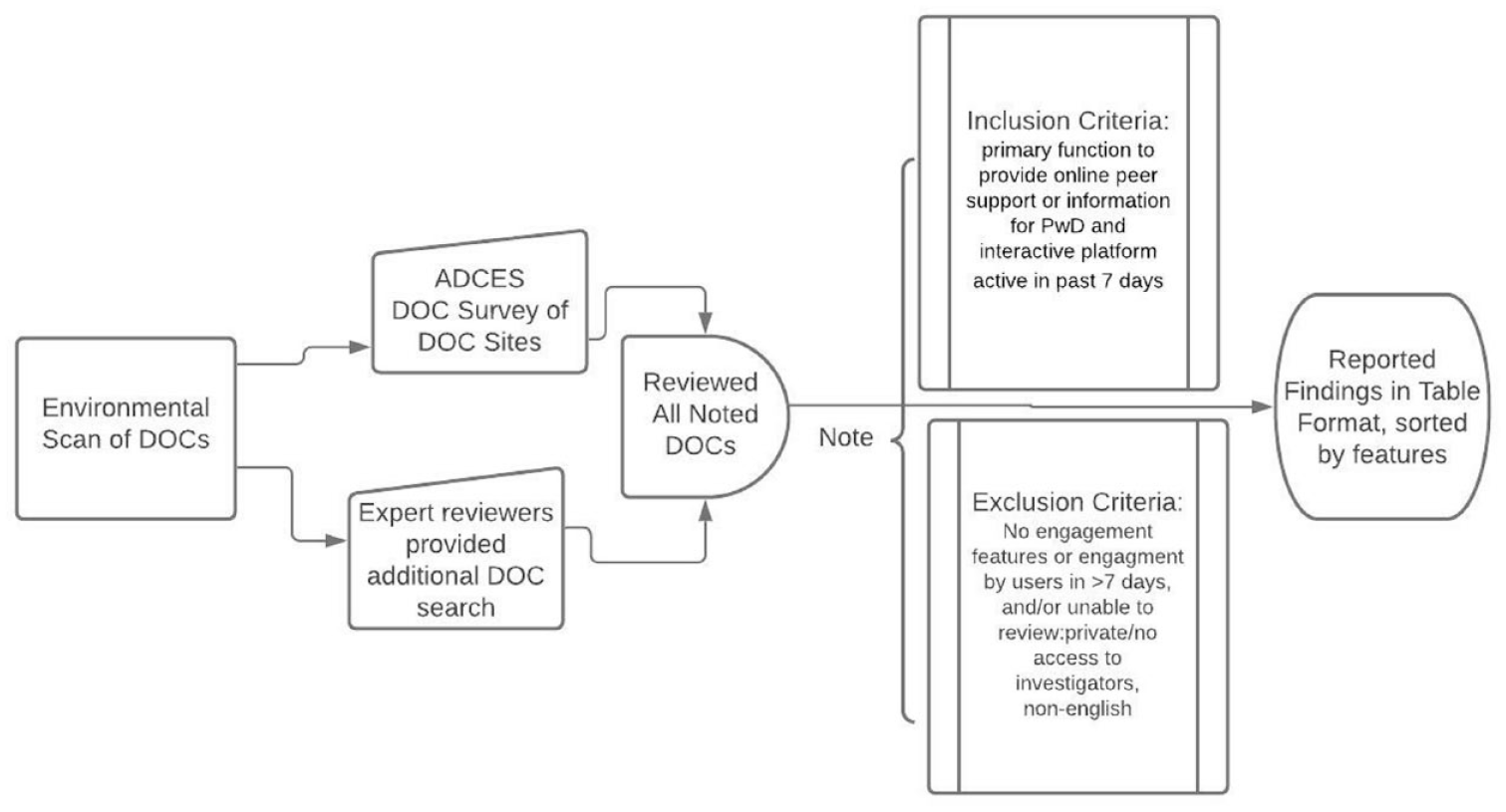
Phase 2 methods for environmental scan and DOC review. Abbreviations: DOCs, diabetes online communities; ADCES, Association of Diabetes Care and Education Specialists; PWD, people with diabetes.
Eligibility criteria
Diabetes online communities were included if they stated their primary function was to provide online peer support or information for PWD and had an interactive platform with DOC users and engagement (defined as having a viewable comment or share) within the past 7 days from site visit. Diabetes online communities which did not offer an interactive component, such as blogs with no comment section, were excluded.
DOC selection criteria
Diabetes online community platforms with posts in English were reviewed and included blogs, Facebook, Instagram, and Twitter.
Data collection
Survey data on file at ADCES from key stakeholders were initially examined. 14 The original survey was distributed in 2020 by the ADCES Peer Support Workgroup and DOC community leaders via e-mail and social media platforms. Survey respondents self-reported population served, platforms, purpose of DOC, and partnerships. Twenty-five distinct DOCs were identified for the initial review. Each author also conducted their own search to identify additional DOC sites based on research knowledge and clinical experience.
Data reporting
All DOCs meeting inclusion criteria underwent data extraction to record: social platform, population (type 1 diabetes [T1D] or type 2 diabetes [T2D], pediatric, and pregnancy in diabetes/gestational diabetes), content (information, technology, support), and number of followers. Additional information describing unique features pertinent for HCPs was also identified.
DOC quality assessment
Diabetes online community interactivity is associated with user engagement and therefore was used as an indicator of quality of DOC platforms.4-7 Bidirectional features such as comments, likes, and shares were considered interactive compared with traditional Web sites which serve as a static repository of information.
Results
Phase 1: Rapid Review
After an initial yield of 182 citations, 94 full-text articles were examined. Twelve studies meeting all criteria were included.15-26 Studies were global in nature, and included 4097 participants from the United States, China, and Europe. Study summaries are presented in Tables 2 and 3. Do-it-yourself (DIY) noncommercial, opensource hybrid closed loop systems users form a unique and homogenous DOC community, and those (eight in total) results are presented separately (Table 3). Out of four DOC studies not involving DIY users, one focused on T1D, 18 another on T2D, 15 and two studies included both T1D and T2D.16,17 All studies reported cross-sectional survey results with self-reported outcomes, with one paper comparing outcomes of two groups. 18
Characteristics of DOC Studies and Outcomes.
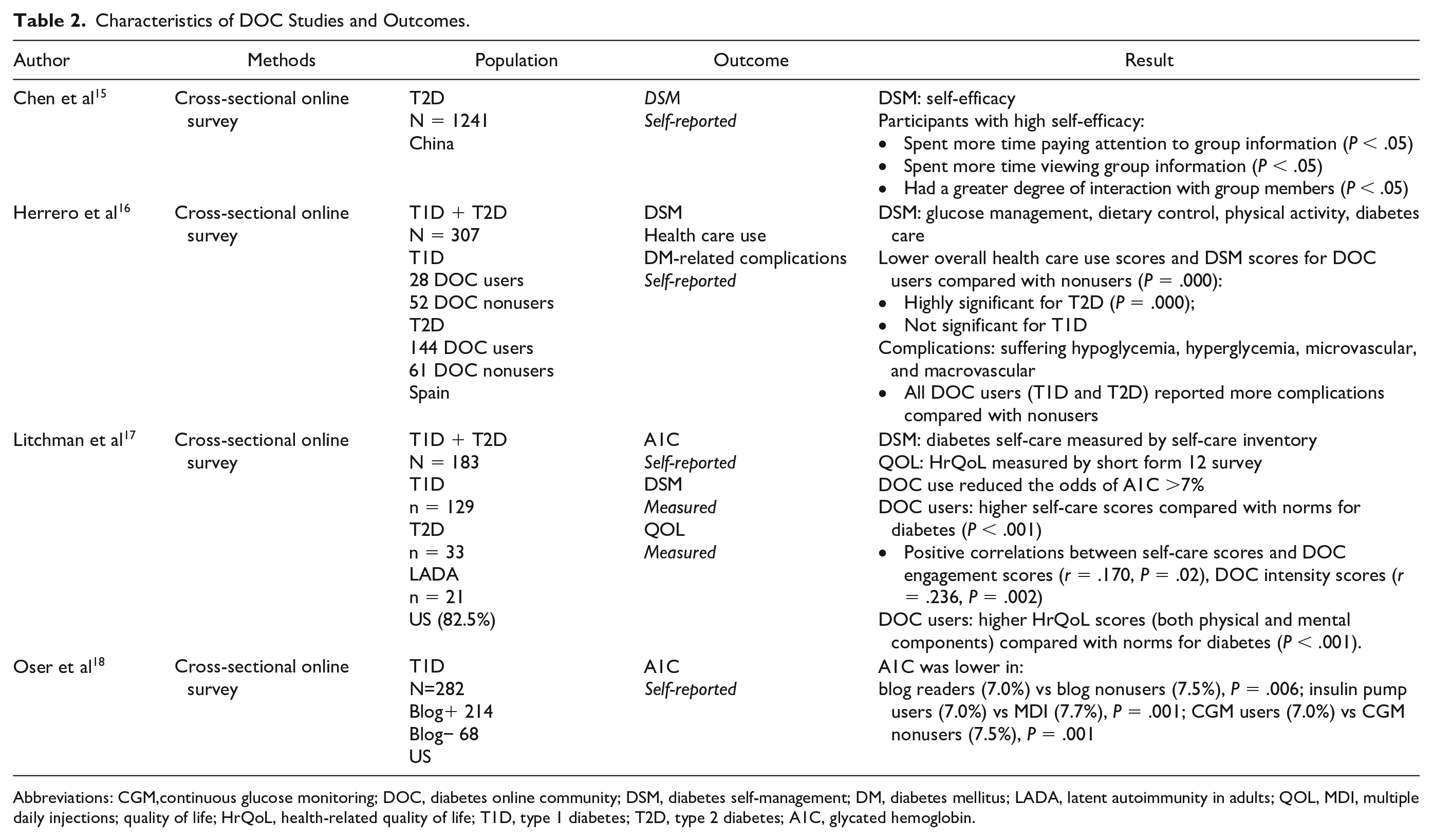
Abbreviations: CGM,continuous glucose monitoring; DOC, diabetes online community; DSM, diabetes self-management; DM, diabetes mellitus; LADA, latent autoimmunity in adults; QOL, MDI, multiple daily injections; quality of life; HrQoL, health-related quality of life; T1D, type 1 diabetes; T2D, type 2 diabetes; A1C, glycated hemoglobin.
Characteristics of DIY DOC Studies and Outcomes.
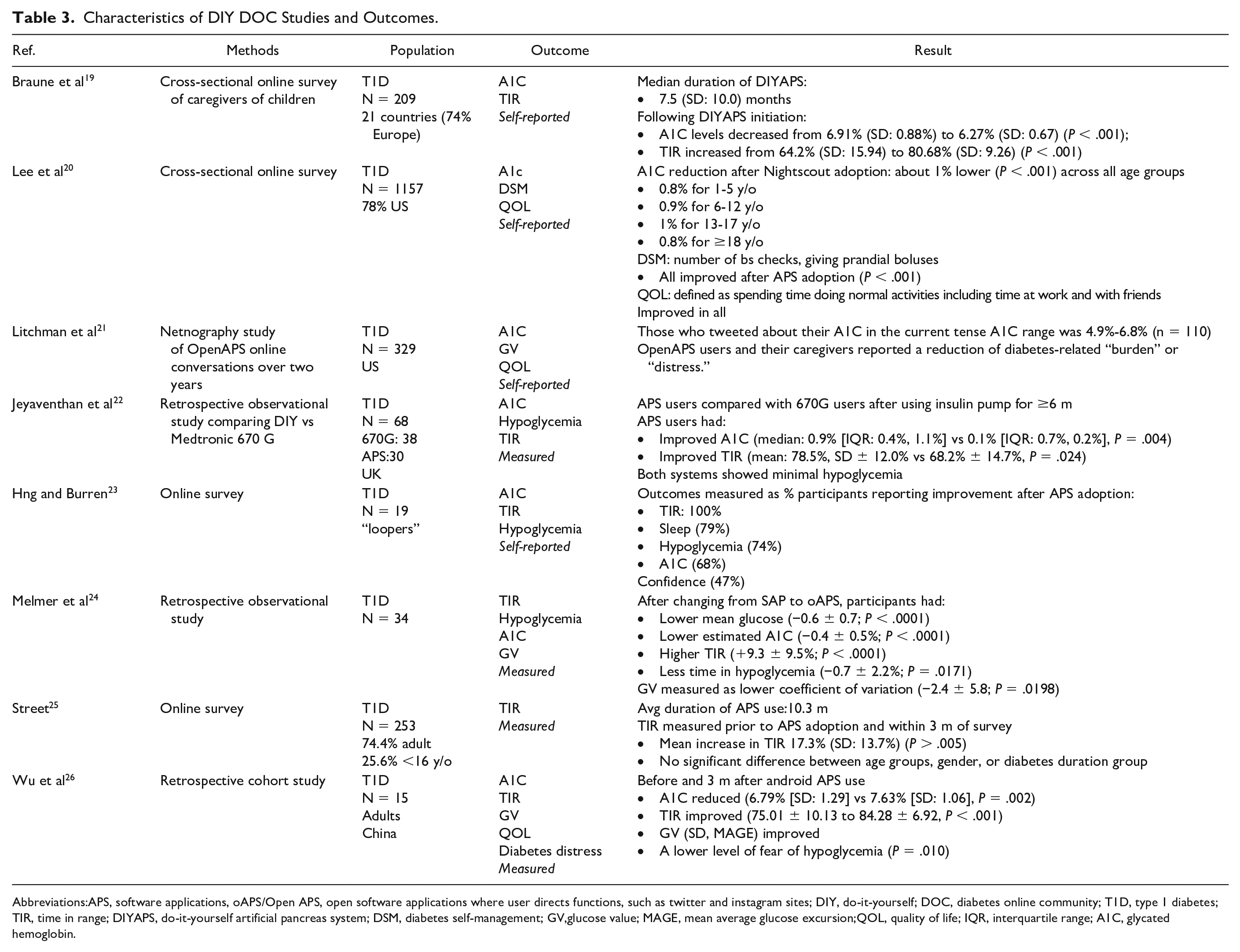
Abbreviations:APS, software applications, oAPS/Open APS, open software applications where user directs functions, such as twitter and instagram sites; DIY, do-it-yourself; DOC, diabetes online community; T1D, type 1 diabetes; TIR, time in range; DIYAPS, do-it-yourself artificial pancreas system; DSM, diabetes self-management; GV,glucose value; MAGE, mean average glucose excursion;QOL, quality of life; IQR, interquartile range; A1C, glycated hemoglobin.
Clinical outcomes
In non-DIY DOCs, two studies reported A1C results17,18 Controlling for insulin pump and continuous glucose monitor use, those who read blogs had lower A1Cs compared with those who did not read blogs. 18 Litchman et al 17 found that the significance of engagement predicted A1C by showing that people who engage with DOCs are less likely to have an HbA1c above 7%. All DIY studies reported improvement in metrics after APS adoption (Table 3). Seven reported A1C/estimated A1C,19-24, 26 six reported time in range (TIR),19,22,24-26 and three reported hypoglycemia.22-24
Behavioral outcomes
Three studies reported behavioral outcomes.15-17 In two studies, DOC use was associated with higher self-efficacy.15,17 Chen et al 15 identified that among Chinese participants, high self-efficacy correlated with positive DOC experiences (spending more time paying attention to group information, viewing group information, and having a greater degree of interaction with group members, all P < .05). In the Spain-based study, Herrero et al 16 found that participants with T2D but not T1D, who used DOCs, had lower diabetes self-care levels compared with those who did not use DOCs and reported a higher degree of diabetes-related complications. Conversely, Litchman et al 17 found that DOC use (engagement and intensity) among participants with T1D, T2D, and latent autoimmunity in adults (LADA) (combined in the analysis) was associated with higher self-management scores when compared with diabetes norms.
Psychosocial outcomes
Quality of life (QOL) was examined in four studies, three out of those in DIY users. Instruments for QOL assessment varied between studies and included health-related QoL (HrQoL), 17 self-assessed QOL including the ability to spend time doing normal activities, 18 self-described reduction in diabetes-related burden or distress, 21 or measured hypoglycemia fear scale, and diabetes distress scale. 26 Higher quality of life was identified in DOC users when compared with population norms 17 Three DIY-dedicated DOCs studies reported improvement in QOL20,21,26 and one reported improvement in diabetes distress, and fear of hypoglycemia after APS adoption. 26
Results of Phase 2: Identify and Describe Key Features of DOCs to Facilitate HCP Navigation
An internal environmental scan survey administered by ADCES from November 8, 2020, to December 22, 2020, received responses from 25 DOC group leaders (data on file). 14 Of those, seven were omitted from final review due to the noninteractive nature of platform not meeting study definitions of a DOC, leaving 18 for comprehensive review. Authors identified additional 29 DOC sites by cross-referencing survey site platforms and cited partners. After condensing DOCs with a presence on multiple platforms and eliminating noninteractive DOCs, a total of nine DOCs were added to the original list of 18. A total of 27 DOCs were included and the reporting of the DOC characteristics resulted in a DOC taxonomy (Table 3).27-53
Only one DOC had a blog with interactive features consistent with other DOC platforms. 38 While 21 DOCs are housed on more than one platform, Facebook had the most followers on 14 of the 27 DOCs. Instagram dominated on four DOCs and Twitter dominated on one DOC. Moderator functions are available to DOCs using the Facebook platform only, where 3 of the 19 DOCs appeared to be using moderators.32,36,48 Content of DOCs varied. Two were solely technology focused32,53 2 were support focused,34,41 2 were information focused,28,45 and the remaining 22 sites were focused on more than one content area. Several subtopics were observed within the scope of the information, support, and technology content areas, including diet, exercise, new diagnosis of diabetes, maturity-onset diabetes of the young, LADA, and gender and minority perspectives.
Discussion
This article builds upon a previous scoping review, adding a narrow focus on quantitative metrics, and is the first, to our knowledge, to comprehensively review DOCs for content and target population for the purposes of facilitating HCP utilization. 5
While our results are encouraging, overall, there is a paucity of information on the impact of DOC use. Data support an association between DOC use and improved clinical outcomes. DOC use may offer a mechanistic pathway for improving self-efficacy, however, as suggested by Chen et al, 15 may relate to the end-user experience. In an analysis of an in-person peer support intervention, self-efficacy was associated with both reduced diabetes distress and improved glycemic outcomes 9 and future DOC research should assess for these outcomes. The association between self-management and DOC use is unclear and warrants further examination based on diabetes type, presence of complication, and country of origin. While evidence indicates most DOC users report DOCs are helpful with minimal harm, qualitative findings suggest stigma-based infighting between those with T1D and T2D may impact experiences of DOC users.54-56 Future studies should determine how DOC engagement, both positive and negative experiences, impact diabetes outcomes. Specific to DIY-related DOC use, reported outcomes may reflect participant self-selection, who were highly motivated and meeting diabetes targets prior to DOC and/or DIY adoption. 17 Improvements in glycemic outcomes were impressive due to good control at baseline; it is unknown if similar improvement in outcomes would be achieved in a cohort with poorly controlled diabetes.
As DOCs are available on singular and multiple platforms across the social media spectrum, the question is raised if one platform offers distinct advantages over another. Oerum 11 noted that various platforms meet different user needs and preferences and recommends that users determine DOC choice by platform and then content as a secondary choice. Many DOC sites are centered on a Web site blog, linked to multiple platforms, such as Facebook, Instagram, and Twitter, and therefore serve as a hub to facilitate DOC engagement. In addition, blogs have helpful topic searches and other engaging elements including posting popular search topics. Some DOCs post unique content on various platforms, though most share the same content across all DOC platforms.
Another question of importance is what is the role of DOC within other support systems and what is the optimal way to utilize them. Diabetes self-management and support (DSMES) provided by certified diabetes care and education specialist is a standard of care. 10 Although evidence indicates most DOC users continue to see their diabetes clinician regularly and trust their diabetes clinician more than content found in DOCs, how DOC use relates to formal DSMES programs attendance is unknown. 57 It is possible that DOCs supplement DSMES, but for some, the information found on DOC platforms may be in lieu of formal DSMES. In addition, some PWD are seeking content they do not receive in the clinical environment, along with an alternative platform and peer-to-peer delivery. Diabetes online communities offer easy access to ongoing support for PWD. In related diabetes lifestyle clinical interventions, support was found to be a contributing factor influencing adherence to change in addition to psychosocial outcomes.5,57 Furthermore, it would be valuable to have a validated tool to identify patient DOC support needs. Community Advisory Boards (CABs) are relevant in developing research questions and tools for PWD. Many studies did not use CAB, and therefore have selection bias; hence, questions are biased to clinician perspective.
Gap in Translation to Clinical Practice
There remains a disconnect between recommended resources on ADCES and what patients want from DOC resources. Clinicians/Educators take part in DOCs but rarely (one in three) recommend DOC to PWD.
Currently, there is more evidence for use of DOCs in T1D populations than T2D populations.7,57 Some T2D populations report negative experience with DOCs, likely related to a mismatch of population and content, and therefore, an HCP should recommend T2D content focused DOCs.
Limitations
The rapid review is not without limitations. Studies had major limitations inherent to their cross-sectional cohort design and self-reported outcomes and only show associations with outcomes and not causation. Notably, there were no longitudinal prospective observational studies or randomized control trials.
Glycemic outcome review is limited by the paucity of evidence. Despite the rise in DOCs, funding for DOC research is scarce and necessary to develop more robust examination of how DOC use impacts clinical, behavioral, and psychosocial quantitative outcomes.
We also acknowledge that the goal of making a current, complete, and inclusive list of DOCs may be impossible to achieve. By nature, the DOC is ever-changing and there are likely thousands of mini-DOCs in the United States alone. Searching keywords such as “diabetes” in Facebook, for example, generates a plethora of public and private communities. Because an exact number is not given, it would be exceedingly difficult to calculate. Platforms, including Reddit, Snapchat, WhatsApp, and TikTok, were not included due to platform-specific privacy restrictions which were prohibitive for reviewers. This review is limited to published literature, social media searches, and inextricable bias of personal experience of English-speaking diabetes specialist authors, and the phase 2 environmental scan survey was self-reported by DOC members. Due to this gap in representation of specific communities, sites were likely missed.
Clinical Considerations for Prescribing DOCs
Based on our findings and the findings of others, there are ten factors that clinicians should consider when prescribing DOCs. 12
Privacy. While some DOCs are private, others are public. People with diabetes must understand the differences before sharing personal health information in DOCs.
DOCs are dynamic. The composition and content of DOCs are ever-changing, and therefore, DOC navigation may present challenges for new and veteran users as well as clinicians trying to prescribe a particular site.
Pace: Some DOC sites move faster than others. For example, the #DSMA twitter chat, which has occurred every Wednesday evening at 9 PM ET since July 2010 is fast paced, while asynchronous platforms (eg, Facebook) are much slower in pace.
Commercialization. Commercial sponsors and opportunists for-profit may permeate some DOCs. People with diabetes seem to have little circumspection toward these sites, as evidenced by number of followers.
Quality of DOC Information. While diabetes misinformation does exist online, rates of misinformation is low within DOCs and users continuously “self-police” to improve the quality of information shared among users.
Cyberbullying. Diabetes online community infighting has been described. Those with T2D may be especially at risk due to higher rates of social stigma.
Access. Due to limited Internet access, language limitations of DOC sites, or other factors, DOCs may not be accessible. While this review is limited to English only, there are DOCs in multiple languages.
Attitudes: Not all PWD need or desire DOC use. Some PWD may have negative experiences with previous social media use or may not be interested learning about the experiences of others with diabetes.
Content: May be broad or focused. Diabetes online communities may be multitopic and have search engines (Facebook, blogs) or may be focused on one topic (eg, exercise or low carb diet). While a range of topics, which present in a Twitter or Instagram feed, may be engaging for an experienced PWD, diverse content may be overwhelming for a newly diagnosed PWD who might prefer a blog format with search engine to navigate specific areas of interest.
Culture. Finding the right fit to a DOC is important; we noted groups focused on a particular gender, ethnicity, age group, or lifestyle interest. Poor culture fit may negate benefits of DOC participation.
Tailoring your DOC recommendation to the PWD’s individual needs is encouraged. Using Table 4 as a guide, clinicians should consider the type of platform, type of diabetes, and preferred content the patient will benefit from. See Table 5 for detailed recommendations.
Diabetes Online Community Sites.
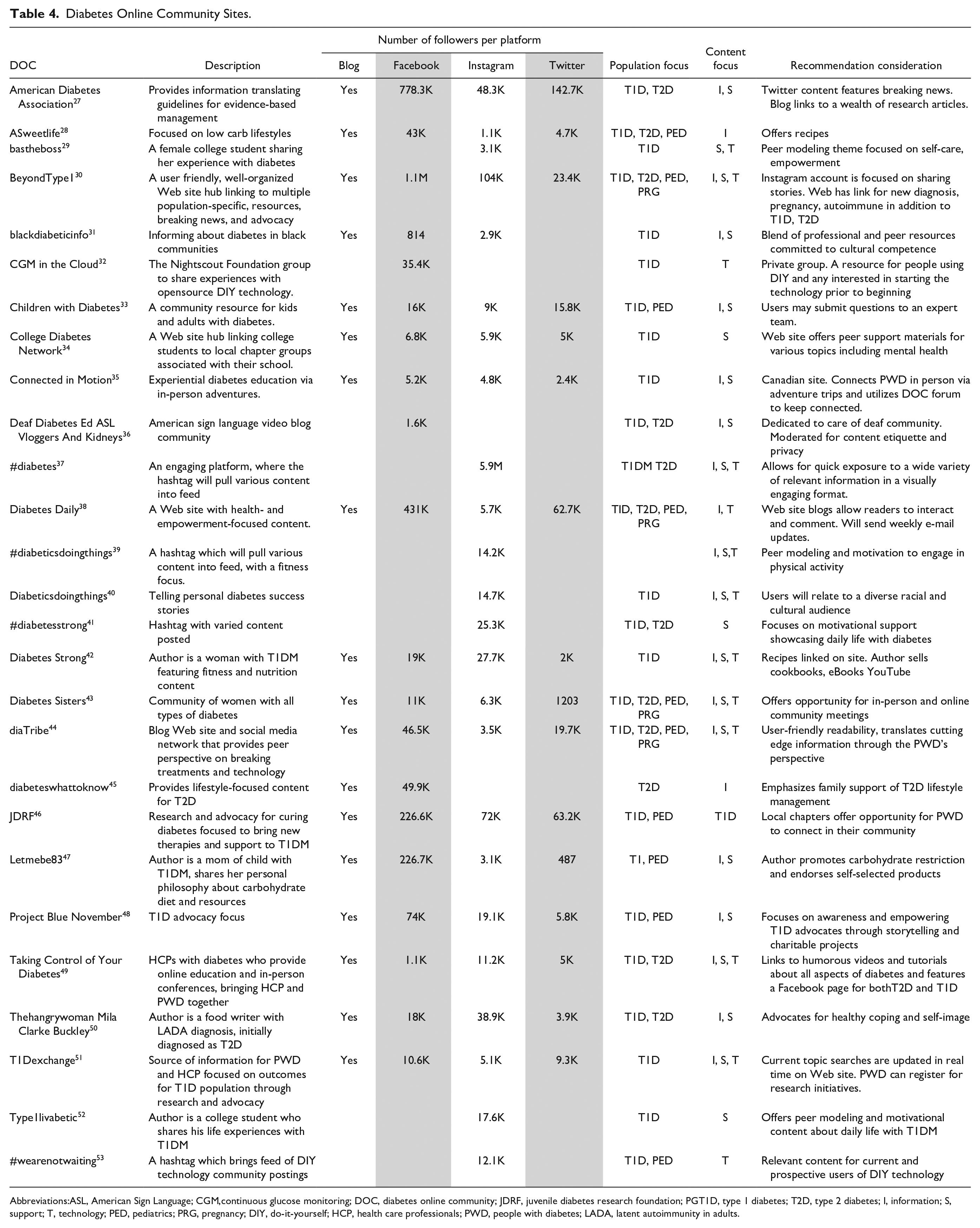
Abbreviations:ASL, American Sign Language; CGM,continuous glucose monitoring; DOC, diabetes online community; JDRF, juvenile diabetes research foundation; PGT1D, type 1 diabetes; T2D, type 2 diabetes; I, information; S, support; T, technology; PED, pediatrics; PRG, pregnancy; DIY, do-it-yourself; HCP, health care professionals; PWD, people with diabetes; LADA, latent autoimmunity in adults.
Recommending a Diabetes Online Community for People Affected by Diabetes.
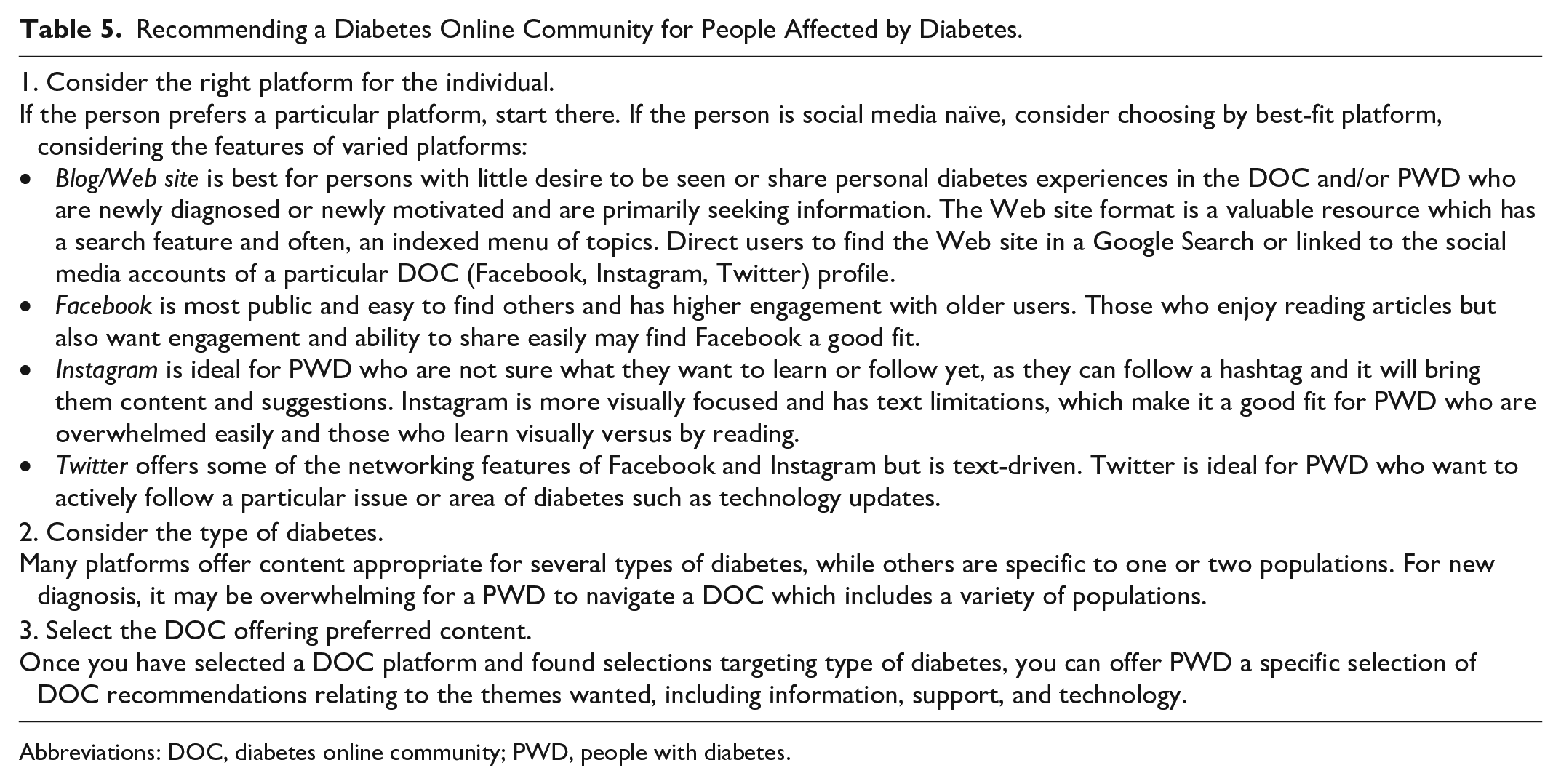
Abbreviations: DOC, diabetes online community; PWD, people with diabetes.
Conclusion
The DOC serves as a no-cost, 24 hours a day resource for PWD and their families. The use of DOCs for PWD may lead to improved glycemic, behavioral, and psychosocial outcomes. Thus, engagement in DOCs can be recommended for PWD and their families. Choosing the optimal DOC that would meet the specific need of a PWD remains a challenge. Health care professionals are encouraged to promote and prescribe DOCs for PWD using Table 4 as a guide to individualize referrals. More research is needed to determine the scope of benefits and best-fit features for varying diagnosis and other conditions of diabetes. The mechanism by which DOC use may lead to improved outcomes warrants more study. Funding opportunities focused on studying DOC outcomes and clinical integration are needed to support this gap in research.
Footnotes
Acknowledgements
Thank you to the Association of Diabetes Care and Education Specialists (ADCES) for contributing diabetes online community survey results from the ADCES Peer Support Workgroup 2020.
Abbreviations
A1C, glycated hemoglobin; ADA, American Diabetes Association; ADCES, Association of Diabetes Care and Education Specialists; CAB, Community Advisory Boards; DSM, diabetes self-management; DSMS, diabetes self-management and support; DIY, do-it-yourself; DOC, diabetes online community; HCP, health care provider; HrQoL, health-related quality of life; I, information; LADA, latent autoimmunity in adults; PED, pediatrics; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PWD, people with diabetes; QOL, quality of life; S, support; T, technology; T1D, type 1 diabetes; T2D, type 2 diabetes; TIR, time in range.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.