
Abstract
Introduction:
Diabetes mellitus technology (DMT) is increasingly used for routine management in developed countries, yet its uptake in developing countries is not as consistent. Multiple factors may influence this, including country specific patient perception regarding DMT. We conducted a pilot study in Pakistan to understand this important question which has not been studied yet.
Methods:
A cross-sectional pilot study was conducted in Pakistan. An anonymous survey exploring perceptions of diabetes technology was circulated on social media platforms, collecting responses over 2 weeks. Target population included adults (≥18 years) living in Pakistan, with DM1 or 2.
Results:
A total of 40 responses were received. The majority (36/40) reported using conventional glucometers. Nine used continuous glucose monitoring (CGM). Thirty-two of 40 patients believed DMT improved diabetes care, 22 felt it helped decreased risk of Diabetes-related complications. 15/40 stated that DMT results in increased cost of care. Sixteen reported their diabetes care teams had never discussed wearable DMT options whereas 11 disliked them because they did not want a device on their self.
Conclusion:
In our pilot study we have identified broad themes of opportunity and challenges to DMT use in Pakistan. Patients’ perceptions regarding DMT were generally positive but significant barriers to its acceptance included high cost, lack of discussion between doctor and patient about available technology and personal hesitation. Limitations of our study include sampling bias (online survey) and small sample size, but this data can help inform larger studies, to look at this important topic in greater detail.
Introduction
Diabetes Mellitus (DM) affects approximately 382 million individuals worldwide,1,2 75% of whom live in low- and middle-income countries like Pakistan.3,4 Intensive glycemic management has demonstrated reduced risk of some of the DM associated complications. A major challenge with aggressive glycemic control is the increased risk of recurrent and severe hypoglycemia. 5 Patients with DM on insulin therapy are instructed to check their blood sugars frequently; the information from self-monitored blood glucose (SMBG) monitoring helps guide diabetes medication and insulin dose adjustments. 6 However, fingerstick glucose monitoring is painful and tedious, and often most patients are unable to check their glucose levels as often as instructed. 7
Technology has heralded the development of innovative digital health devices for chronic diseases 8 including DM care. Since the commercial availability in late 1970s of continuous subcutaneous insulin infusion (CSII), commonly known as insulin pumps,9-11 DM technology continues to evolve. Continuous glucose monitors (CGM) have increasingly become more available and affordable. 12 CGMs sense and record glucose levels in the interstitial fluid with newer models able to alert patients to high/low glucose values. Studies report a reduction in HbA1C of (⁓0.5%) from baseline levels >7.5%, as well as a reduction in frequency and severity of hypoglycemic events, with the use of CGM in adults with Type 1 DM.13,14 CGMs linked to CSII allow for automated adjustment in subcutaneous insulin delivery doses every 1-15minutes. 15 Such closed loop systems with automated decision-making are approved for use in most of the developed world and some developing countries. However, costs associated with CGM devices remain high, and are a barrier to implementation in lower-middle-income countries (LMICs) like Pakistan.
Adaptation to DM technology has seen challenges worldwide 16 with different factors impeding the adoption of electronic devices; including time-consuming data entry, data loss/errors, anxiety toward a new device, user-friendliness and costs. Age is among the most important factors affecting technology acceptance.3,17 It is important to recognize patients’ perceptions within the context of rapidly advancing technology, to possibly design user-friendly future health interventions.3,17 Several research groups have explored barriers to diabetes technology use in adults with diabetes but most of this data originates from developed countries and regions with different socioeconomic parameters. Pakistan, with its unique set of socioeconomic challenges, a low literacy rate, a high burden of DM and a unique demographic; where the majority (64%) population is younger than 30 it is essential to understand the local context of perceived barriers to diabetes technology.
There is limited information about patient perceptions regarding diabetes technology in developing countries, particularly South Asia where there is a high burden of DM. Our pilot survey aims to understand these perceptions among patients with both type1 and type 2 DM in Pakistan 18 as DM technology providers begin to expand in the local market. This enhanced understanding of the patient perspective could help design interventions to effectively increase the utility of DM technology in LMICs.
Methodology
Study Setting and Participants
This cross-sectional study was conducted by the Department of Medicine, Aga Khan University Hospital, Pakistan, after acquiring due approval from the institutional review board. An anonymous survey self-designed by the research team consisted of 14 questions spanning over 3 sections for demographics, glycemic control, understanding and perceptions of diabetes technology, and a section for open responses (Appendix). The target population included all adults (≥18 years) in Pakistan with a known diagnosis of T1DM or T2DM.
Data Collection
Prior to dissemination, the survey was pre-tested on 5 adult individuals with DM, and ambiguous questions were either omitted or rephrased. This final survey was disseminated via Google Forms on different social media platforms, such as Facebook and Twitter, and via snowball sampling. An online method of data collection was chosen to abide by the conditions of ethical clearance received by the institutional review board which allowed only virtual data collection due to the risks of physical interaction during the ongoing COVID-19 (coronavirus disease 2019) pandemic. Online data collection also enabled a wider reach for survey dissemination. The Google Forms survey was preceded by a consent form (Appendix). To ensure accurate respondent inclusion, the survey was also preceded by screening questions recording participants’ age, diagnosis of T1DM and T2DM, and country of nationality and residency. This ensured that only adult patients who were diagnosed with DM and of Pakistani nationality and currently residing in Pakistan were included in the study. Patients who were excluded on the basis of the screening questions were automatically directed to the end of the form and their responses were not recorded. The survey was disseminated across all platforms for a total of 4 times (every 5 days over the course of 15 days) and dissemination was ceased when no additional responses were recorded after the fourth cycle of dissemination.
Statistical Analysis
Quantitative data was analyzed using IBM Statistical Package for Social Sciences Version 21.0. Descriptive statistics were presented as frequencies and percentages for categorical variables.
Qualitative analysis of the responses received to the open-response sections was performed via thematic grouping of responses and reporting frequencies of responses under major themes. Two authors were primarily involved in qualitative analysis. Both individuals had previous experience with qualitative analysis, specifically thematic grouping, for prior research projects. A third member of the research team initially de-linked the open-ended responses from the rest of the responses to the questionnaire and provided these anonymized open-ended responses to the 2 authors. After an initial familiarization with the content of the responses, the following steps were then followed:
Translation of Text in Roman Urdu: One respondent had provided their open-ended responses in Roman Urdu (Urdu language written with the Latin script). Since the Urdu used was simple and both authors possessed native level expertise with Urdu, these responses were translated to simple English. This was performed independently by the 2 authors, and their translations were compared and synthesized to produce English translations that were unanimously accepted by the research team. The English translations of these responses were used for qualitative analysis.
Finalizing of Responses Set: Prior to beginning thematic grouping, both authors first independently determined which responses were suitable for inclusion for qualitative analysis. Pre-decided bases for elimination of responses to open-ended questions were if the responses contained no words (such as “-” or “.”) or if they indicated an unwillingness to respond (“No comment”). There was no minimum length of responses for inclusion, as even one-word responses conveyed valuable opinions regarding DM technology (“Helpful,” “Good”). Excluded and included responses were then compared by the 2 authors. Differences were settled by discussion with the complete research team. Thematic analysis was performed on the finalized set of responses.
Identification and Finalization of Themes: The 2 authors independently proceeded to identify possible themes within which to categorize responses. There was no limit on the number of themes to be identified. These were then compared by the 2 authors among themselves and jointly discussed. After synonyms were accounted for, themes concerned with related constructs were combined (eg, “DM technology is too expensive” and “Patients cannot afford DM technology” were combined to “High Costs”). Disagreement was settled by discussion with the corresponding author. After joint consensus, a set of themes were finalized.
Categorization of Responses: The 2 authors independently grouped responses under the finalized themes. If the same respondent provided multiple statements that could be categorized within more than one theme, the concerned statements were included under multiple themes. Responses not falling under any theme were categorized as “Other.” These thematic groupings were then compared by the 2 authors and differences were settled by discussion with the complete research team. This finalized categorization of themes was included in the manuscript.
Frequency of Responses under Theme: In order to provide context regarding the recurrence of each theme, the number of responses categorized within a theme were also expressed as a percentage of the total number of responses.
Results
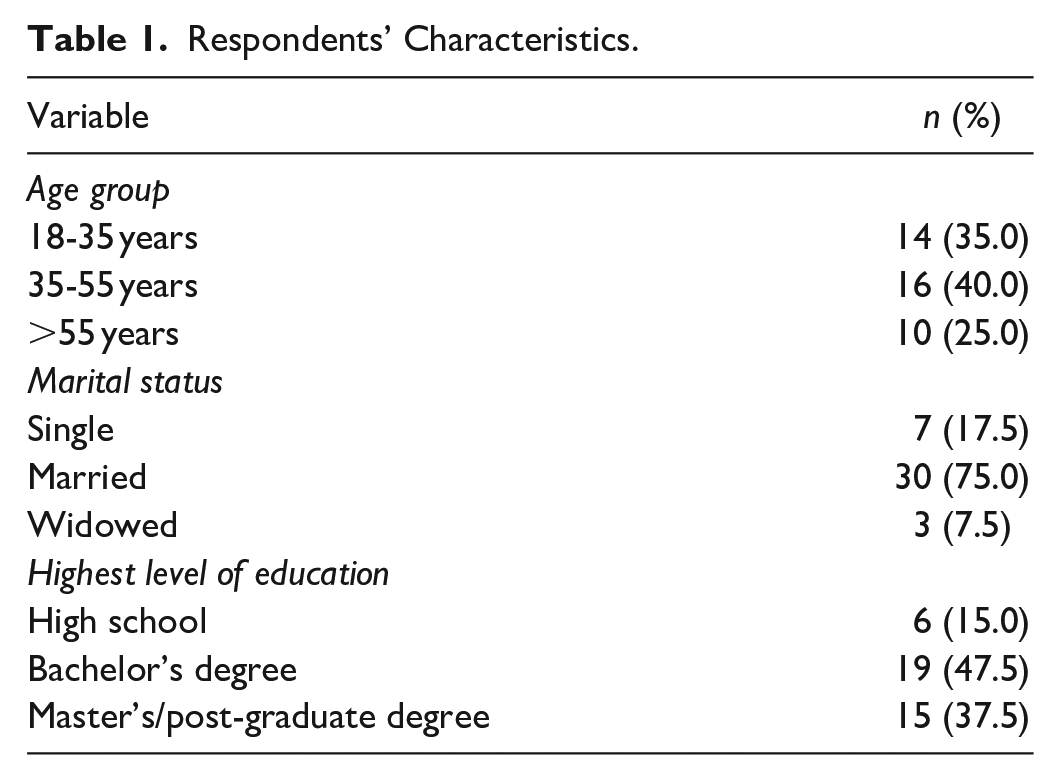
A total of 40 patients with diabetes mellitus (DM) responded to our pilot survey. The greatest percentage of respondents were aged between 35-55 years (n = 16; 40%) and married (n = 30; 75%). Almost half of the respondents (n = 19; 47.5%) reported having a bachelor’s degree as their highest qualification. Demographics are shown in Table 1.
Respondents’ Characteristics.
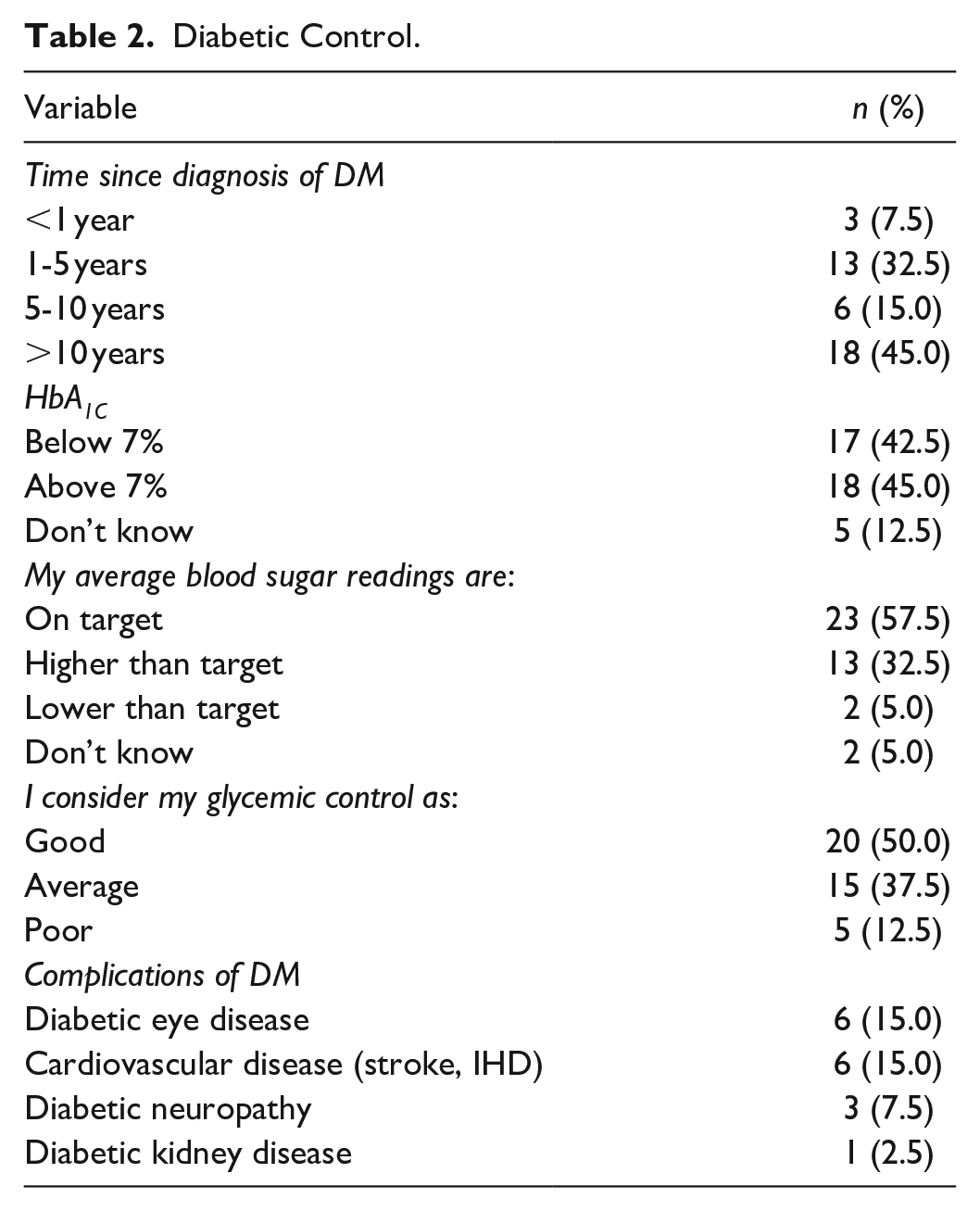
The greatest percentage of respondents reported having been diagnosed with DM over 10 years ago (n = 18; 45%), followed by 1-5 years (n = 13; 32.5%). Around 45% (n = 18) of respondents reported having an HbA1C >7%, and 32.5% (n = 13) felt that their average blood sugar readings were higher than their target. Only half (n = 20; 50%) of respondents felt that their glycemic control was good, and common reported complications of DM included diabetic eye disease (n = 6; 15%), cardiovascular disease (n = 6; 15%), and diabetic neuropathy (n = 3; 7.5%) (Table 2).
Diabetic Control.
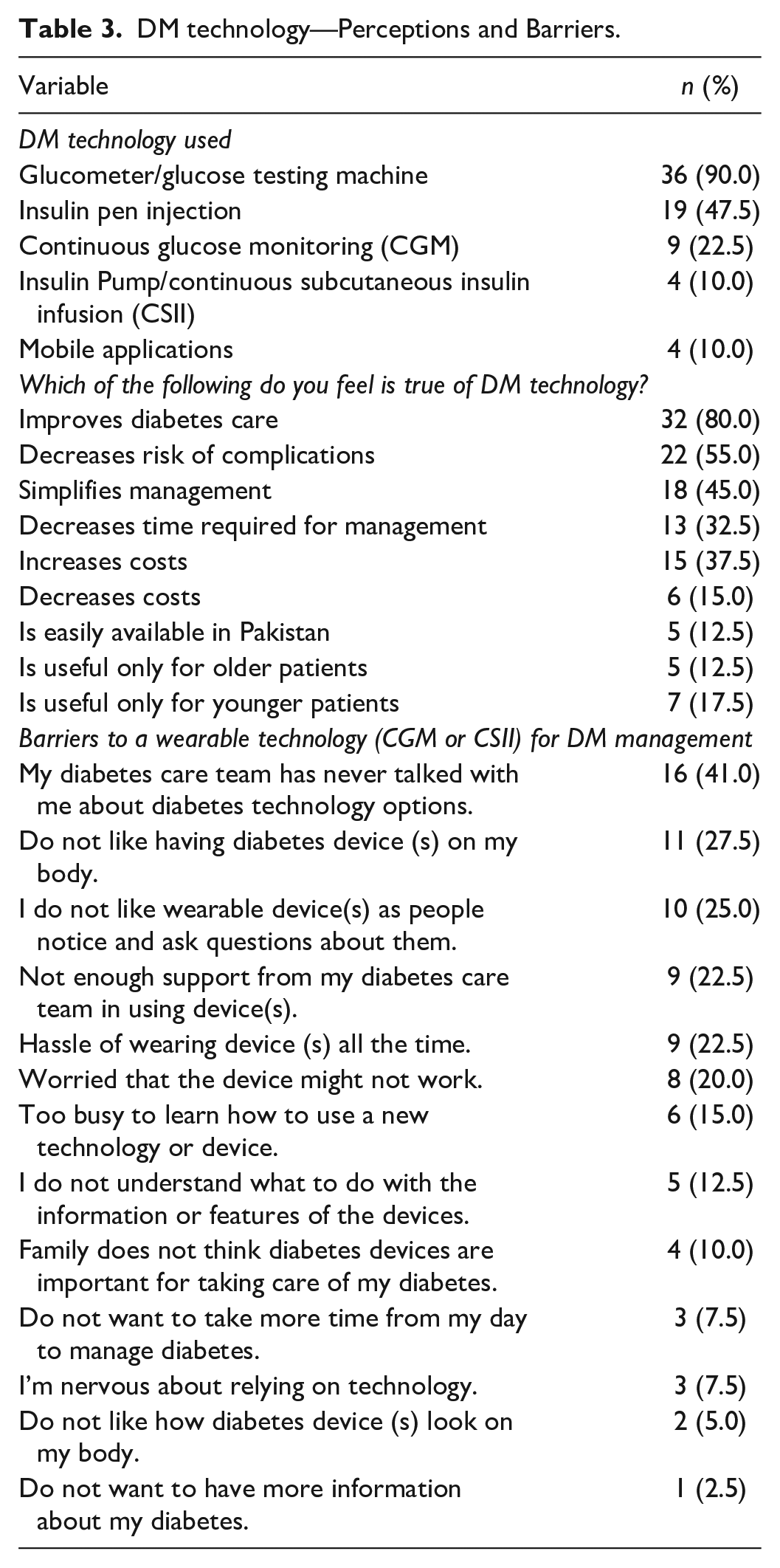
The most common DM technology used by respondents was fingerstick glucometers (n = 36; 90%), followed by insulin pen injections (n = 19; 47.5%). Most respondents felt that DM technology improves diabetes care (n = 32; 80%) and decreases the risk of complications (n = 22; 55%). However, only 5 (12.5%) respondents felt that DM technology was easily available in Pakistan, and 15 (37.5%) felt that it increased costs of DM management. The commonest barriers to a wearable technology (CGM and CSII) were that patients’ diabetes care teams had never discussed wearable technology as management options (n = 16; 41.5%), patients did not like having a wearable DM device on their bodies (n = 11; 27.5%), and that patients did not like wearable DM technology due to the attention they attracted from other people (n = 10; 25%). Perceptions regarding DM technology and barriers to wearable DM technology are shown in Table 3. Of the total respondents some DM patients may not have been on insulin and on oral diabetes agents alone.
DM technology—Perceptions and Barriers.
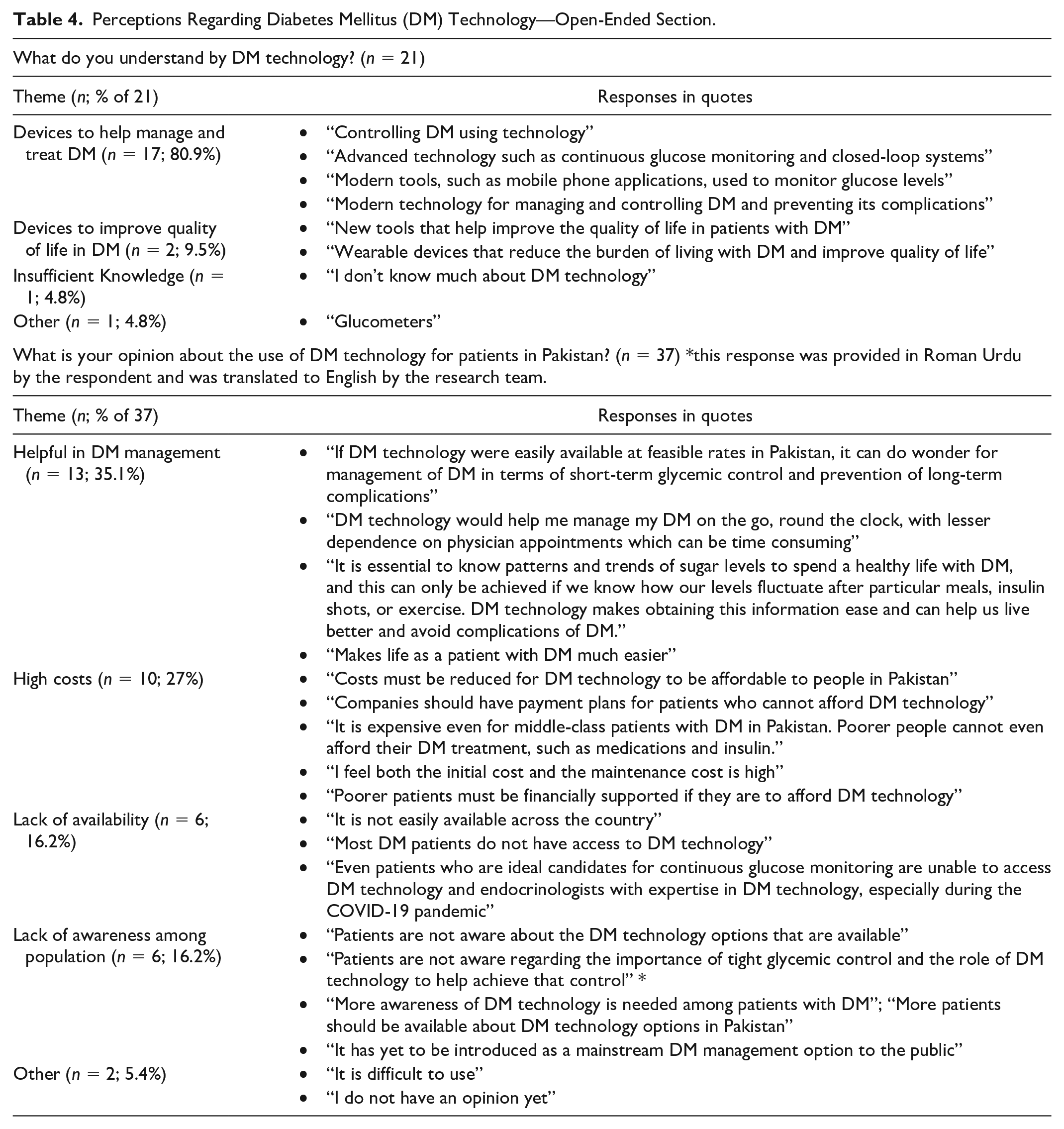
Thematic analysis of the open-ended response sections revealed that while respondents did possess an understanding of DM technology and its potential to optimize diabetes management and improve quality of life, they were also cognizant of several barriers to the use of DM technology in Pakistan, such as high costs, lack of availability, and lack of awareness among the population (Table 4).
Perceptions Regarding Diabetes Mellitus (DM) Technology—Open-Ended Section.
Discussion
Our pilot survey intended to explore the usage and perceptions of DM technology among patients with Diabetes (all types) in Pakistan. The average annual income in Pakistan is approximately US$420, and 35% of the population lives below the international poverty line (World Bank data). The cost of a 14-day use CGM sensor is approximately $77, an insulin pump approximately $700 and monthly supplies are separate. Insulin is widely available in the urban areas of Pakistan, at a cost ranging from $12 per 10 ml vial or 6-8$ per 3 ml pen. Access to health care and pharmacies is limited in far flung and rural areas many of which also do not have electricity available. The mean annual direct cost per patient with diabetes was estimated to be 332 USD in a previous study. 19 Medications accounted for the largest share (60.4%) of this cost.
Among a total of 40 respondents, the majority (90%) reported using the conventional method of monitoring blood sugars, which comprises of finger prick and glucose strip testing using glucometers. 22.5% of patients used continuous glucose monitoring (CGM), and 10% used insulin pumps and mobile applications. While most patients believed diabetes mellitus technology improves diabetes care (80%) and decreases the risk of diabetic complications (55%), barriers to use included high-costs, lack of availability, and lack of awareness.
Despite few respondents using DM technology such as CGM (22.5%), the perceptions regarding DM technology were largely positive among respondents overall. The majority stated that DM technology improved diabetes care (80%), decreased risk of complications (55%) and simplified management (55%). Thematic analysis revealed that respondents felt that DM technology could help improve quality of life in patients with DM. Studies from developing countries confirm these positive perceptions, as DM technology undoubtedly improves health outcomes, and is also increasingly being found to improve quality of life among patients. 20
Most importantly, our pilot survey highlighted several important barriers to the use of DM technology in Pakistan. The high costs associated with DM technology was a common theme in the open-ended section of our survey (Table 4). Moreover, 37.5% of respondents felt that DM technology increased the costs associated with diabetes care. In LMICs like Pakistan, where patients with DM are frequently from non-affording backgrounds and most healthcare costs are met out-of-pocket, affordability stands out as a major barrier to the use of DM technology. The availability of DM technology across the country is very limited, possibly due to multiple factors, including cost. This lack of availability was also identified as a barrier to use of DM technology by respondents. (Table 4). In Pakistan, other technology such as smart phones, computers, television are available in short installments, including the only currently available insulin CSII/pump in the market, a comment related to this was made by one respondent (Table 4).
With regards to wearable DM technology devices, which include CGM and CSII, respondents had additional concerns. Most commonly, respondents reported that their diabetes care teams had not discussed the options of wearable devices with them (41%). Moreover, 22.5% reported that they did not receive enough support from their diabetes care team in exploring wearable devices as options. Although diabetes education is the cornerstone of achieving the optimal use of DM technology, 20 lack of awareness regarding DM technology was highlighted as a barrier in our survey (Table 4). This brings to the fore a deeper problem in DM management in the country, as proper awareness regarding the basic principles of DM treatment is lacking. A survey by Rahman et al. from Pakistan demonstrated poor levels of awareness regarding DM and its management, among patients with DM with only 23.7% of males and 10% of females knowing the importance of routine blood glucose measurement. 21 Likewise, only 36.3% of males and 13% of females with known DM understand the importance of glycemic control. 21
Other reservations regarding wearable devices centered around not liking having a diabetes device on one’s body (27.5%) and describing it as a hassle (22.5%). Naranjo et al. identified technology adaptability, that is, the ease by which a diabetes device can be integrated into patients’ personal daily lives, as an important consideration in the advancement of diabetes technology. 22
Lastly, concerns regarding dependence on technology were also reported. Around 20% were worried that their wearable devices would not work, and 7.5% of respondents were nervous about relying on technology for DM management, and 15% of respondents reported being too busy to learn how to use new technology. Given the learning curve associated with DM technology, 20 which is particularly relevant in LMICs like Pakistan where many patients may be technologically illiterate, such hesitation regarding the use of technology in DM management is understandable.
Limitations of our pilot survey include its small sample size and subsequent lack of generalizability. Most respondents had either a bachelor’s or higher education which is not representative of the majority in Pakistan. Additionally, the virtual mode of data collection, an unavoidable limitation during the COVID-19 pandemic, may also lead to a lack of generalizability as a significant percentage of the population of Pakistan does not have access to the internet. The lack of adequate representation of patients with DM who are not educated or do not have access to the internet is a limitation of this study, as these patients would undoubtedly have different perceptions and understanding of DM technology.
Conclusion
In our study, although the perceptions regarding diabetes mellitus (DM) technology are generally positive among patients with DM, we have helped identify significant barriers to its widespread acceptance and use in Pakistan. Most prominent is the lack of basic knowledge of DM management among adults with Diabetes. Yet, the implementation of insulin pumps and CGMs should not be considered as premature because Pakistan is an emerging digital market with a marked shift toward overall technology adaptation. Recognizing this, recently 2 leading DM technology companies, have expanded their services and launched their standalone CGMs in the market. There is most definitely a need for larger studies implemented in both urban and rural areas of Pakistan to help expand on the knowledge gained through our study.
Supplemental Material
sj-docx-1-dst-10.1177_19322968211011199 – Supplemental material for Perceptions and Understanding of Diabetes Mellitus Technology in Adults with Type 1 or Type 2 DM: A Pilot Survey from Pakistan
Supplemental material, sj-docx-1-dst-10.1177_19322968211011199 for Perceptions and Understanding of Diabetes Mellitus Technology in Adults with Type 1 or Type 2 DM: A Pilot Survey from Pakistan by Sarah Nadeem, Uswah Siddiqi, Russell Seth Martins and Kaleemullah Badini in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
DMT, diabetes mellitus technology; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; DM, diabetes mellitus; HbA1c, glycated hemoglobin; IHD, ischemic heart disease; LMICs, low- and middle-income countries; SMBG, Self-monitored blood glucose; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study received ethical approval from the ethics review committee of the Aga Khan University Hospital (Reference Number: 2020-5588-14649) and was carried out in accordance with the Declaration of Helsinki (1964) and its future amendments.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.