
Abstract
The purpose of this article is to illustrate that setting standards of care is the cornerstone for excellence in diabetes management. This is underpinned by 3 activities: a standards and accreditation process, an audit and benchmarking program and a linked quality improvement plan. While there are many examples of local auditing and quality improvement programs, there are very few that are at a national level. The National Association of Diabetes Centres (NADC) was formed by the Australian Diabetes Society and the Australian Diabetes Educators Association to set standards of diabetes care in Australia. A rigorous accreditation process was put in place to recognize primary, secondary, and tertiary level diabetes centers that meet these standards. The NADC accreditation process is underpinned by a quality improvement plan, which must be submitted for accreditation to be granted and is informed by the Australian National Diabetes Audit (ANDA). ANDA is conducted annually to gather information about treatments, complications, self-care practices and quality of life outcomes and provides a national as well as an individual report to the participating center that is used to benchmark against other like centers. The ANDA reports are important to inform national policy and advocacy for diabetes care and to also provide information for quality improvement purposes for the individual participating center. We believe that the NADC Standards and Accreditation can be an exemplar for other countries to adapt and adopt to standardize diabetes care at the highest level.
Introduction
According to the Australian Government funded National Diabetes Services Scheme (NDSS) database, there are over 1.38 million people living with diabetes in Australia, giving a prevalence rate of 5.2%. 1 Furthermore, data from the Australian Institute of Health and Welfare (AIHW) indicate that in 2018, diabetes contributed to 11% of all hospitalizations and 10.5% of all deaths. 2 Alarmingly, hospitalization rates and death from diabetes was 2 times higher in the lowest socioeconomic and remote and very remote areas compared with the highest socioeconomic and urban areas, respectively. 2 Finally, Indigenous Australians are 4 times more likely to be hospitalized and die with type 2 diabetes than their non-Indigenous counterparts. 2 In 2013 it was estimated that in Australia diabetes costs $14.6 billion in direct and indirect costs. 3 These data attest to the significant impact of diabetes on the Australian health system and economy.
The intention of this article is to provide evidence that excellence in diabetes care can be achieved by 3 elements: a national standards and accreditation process, an audit and benchmarking program and a linked quality improvement plan. A literature review was conducted via Pubmed using the terms: diabetes, quality improvement, benchmark, and accreditation. The first 1,000 abstracts were reviewed and relevant articles were used to inform this article.
Accreditation and Quality Improvement in Diabetes Care
Accreditation of a service ensures that standards of care are being adhered to and that the best possible care is being delivered to the patient. For example, hospital accreditation via the Danish Healthcare Quality Programme has shown that patients are more likely to have care according to clinical guideline recommendations and lead to improvements in care including diabetes, particularly during the accreditation process.4-6 This also holds true for accreditation of diabetes-related foot services in Germany and Belgium, which resulted in a number of quality improvement outcomes. 7 Finally, national accreditation of primary care practices in The Netherlands showed improvements in 6 diabetes-related indicators. 8
The ability to measure and track clinical performance and outcomes, tied to a quality improvement (QI) process is essential to ensure that the best possible care is provided. This process also identifies areas of strength and opportunity and, therefore, can establish positive feed-forward processes of continual improvement in care delivery if appropriately executed. As illustrated by the United Kingdom Prospective Diabetes Study (UKPDS) for type 2 diabetes 9 and Diabetes Control and Complications Trial (DCCT) for type 1 diabetes, 10 it is critical that care is provided in a timely manner and targets are met to prevent long term complications including cardiovascular and chronic kidney disease. Successful QI initiatives are dependent on an environment that is ready for change and supported by a leadership that is prepared to support change proposals as well as adequate resources to enable change to occur. It is clear that setting standards, assessing performance and having a QI process is critical for managing diabetes and its complications.
There are a number of examples where benchmarking and QI has resulted in positive outcomes and therefore provides support for this approach. For example, at a single large tertiary hospital setting, Bergmann and colleagues completed an audit of their records which showed that 74% of children with type 1 diabetes with mild diabetic ketoacidosis were being hospitalized, and were able to reduce this by 37%. 11 To improve outcomes in new-onset type 1 diabetes, Prahalad and colleagues established the 4T Study for benchmarking and quality improvement, with preliminary data showing a 0.54% reduction in HbA1c 6 months post-diagnosis, compared with historical control data. 12
Similarly, Quach and colleagues implemented a quality project and improved completion of foot exams and amputation risk assessments for veterans with diabetes, by using a four-member patient aligned care team. 13 At a larger scale, a consortium comprising 6 affiliated hospitals and 4 university health sciences schools established a QI patient safety program with outcomes of delivering educational programs and improving patient healthcare quality and safety. 14
Likewise, Acharya and colleagues developed a QI program across a large health district in regional New South Wales Australia, challenged with significant rural and remote geography and limited specialist workforce. 15 Over 12 months, the QI program resulted in a 0.4% reduction in HbA1c, a 1 kg weight loss and a 3 mmHg reduction in systolic blood pressure. 15 In support, a study by Cheng and colleagues implemented a QI plan in 5 primary care practices in Ontario Canada and showed improvements in HbA1c, LDL-C and diastolic blood pressure with greater improvements in patients above the recommended therapeutic targets. 16
It is clear from the above discussion that accreditation, benchmarking and QI processes can lead to better outcomes in diabetes. It is also evident that these activities often occur at a single site or local health service area, with the potential of being scaled up to a state or national level. However, there are few combined national benchmarking and QI programs that have been reported in the literature. The American Diabetes Association has developed the Diabetes INSIDE (Inspiring System Improvement with Data-Driven Excellence) Program based on their Standards of Medical Care in Diabetes. 17 Implementation of Diabetes INSIDE for adults with type 2 diabetes in a local health system resulted in reduced HbA1c levels and the number of patients with a HbA1c above 9%. 18 Furthermore, simulation modelling in patients with a baseline HbA1c 8% or greater showed reduced 5-year complication rates including all-cause mortality, cardiovascular disease death, non-fatal/fatal myocardial infarction, non-fatal/fatal stroke, end-stage renal disease, blindness, and neuropathy. 19
Another important national QI is in Hong Kong, which in 1995 established a territory wide diabetes registry (Hong Kong Diabetes Registry), and was the catalyst for a number of initiatives and quality improvement programs which include the Joint Asia Diabetes Evaluation (JADE) program and the Risk Assessment and Management Program for Diabetes Mellitus (RAMP-DM). 20 These were underpinned by upskilling nurses to perform specific tasks such as foot checks and preparing patients for fundoscopies, in addition to the introduction of an electronic medical record. Furthermore, establishment of a register that gathered data, monitored performance and trends, including care gaps, was introduced at 18 hospital-based diabetes centers. Additionally, this tool facilitated benchmarking and has resulted in identification of care gaps for continued improvements in care. 20
The National Association of Diabetes Centres (NADC)
In 1994, the National Association of Diabetes Centres (NADC) was established by the Australian Diabetes Society and the Australian Diabetes Educators Association, the peak health professional bodies representing endocrinologists/diabetologists and diabetes educators in Australia. 21 The NADC was initially funded by a grant from the Commonwealth Government of Australia and comprised mainly of tertiary level hospital-based diabetes centers with a key aim of collaboration and benchmarking care between diabetes services across the country. Over the years and in recognition that care occurs across the spectrum of health services, the NADC has encouraged and indeed increased its membership in secondary/community and notably in primary care, where the majority of people with type 2 diabetes are being cared for. At its core, the NADC is responsible for setting national standards for diabetes care. This is achieved through a rigorous accreditation process supported by a National Diabetes Care Course and the Australian National Diabetes Audit for benchmarking and QI purposes. 22 The NADC Standards and Accreditation Program is novel as it is a national enterprise and other than the Hong Kong based diabetes registry and QI program, we are not aware of another similar endeavor specifically for diabetes centers in tertiary, secondary, and primary care.
The NADC Standards and Accreditation Program
The NADC Standards of Care underpin the accreditation program and have been developed to assist all diabetes services from primary care through to tertiary level centers to achieve quality care through improved governance, education and clinical criteria (Figure 1). To achieve accreditation, it is expected that all tertiary level centers are able to meet most of the applicable criterion indicators. The 4 areas of accreditation are: Healthcare Improvement; Governance and Process; Management Quality and Safety; and Centre Maintenance. A sample of the NADC Accreditation Scoresheet used by assessors is provided in Figure 2. Secondary and primary care services are assessed against like-sized organizations and are also reviewed against the type and level of services that the particular organization provides. This background information is provided in the application form and in the additional information documents attached to the accreditation application. It is important to recognize that many NADC services are already accredited in their affiliation with a larger hospital, community health service or general practice. There are deliberate synergies and overlap with existing accreditation systems such as the Royal Australian College of General Practitioners (RACGP) Standards for General Practice and the National Safety and Quality Health Service (NSQHS) Standards. A Standards and Accreditations Committee comprising of experienced endocrinologists, credentialed diabetes educators and primary care practitioners oversees the NADC Standards and Accreditation Program to minimize duplication and to ensure that the appropriate standards are being assessed.
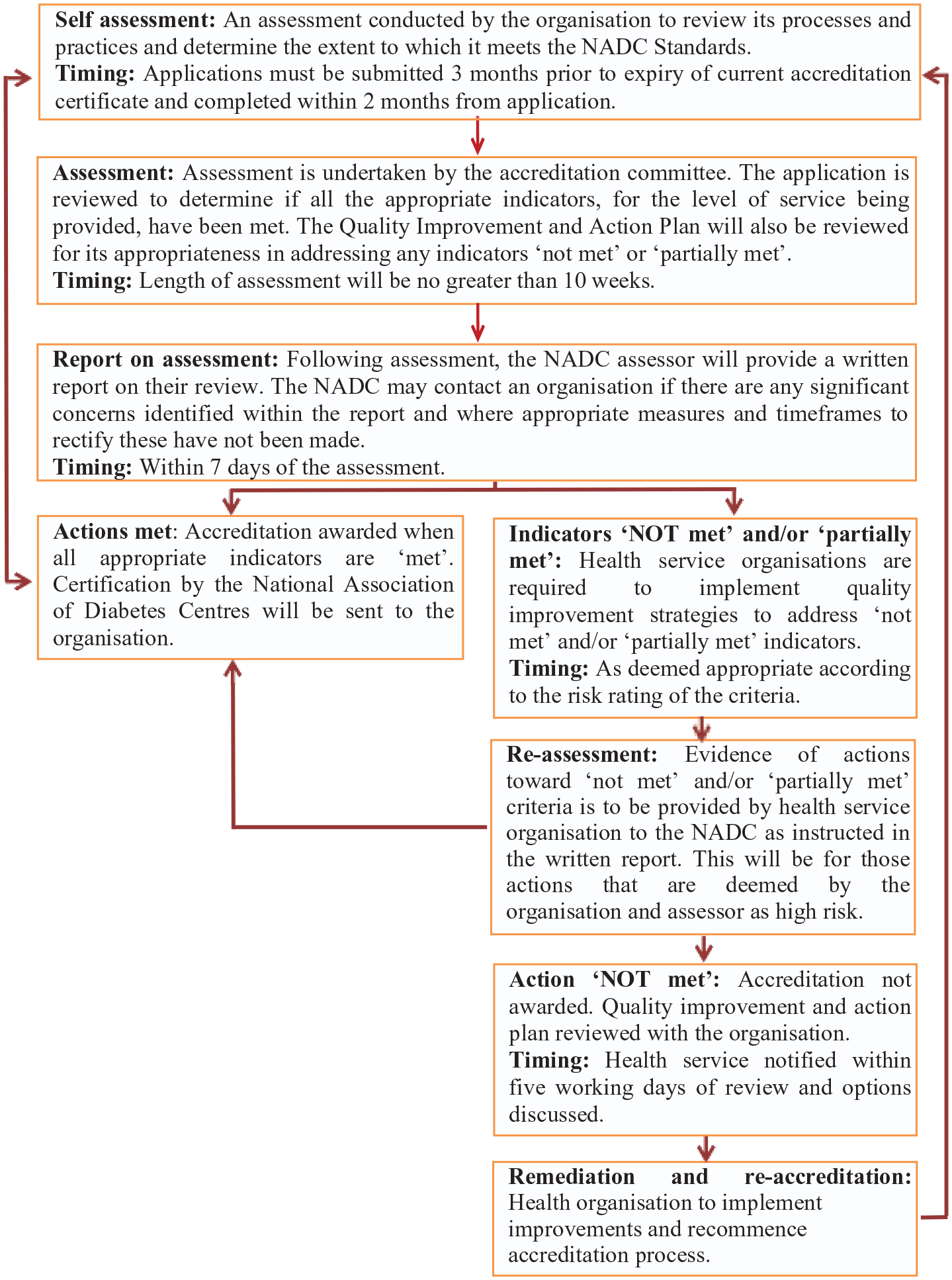
The NADC accreditation process.
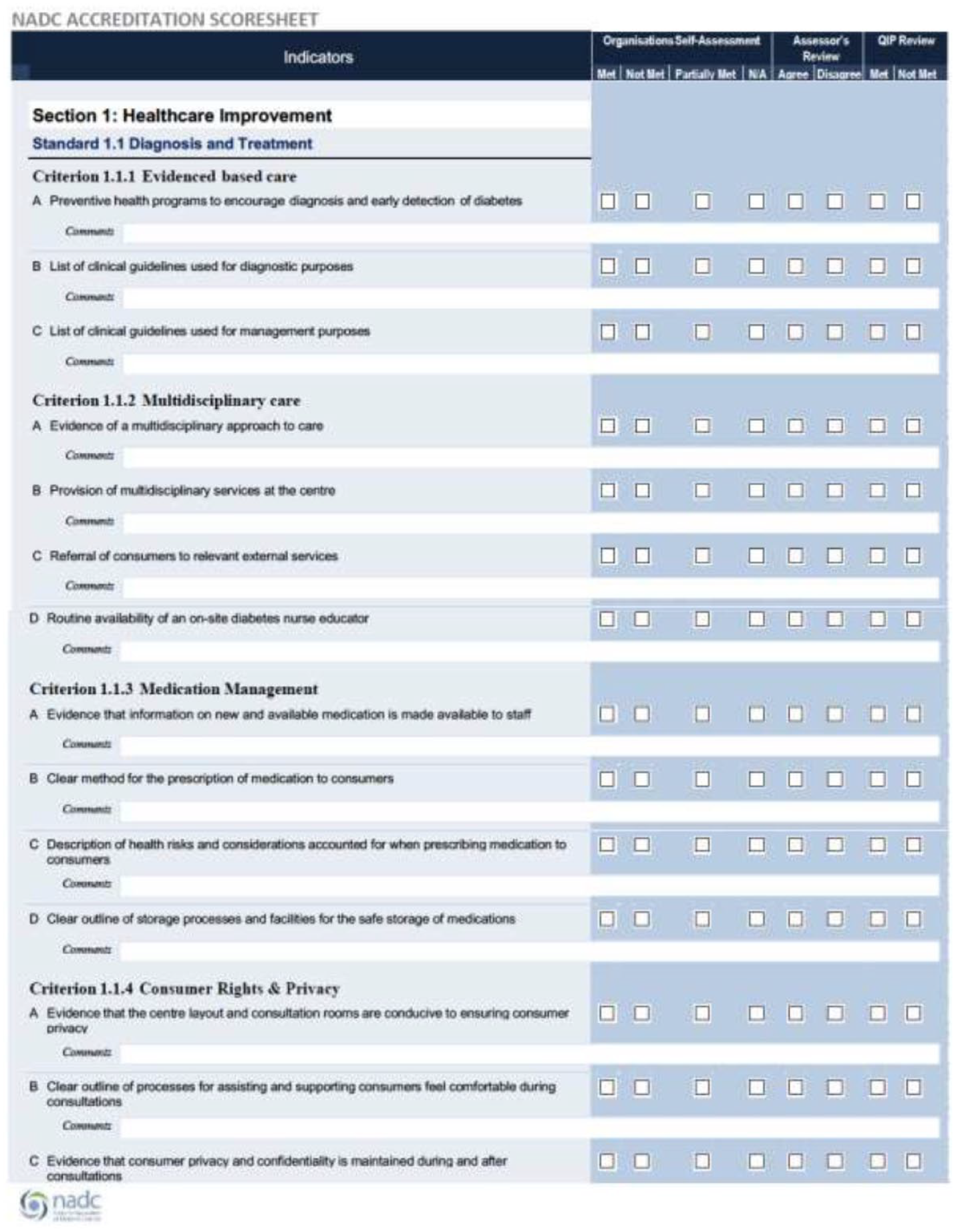
Sample of the NADC accreditation scoresheet used by assessors.
Central to the accreditation program is a QI process, as it is integral for ensuring improved patient health outcomes through reflective practice, evidence-based care, and best practice clinical care (Figure 1). There are many components to the NADC’s QI program, including physical structure and processes of an organization, through to governance, leadership, education and training and of course, clinical care. Participation in the Australian National Diabetes Audit (ANDA) is encouraged as part of the service’s QI evidence. Indeed, the NADC Standards require monitoring and improvement strategies to be demonstrated as routine practice within the organization. Throughout the accreditation self-audit process, a quality improvement plan is to be developed alongside the Standards and Accreditation application. The plan provides assessors with an indication of existing QI activities in addition to any further requirements identified throughout the self-assessment process. The quality improvement plan includes details of the desired outcome, what will be undertaken to achieve this, and the timelines for each action. Each service must complete the QI Plan and execute actions documented in the plan within the timeframes outlined on the QI Plan template. The NADC assessor reviews the action items and stated priority levels to ensure these are appropriate for the type and size of the organization and expected level of service delivery. If the plan is felt to be lacking or activities not appropriately defined, the organization is contacted by the NADC to discuss these further. Where appropriate, a virtual meeting with the team and the accreditation manager is held to discuss concerns and the requirements for more evidence or need for further organizational progress to meet the expectations of the Standards. Further, where “High Priority” action items have been identified by either the organization or the surveyor, the NADC will follow up with services to ensure these have been undertaken. If organization action items, in consultation with the assessor, are felt to have not been met within an appropriate timeframe, accreditation may be withdrawn.
Approximately 10% of applicants fail NADC Standard Accreditation in any given round. The main reasons for this are insufficient evidence provided and/or unable to meet the core criteria and a lack of quality improvement process. It is clear that successful organizations are those that complete the application using a team approach, compared to those that have 1 team member responsible for the accreditation process.
It is clear from the above description that the NADC Standards and Accreditation Program is quite involved and rigorous. Therefore, it is recommended that a team approach is employed in completing the application. This assists in lessening the burden on any one individual within a service but ensures widespread understanding of the NADC standards among all staff. Benefits to the service for being a NADC accredited center is significant kudos among their peers and within their broader facility. Importantly, it provides opportunities to leverage for additional funding support from within the organization and beyond. As of the 1st June 2020, there were 28 diabetes services holding NADC accreditation in Australia, with 2 services in the assessment process. A copy of the NADC Accreditation Workbook can be found at https://nadc.net.au/accreditation/.
Australian National Diabetes Audit (ANDA)
The Australian National Diabetes Audit (ANDA) is another important QI activity for services across all states and territories of Australia. 22 The audit is cross-sectional and occurs between May and June each year, with centers completing a minimum dataset form of the first 100 patients that present to the tertiary service (60 patients are required for secondary and 30 patients for primary care services). A copy of the minimum dataset can be found in the annual reports at https://nadc.net.au/anda/. Information that is collected includes treatments, complications, self-care practices and quality of life outcomes. Participating diabetes services receive an individualized report of their patient outcome data in comparison with their peers. In addition to the primary report received by participating sites, the pooled national report is an important source of cross-sectional data on the clinical status and outcomes of people with diabetes attending services across the country. Sharing this information in an annual report assists in identifying processes that may be adopted to improve education and clinical care which (once implemented) should result in improved outcomes for people attending those centers. A report providing comparison data for each site compared against all other sites is generated. Pooled data analysis addressing the outcome findings for all data fields enable sites to compare and benchmark their practice findings against other participating sites. ANDA data provide additional and vital QI processes for diabetes services in Australia. Identifying site-specific and nationwide variations in clinical performance can inform the implementation of targeted, evidence-based QI activities. This, in turn promotes best practice and high-quality care to reduce the occurrence of diabetes-related complications and ultimately improve the quality of life among people living with diabetes in Australia. The addition of longitudinal linkage to the ANDA (ANDA-L) facilitates future analysis of trends in diabetes health outcomes and correlation to different treatment approaches.
As a result of this nationwide audit and benchmarking process we have been able to show that younger people with type 2 diabetes (<60 years) had worse glycemic control and were more likely to be obese, dyslipidemic and smokers than older patients (>60 years). 23 This was associated with younger people with type 2 diabetes not adhering to medication and dietary recommendations and self-care practices and blood glucose monitoring. 24 Furthermore, the apparent difficulty of this group in following dietary advice, smoking, forgetting medications, and increased incidence of diabetes distress were all associated with greater odds of depression, whereas higher own health rating was associated with lower odds (all p < 0.02). 25 In addition, female gender, increasing HbA1c, insulin use, difficulty following dietary recommendations and depression were all associated with greater odds of diabetes distress and older age, higher own health rating and monitoring blood glucose levels as recommended were associated with lower odds. 25 Depression, diabetes distress and higher HbA1c were all found to be associated with was associated with sub-optimal self-care, while diabetes distress was associated with higher HbA1c and sub-optimal self-care. 25 Of note, people with type 2 diabetes who were current or past smokers had a higher HbA1c than never smokers and higher triglyceride and lower HDL levels. 26 Moreover, compared to never smokers, current smokers had higher odds of severe hypoglycemia. Current and past smokers also had higher odds of myocardial infarction, stroke, peripheral vascular disease, lower limb amputation, erectile dysfunction and peripheral neuropathy, with no significant change over time. 26
In a type 1 diabetes cohort cardiovascular risk factors that were prevalent included hypertension, dyslipidemia, overweight/obesity, ever smoking, albuminuria, estimated glomerular filtration rate < 60 mL/min/1.73 m2 and HbA1c > 7.0% [27]. Furthermore, older age, longer diabetes duration, smoking, and antihypertensive therapy use were positively associated with cardiovascular disease, while high density lipoprotein cholesterol and diastolic blood pressure were negatively associated. Worryingly, these risk factors increased linearly with 20 years or more disease duration. Diabetes specific cardiovascular risk stratification tools incorporating diabetes duration will be an important consideration in future guideline development. 27 Interestingly, the use of technology in adults with type 1 diabetes (CGM, insulin pumps, or combined insulin pump and CGM) was associated with lower HbA1c compared to standard care. 28 This supports the clinical benefits of the Australian Government subsidy program to CGM for eligible adults with type 1 diabetes 1 and argues for equitable and affordable access to technology. Technology use was not associated with diabetic ketoacidosis, but CGM was associated with more hypoglycemia. 28
It is clear from the above outcomes that ANDA is an important activity for benchmarking and QI activities to ensure that best care is being delivered to people with diabetes. It is also a valuable source of information that can contribute to advocacy within an organization and more broadly to state and national governments for increased funding and support of services, access to therapies and resourcing.
Concluding Remarks
The NADC Standards and Accreditation Program for diabetes centers is a national activity that aims to ensure the highest level of care delivery is being achieved. It is relevant across the spectrum of care from primary through to tertiary levels centers and is underpinned by a QI activity to ensure continued progress toward care excellence. It is important to note that the NADC also offers standards and accreditation for tertiary diabetes centers that provide diabetes technology and high-risk foot services, for pharmacies with an interest in diabetes therapeutics and products and an accreditation program for Centre of Excellence for tertiary centers that can demonstrate that they not only meet but indeed exceed the standard criteria. The ANDA initiative is key to measuring care outcomes and provides benchmarking against similar services and informs the QI process.
The NADC Standards and Accreditation can be an exemplar for other countries to adapt and adopt to standardize diabetes care at the highest level. Accreditation and standards of care, auditing and QI are fundamental components of an integrated interdisciplinary approach to diabetes care with the ultimate goal of reducing and preventing complications.
Footnotes
Acknowledgements
None.
Abbreviations
AIHW, Australian Institute of Health and Welfare; ANDA, Australian National Diabetes Audit; DCCT, Diabetes Control and Complications Trial; NADC, National Association of Diabetes Centres; NDSS, National Diabetes Services Scheme; QI, Quality Improvement; UKPDS - United Kingdom Prospective Diabetes Study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Australian Diabetes Society and the National Association of Diabetes Centres has received support from the Australian Government Department of Health as well as the following companies: Abbott Diabetes Care, AstraZeneca, Boehringer Australia, Eli Lilly Australia, MSD Diabetes, Novo Nordisk Australia, Roche Australia, Sanofi Diabetes.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.