
Abstract
Background:
Diabetes technology use is associated with favorable type 1 diabetes (T1D) outcomes. American youth with public insurance, a proxy for low socioeconomic status, use less diabetes technology than those with private insurance. We aimed to evaluate the role of insurance-mediated provider implicit bias, defined as the systematic discrimination of youth with public insurance, on diabetes technology recommendations for youth with T1D in the United States.
Methods:
Multi-disciplinary pediatric diabetes providers completed a bias assessment comprised of a clinical vignette and ranking exercises (n = 39). Provider bias was defined as providers: (1) recommending more technology for those on private insurance versus public insurance or (2) ranking insurance in the top 2 of 7 reasons to offer technology. Bias and provider characteristics were analyzed with descriptive statistics, group comparisons, and multivariate logistic regression.
Results:
The majority of providers [44.1 ± 10.0 years old, 83% female, 79% non-Hispanic white, 49% physician, 12.2 ± 10.0 practice-years] demonstrated bias (n = 33/39, 84.6%). Compared to the group without bias, the group with bias had practiced longer (13.4±10.4 years vs 5.7 ± 3.6 years, P = .003) but otherwise had similar characteristics including age (44.4 ± 10.2 vs 42.6 ± 10.1, p = 0.701). In the logistic regression, practice-years remained significant (OR = 1.47, 95% CI [1.02,2.13]; P = .007) when age, sex, race/ethnicity, provider role, percent public insurance served, and workplace location were included.
Conclusions:
Provider bias to recommend technology based on insurance was common in our cohort and increased with years in practice. There are likely many reasons for this finding, including healthcare system drivers, yet as gatekeepers to diabetes technology, providers may be contributing to inequities in pediatric T1D in the United States.
Keywords
Introduction
The use of diabetes technology, such as insulin pumps and continuous glucose monitoring (CGM), improves glycemic outcomes in youth with type 1 diabetes (T1D), thereby decreasing risk for both short- and long-term complications.1-7 There has been a marked uptake in diabetes technology use in the last decade,8-11 however, the use of diabetes technology has preferentially increased in youth from higher socioeconomic groups.9,10 Studies have consistently demonstrated lower rates of diabetes technology use in youth of lower socioeconomic status (SES) when compared to youth from higher SES groups and this gap has widened in the last decade in the United States. 9
This observed inequity in uptake and access to innovative diabetes technology is consistent with a larger pattern in the introduction of any new and effective treatment where uptake first occurs in individuals from higher SES. 12 Generally, disparities emerge when an efficacious treatment option has unequal access.12,13 One contributor to these disparities is the often unconscious and systematic discrimination of one sub-group, referred to as implicit bias. 14 Implicit bias can also present as the systematic promotion of a non-marginalized subgroup. In an example of the effect of provider implicit bias on medical decisions and outcomes, pediatricians are less likely to prescribe narcotics post-surgery to black children when compared to white children. 15 When compared to non-Hispanic Whites, racial/ethnic minorities were consistently less likely to receive clinically indicated preventive services, diagnostic tests, and procedures spanning the breadth of disease areas including diabetes.14-18 The role of implicit bias in diabetes technology recommendation by providers for low SES youth has been understudied.
The aim of this study, entitled The Gatekeeper Study, is to determine if provider implicit bias against public insurance, as a proxy for low SES, influences diabetes technology recommendations in the United States. Consistent with the literature at large, we hypothesized that insurance-mediated provider implicit bias, defined as the systematic discrimination of youth with public insurance, would be common in providers in recommending diabetes technology.14,18-20
Methods
Study Overview
The Gatekeeper Study is a prospective study consisting of a baseline diabetes provider implicit bias assessment followed by an educational module on the role of implicit bias. This report focuses on the documentation of provider bias at baseline, prior to receipt of the educational module. Written informed consent was obtained before data collection. The Gatekeeper Study was delivered online and managed using REDCap, hosted at Stanford University21,22 and was approved by the Stanford University Institutional Review Board.
Participants
We recruited multi-disciplinary U.S. pediatric T1D providers between September 2019 and March 2020. For the purposes of this study, providers are defined as physicians, nurse practitioners, and certified diabetes educators as these are the medical personnel who are thought to determine which patients will be introduced to and prescribed insulin pumps and CGM in most pediatric clinics. To facilitate recruitment, we contacted pediatric endocrine division chiefs or research collaborators of the authors in 8 states (California, Colorado, Connecticut, District of Columbia, Massachusetts, North Carolina, Ohio, and Texas) to solicit assistance in recruiting providers from their division who care for youth with T1D.
Provider Variables
After consenting to the study, basic provider demographic characteristics such as provider role, practice-years, age, sex, self-identified race/ethnicity, workplace location, percent public insurance served in their clinic, and personal diagnosis of T1D were collected.
Diabetes Provider Implicit Bias Tool
The Diabetes Provider Implicit Bias (D-PIB) Tool consisted of 2 components: a hypothetical case vignette (see supplemental material) designed by our team and a ranking exercise of patient factors that providers considered to be important in the recommendation of diabetes technology (evaluated separately for insulin pump and CGM).
For the hypothetical case vignette component, providers were randomized and assigned one of two identical case vignettes with insurance status, a proxy to SES, as the only differing factor. We asked providers to determine if they would offer technology to a 13-year-old female with T1D who is adequately engaged but not meeting standardized treatment targets for hemoglobin A1c (HbA1c). 23 A case vignette approach was chosen as it has been used effectively in medical education, practice guidelines, and decision support systems and is a familiar format to the medical provider. 24 In developing the vignette, an incomplete factorial survey design was used. This design method involves creating vignettes based on a set of predefined factors that describe the likely subset of combinations seen in clinical situations and decision-making trees. Incomplete factorial designs are established as a means of unbiased surveying that obviate the need to explore all possible combination of predefined factors. 24
In the ranking exercise, providers ranked patients’ modifiable and non- modifiable factors in the order of consideration for initiating technology therapy (1 = most important to 7 = least important). The patient factors that were evaluated were race/ethnicity, the family’s income, age, HbA1c, type of insurance coverage, self-monitoring blood glucose (SMBG) checks per day, and family preference. Providers were required to rank all 7 patient factors in order of importance. In addition to ranking these factors in order of most to least important in the provider’s consideration to start insulin pump or CGM, providers also listed which factor was the most and the least important in their decision to recommend insulin pump or CGM.
After the development of the D-PIB, we used cognitive testing and retrospective probing to ensure the reliability of the D-PIB.25,26 Consistent with cognitive testing, we solicited input from diabetes psychologists, pediatric endocrinologists, and providers living with type 1 diabetes after development of the items to assess whether the questions satisfied the intended purposes. After the further refinement of survey items based on this feedback, we tested the scale on 3 providers, who completed the measure and then explained their interpretation of each question. This methodology was consistent with the principles of retrospective probing. The items did not require revision based on responses from the 3 test providers.
Definition of Provider Implicit Bias
During the time of this study, state insurance payers relevant to our study covered insulin pump and CGM therapy for youth with T1D.27-29 Therefore, if insurance was utilized as an important factor in the decision to recommend diabetes technology, the provider was flagged as having bias. Specifically, for the clinical vignettes, the a priori definition of provider implicit bias was met when patients in the vignettes with private insurance were offered more technology than patients in the vignettes with public insurance. For the ranking exercise, the a priori definition of provider bias was met when insurance was considered important (ranked in the top 2 factors) to recommend technology. Based on clinical experience, we anticipated that if insurance was considered an important factor in recommending diabetes technology, it would be considered at or near the top of the list for a provider’s consideration. If a provider demonstrated bias in one or both parts of the assessment, they were categorized as demonstrating bias.
Data Analysis: The primary outcome is frequency of provider bias and provider characteristics that were associated with provider bias. A priori power calculations demonstrated 47 providers were needed to achieve a power of 0.8; 40 providers achieve a power of 0.7. We evaluated which patient factors were most important for recommending diabetes technology via the ranking exercise. Provider characteristics and bias were analyzed with descriptive statistics and group comparisons (t tests for continuous variables and chi-square/fisher’s exact for categorical variables). Informed by the findings of the univariate analysis, we built a multivariate logistic regression with provider bias as the dependent variable and provider characteristics (age, sex, race/ethnicity, provider role, percent public insurance served, and workplace location) as independent variables to determine contributors to provider bias. All statistical analyses were executed using RStudio 1.3.
Results
Provider Characteristics
We consented 42 providers to participate and 39 providers completed the baseline D-PIB tool. Provider characteristics are presented in Table 1. Randomization was effective in our cohort with no statistical differences in age, sex, race/ethnicity, provider role, personal diagnosis of T1D, workplace characteristics, practice-years, or percent public insurance served in those randomized to public vs private insurance clinical vignettes.
Provider Characteristics.

n (%) presented unless otherwise specified.
Bias is determined by baseline responses to Diabetes Provider Implicit Bias tool.
P values were calculated using independent t tests for continuous variables and chi-square test for binary or categorical variables. Values below .05 are bolded.
The mean age of our participants was 44.1 ± 10.0 years and the majority of providers were non-Hispanic White (n = 31, 79.5%) and female (n = 35, 89.7%). All three target provider roles were represented in our participants (physicians n = 19, 48.7%; nurse practitioners n = 12, 30.8%; certified diabetes educators n = 8, 20.5%). Nearly 30% of participants had a personal history of T1D. The majority of the providers work in urban (n = 28, 71.8%) and academic (n = 35, 89.7%) settings with mean practice-years of 12.2 ± 10.0 years.
Factors to Recommend Diabetes Technology
Provider ranking of patient factors is presented as a violin plot in Figure 1. Type of insurance coverage was second most important for recommending CGM (mean rank 2.83 ± 1.56) and was fourth most important in recommending insulin pump therapy (mean rank 3.74 ± 1.69). Providers ranked family preference as the most important consideration in recommending insulin pump or CGM therapy (mean rank 1.57 ± 0.88 and 1.69 ± 1.05, respectively). Race/ethnicity was ranked to be the least important consideration in recommending insulin pump or CGM therapy (mean rank 6.86 ± 0.43 and 6.91 ± 0.37, respectively).
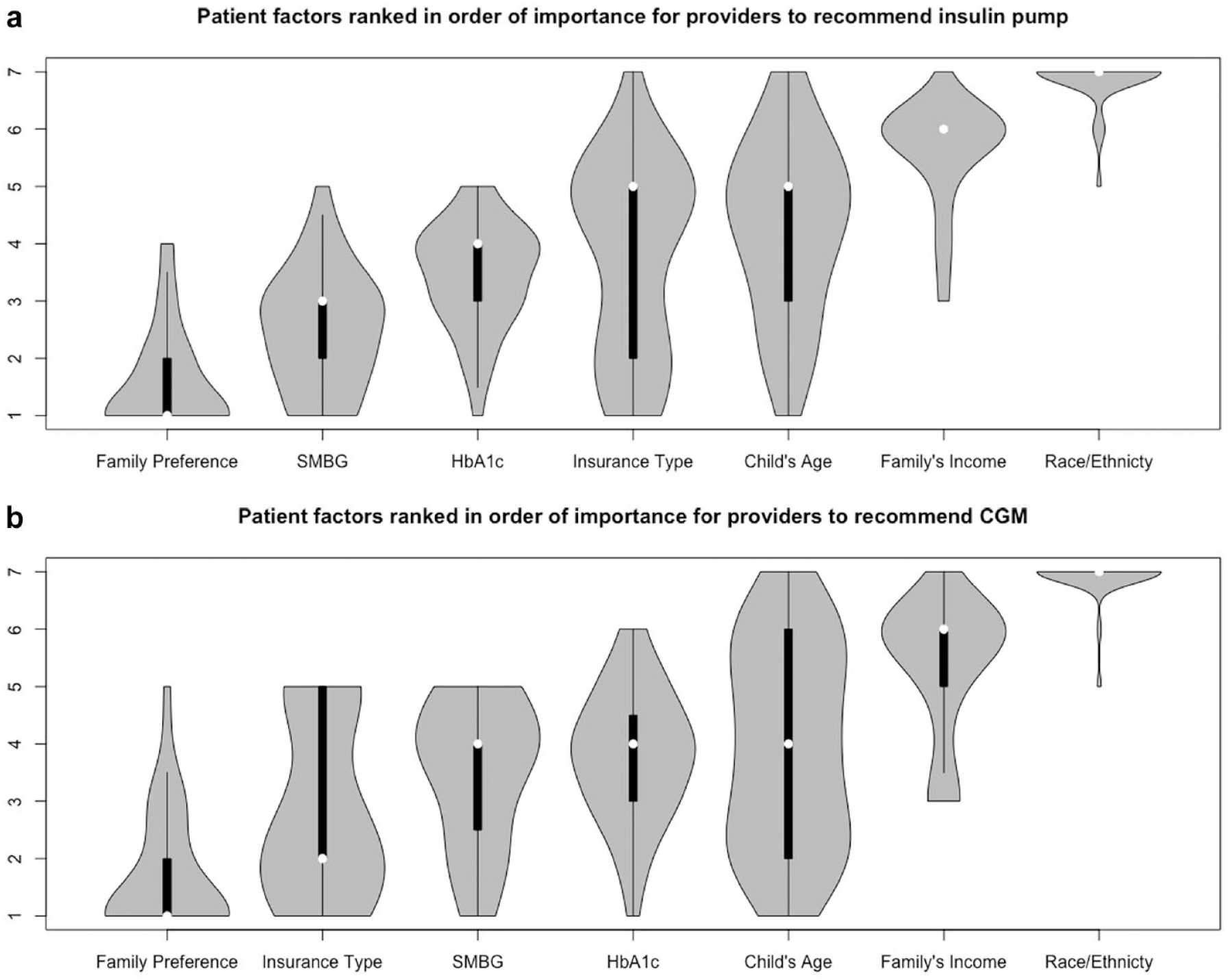
Patient factors ranked in order of importance for providers to recommend insulin pump or CGM.
Presence of Bias
Implicit bias against public insurance was common in our cohort (n = 33, 84.6%). Group comparisons of provider characteristics stratified by bias are presented in Table 1. When compared to those who had bias, providers who did not have bias tended to have fewer practice-years (13.4 ± 10.4 years vs 5.7 ± 3.6 years, p = 0.003). Although age and practice-years are highly correlated (r = 0.88, P < .001), there was no difference in age of providers with bias and without bias (44.4 ± 10.2 vs 42.6 ± 10.1, respectively; P = .701). The provider’s sex, race/ethnicity, personal diagnosis of T1D, roles, workplace characteristics, or percent public insurance served did not differ in the groups with bias and without.
The findings from the multivariate logistic regression model are presented in Table 2. Practice-years remained significantly associated with bias (adjusted odds ratio: 1.47, 95% CI [1.02,2.13]; P = .007) in the multivariate model. Thus, for each increase in year in practice, the odds of having bias increases by a factor of 1.47. As in the univariate analysis, age was not associated with bias (adjusted odds ratio 1.23, 95% CI [0.96,1.59]; P = .057). Similarly, the remainder of the provider characteristics, such as race/ethnicity (adjusted odds ratio: 7.52, 95% CI [0.36,155.67], P = .163), were not associated with bias in the multivariate model.
Adjusted Odds Ratios (OR) of Provider Characteristics and Implicit Bias with the Model Adjusting for Age, Sex, Race/Ethnicity, Provider Role, Percent Public Insurance Served, and Workplace Location.
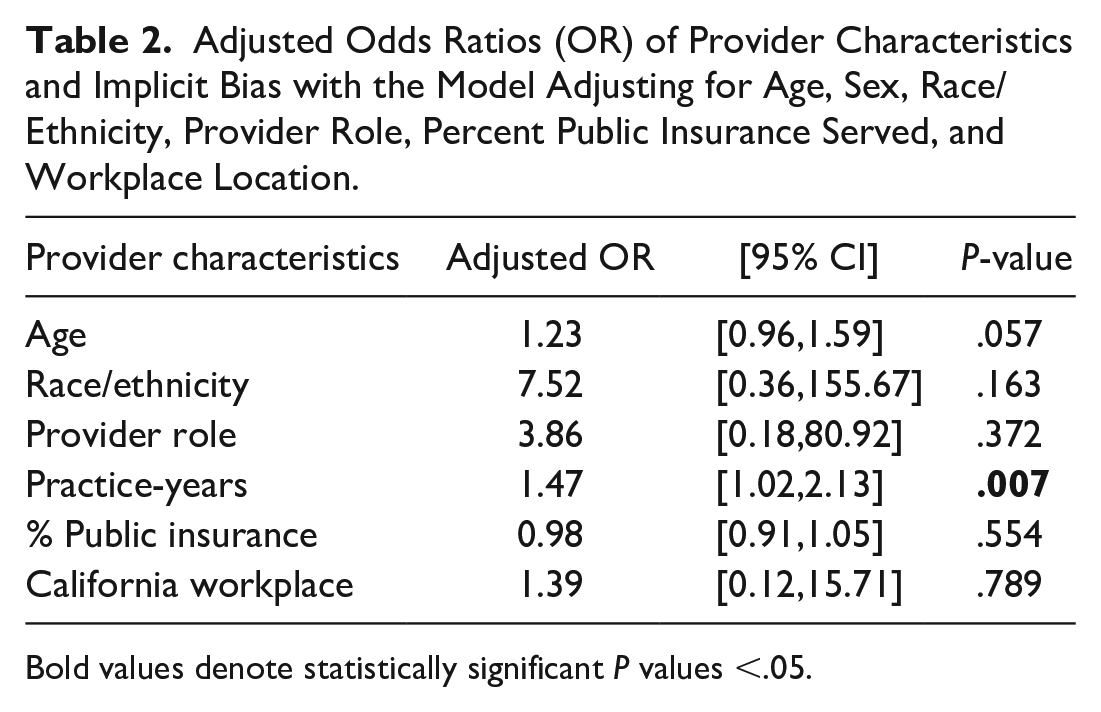
Bold values denote statistically significant P values <.05.
Discussion
To our knowledge, this is the first study evaluating provider implicit bias on diabetes technology recommendation in the United States. We demonstrate that provider implicit bias is common with nearly 85% of our U.S. cohort meeting implicit bias criteria. This finding is consistent with our hypothesis and the report of provider implicit bias in the literature: provider implicit bias is common and has an impact on provider’s management recommendations.14,18-20 The effect of provider implicit bias on recommendations is hypothesized to be a driving factor in health inequities.13,14 In addition, we report a strong association between bias and practice-years suggesting that the longer an individual is in practice, the more likely they were to have insurance-mediated implicit bias. Importantly, this relationship was not present with age and is unique to years in practice. These data raise the concern that as providers practice longer, their attitudes may themselves be a barrier to diabetes technology adoption and contribute to the disparities seen in pediatric T1D technology use by SES.9,10,30,31 The differential use of diabetes technology adoption is considered to be a factor in the inequities seen in HbA1c by SES.9,32,33 These data call to attention the need for providers to reevaluate their current biases in recommending diabetes technology to youth with T1D. Insurance is inevitably a factor in diabetes technology utilization in the United States, however it should not be one of the most important factors in a provider’s decision to recommend and initiate diabetes technology.
These results should be considered in the context of where the providers practiced. During the time of this study, state insurance payers in the geographical locations of our study cohort had policies that covered insulin pump and CGM therapy for youth with T1D.27-29 However, the date when insulin pump and CGM coverage was approved varied by state as did the requirements to initiate and maintain coverage. For example, in California where half of our cohort practiced, CGM coverage was approved in 2016 (before the start of our study) but required documentation of ≥3 blood glucose checks per day, insulin use, a commitment to wear a CGM, and documentation of a need to use CGM for initial approval. For continued approval, individuals had to continue to demonstrate ≥3 checks per day and file re-approval paperwork every 6 months. 28 More recently, the requirement to demonstrate ≥3 checks per day for reapproval was lifted. Although policy changes have taken place, the cumbersome nature of the paperwork required to initiate and maintain coverage persists and is associated with both increased interruptions to diabetes technology and to poorer HbA1c outcomes.29,32,34 This pattern of onerous and challenging coverage policies are observed in other state insurance payers as well 34 and may be a key driver of the formation of provider implicit bias against public insurance.
Provider years in practice represents a key driver of bias in this study. Generally, providers with longer years of work experience would be more likely to have encountered prohibitive coverage policies for youth with public insurance that precluded the ability of providers to offer diabetes technology. It may be challenging for providers to stay up to date on state insurance payers’ policy changes over time. This can result in the bias that youth with public insurance will not have adequate coverage for diabetes technology and therefore should not be recommended to initiate diabetes technology. The overestimation of insurance as a barrier to diabetes technology, as reported elsewhere, 31 is a manifestation of implicit bias against youth with public insurance and may be a contributor to T1D inequities. Similar to payer policy changes, clinical practice guidelines are also being updated regularly and require the diabetes provider to stay up to date on guidelines as well. For example, in 2019 the American Diabetes Association added specific guidance that “continuous glucose monitors should have continued access across third-party payers.” An implication of this study is that the diabetes provider would benefit from regular updates on coverage policies in their state and county and from being mindful of their persisting biases, particularly as they gain more experience in the field of pediatric diabetes. Of equal importance is for state insurance payers to expand coverage and simplify the process of applying and maintaining coverage given that youth with T1D and public insurance want, utilize, and benefit from diabetes technology.29,32,34 It is important to reflect on provider- and insurance-mediated drivers of health inequity in order to realize effective solutions to mitigate disparities.
The limitations to this study include the small study sample comprised of individuals who predominately identified as female and non-Hispanic white. However, in the United States, pediatric diabetes providers more commonly identify as non-Hispanic white female, and thus this study captures the relevant population to assess provider bias. Although the D-PIB was not validated via quantitative methods such as principal component analysis, we were able to establish fidelity of the measure with cognitive testing and retrospective probing. In addition, we were able to demonstrate rates of bias consistent with prior publications evaluating provider bias in the medical field at large. As with many studies, there is a selection bias of participating providers that should be accounted for and in interpreting these data. However, we still see a significant presence of bias against prescribing diabetes technology for pediatric patients with T1D and public insurance in our findings. Strengths of the study include the prospective randomized nature of the study as well as the content we studied.
Conclusions
To our knowledge, this is the first study to evaluate provider implicit bias against public insurance with regards to diabetes technology recommendations in the United States. Provider implicit bias to recommend technology based on insurance was common in our U.S. cohort and increased with years in practice. These data suggest that provider implicit bias contributes to decreased technology access for youth with public insurance, and we hypothesize this has formed due, in part, to changing coverage policies and higher standards for youth with public insurance to gain approval for devices. Providers, shown in this study as gatekeepers to diabetes technology, can also be a promoters to close disparity gaps with further training and more frequent updates on bias and coverage policies. This ultimately would improve the very real inequities observed in pediatric T1D.
Supplemental Material
sj-docx-1-dst-10.1177_19322968211006476 – Supplemental material for Provider Implicit Bias Impacts Pediatric Type 1 Diabetes Technology Recommendations in the United States: Findings from The Gatekeeper Study
Supplemental material, sj-docx-1-dst-10.1177_19322968211006476 for Provider Implicit Bias Impacts Pediatric Type 1 Diabetes Technology Recommendations in the United States: Findings from The Gatekeeper Study by Ananta Addala, Sarah Hanes, Diana Naranjo, David M. Maahs and Korey K. Hood in Journal of Diabetes Science and Technology
Footnotes
Author Contribution
AA and KKH conceived, designed, and conducted the study with contributions from DMM and DN. AA conducted the analysis with support from SJH and supervision from KKH. AA wrote the manuscript. AA, SJH, DN, DMM, and KKH reviewed and revised the manuscript with critical contributions. AA and KKH are the guarantor of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Abbreviations
CGM, Continuous glucose monitoring; D-PIB, Diabetes Provider Implicit Bias; HbA1c, Hemaglobin A1c; SES, Socioeconomic status; SMBG, Self-monitoring blood glucose; T1D, Type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Maahs has had research support from the NIH, JDRF, NSF, and the Helmsley Charitable Trust and his institution has had research support from Medtronic Diabetes, Dexcom, Insulet, Bigfoot Biomedical, Tandem, and Roche. Dr. Maahs has also consulted for Abbott, the Helmsley Charitable Trust, Sanofi, Novo Nordisk, Eli Lilly, Medtronic, and Insulet. Dr. Hood has received consulting fees from Lifescan Diabetes Institute and MedIQ and an investigator-initiated grant from Dexcom, Inc. Otherwise, no potential conflicts of interest relevant to this article were reported by the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Addala is supported by the Maternal Child Health Research Institute and by Stanford University’s K12 (K12DK122550).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.