
Abstract
Background:
While we expect that patients who adjust their insulin delivery algorithms between clinic visits to have better glucose control compared to those who do not, this effect has not been quantified.
Method:
This is a single-center retrospective cohort study including pediatric and adult patients with type 1 diabetes evaluating insulin pump self-management behaviors. Basal insulin dose information was obtained from the Glooko-Diasend database, and used to quantify the frequency and magnitude of basal insulin daily dose adjustments within the 90-day window preceding HbA1c measurement. We use a linear mixed-effects model to analyze associations between frequency/magnitude of daily basal insulin changes and HbA1c.
Results:
We present data on 114 adult (44 ± 17 years, 60% female) and 212 pediatric (12 ± 4 years, 50% female) patients. Individuals changed their basal insulin dose on 72%-94% (interquartile range [IQR]) of observed days relative to the previous day. These changes varied 0.6%-2.4% IQR from the previous day’s value. In pediatric patients, lower HbA1c was associated with more frequent daily profile adjustments, while controlling for rate of hypoglycemia (z = -3.2, P = .001). In adults, there was no relationship between HbA1c and magnitude or frequency of basal profile adjustments.
Conclusions:
Pediatric patients who frequently modify their basal insulin exhibit somewhat better clinical outcomes, although the magnitude by which their basal amount is changed does not contribute to this effect.
Introduction
Optimizing insulin management for type 1 diabetes (T1D) to improve glycemic outcomes requires a substantial amount of patient self-management. 1 Traditionally, insulin doses are adjusted at quarterly endocrinology visits, but more frequent adjustments between visits may be needed to improve glycemic control. Education programs for empowering individuals with T1D to actively manage their insulin intake between visits (eg, Dose Adjustment for Normal Eating, 2 Treat-to-Target Trials 3 ) have been shown to be effective at improving both user confidence in insulin management 4 and blood glucose control.5,6 However, past work has not shown that patients who regularly adjust their insulin regimes experience improved glycemic outcomes. We are unaware of any observational studies that have looked directly at open-loop insulin pump dose changes and their association with glycated hemoglobin (HbA1c). There remain significant gaps in our understanding regarding (i) the extent to which individuals proactively manage their pump profile settings between clinic visits and (ii) the impact on outcomes. Past studies have also generally involved randomized trails (performed at a small scale under possibly unrealistic conditions); this type of work has not been extended to real-life clinical care populations.
In this study, we characterize proactive insulin management behavior and its impact on blood glucose management through a retrospective cohort study consisting of individuals with T1D seen in a clinic. We sought to measure the frequency of and degree to which an individual makes changes to their basal insulin profiles and evaluate the association between those changes and HbA1c. Given the retrospective nature of our study, we focus on changes to basal insulin (as opposed to bolus adjustment), since such changes are more readily extracted from pump management systems. We hypothesized that patients who made more frequent basal profile changes would exhibit lower HbA1c without an increased rate of hypoglycemia.
Methods
Participants
This study was approved by the University of Michigan Medical School Institutional Review Board. This single-center retrospective cohort study included individuals with T1D seen in the Michigan Medicine adult and pediatric diabetes clinics between September 2012 and December 2019. Patients with type 2 diabetes were excluded. Inclusion criteria targeted populations who used an insulin pump and were adherent to treatment recommendations. Patients without insulin pump data in the Glooko-Diasend platform were excluded. We describe daily adherence as follows: recording at least three carbohydrate input measurements, three blood glucose entries, and three bolus amounts on that particular day. Observation periods (90-day windows leading up to each HbA1c measurement) were excluded if the patient did not meet our definition of adherence in more than half of the days (ie, ≥45 days). In addition, we excluded observation periods with an HbA1c >10% since adherence issues could skew the calculations. If a participant had multiple HbA1c values within 90 days of each other, we included only the earlier measurement to avoid overlapping windows. Each individual could have multiple observation periods (ie, comparisons were done at the 90-day period level). In a secondary analysis studying hypoglycemia, we excluded windows that did not have at least 14 days with more than 70% of the daily continuous glucose monitor (CGM) data (>201 five-minute intervals).
HbA1c measurements obtained at regular clinic visits were extracted from the electronic health record (EHR). Daily basal insulin dose intake from insulin pumps was downloaded from the Glooko-Diasend diabetes management software platform. We included all devices integrated with Glooko-Diasend (this excludes Medtronic and Tandem pumps, which were not compatible with the system during the study period).
Outcomes
The primary outcome variable was HbA1c, either based on point-of-care results or laboratory testing. For patients with sufficient CGM data, we calculated the proportion of time hypoglycemic as the proportion of CGM measurements less than 70 mg/dL during days with at least 70% CGM data observed.
Study Definitions
We studied daily changes made to the basal profile. We defined a change based on the total daily basal insulin. The frequency of change was calculated as the percentage of days over the 90-day period that differed from the previous day. The magnitude of change was calculated as the median percent difference of total basal insulin between consecutive days in which a change was observed (Figure 1). In our calculations, we included only consecutive days in which both days met our adherence criteria.
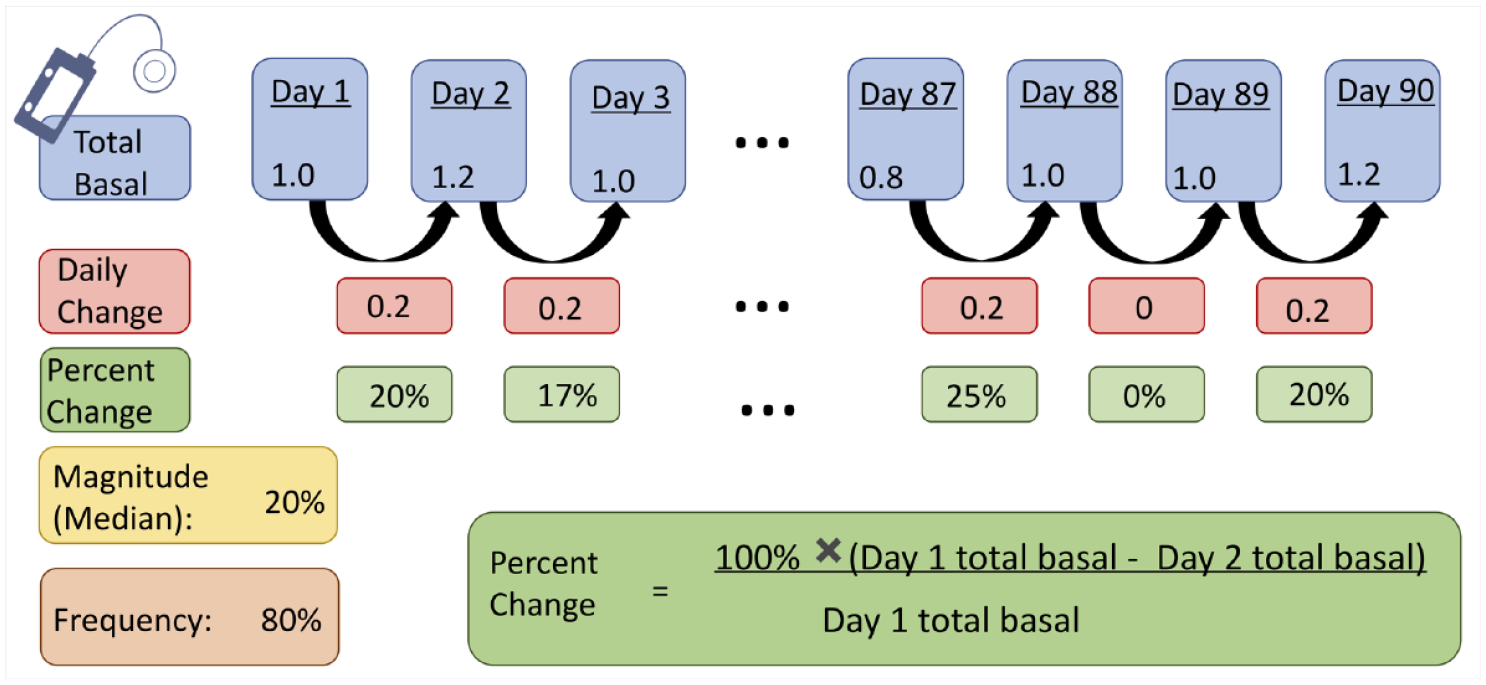
Illustrated calculation of pump metrics. Frequency of change is calculated as the proportion of days with a different total basal value from the previous day, while magnitude of change is the median percent difference from the previous day across all pairs of days. Days with the same total basal value as the previous day were not included in the median calculation.
Analyses
First, to characterize changes to the total basal insulin, we independently examined the empirical distribution of the frequency and magnitude of those changes in our adult and pediatric cohorts. Furthermore, we compared the frequency and magnitude of changes directly, by stratifying 90-day windows into quintiles based on frequency of change and examining the distribution of the magnitude within each quintile.
Second, we measured the correlation between both the frequency and the magnitude of daily basal profile changes with the outcome (ie, HbA1c). To control for repeated measurements across individuals, a linear mixed-effects model was used with HbA1c as the dependent variable, frequency or magnitude of profile changes as an independent variable, and patient as group. We used quintile number in place of raw frequency or magnitude values, in order to account for the observed skewed distributions. In a sensitivity analysis, we repeated the analyses described above, but did not exclude windows in which the HbA1c >10%. P values were calculated with a null hypothesis that the two variables had no dependence, with an alpha level of 0.05. Analyses were performed using statsmodels in python-v3.7.3.
For windows with a sufficient amount of CGM data, we repeated the analysis comparing HbA1c and frequency of profile changes, while controlling for proportion of time spent hypoglycemic. In addition, we repeated our linear mixed-effects model analysis with time hypoglycemic as the outcome.
To examine if the association between HbA1C and frequency of basal rate adjustments might be explained by other behaviors, we measured the correlation between the average number of boluses recorded per day and (i) the HbA1C and (ii) the frequency of basal rate adjustments.
Results
Of the initial 2274 pediatric and 12 955 adult individuals seen in the clinic from September 2012 to December 2019, 212 and 114 met our inclusion criteria, respectively (Figure 2). The majority of exclusions were due to a lack of insulin pump data availability (1673 pediatrics, 11 475 adults). Study population characteristics for both pediatric and adult populations are presented in Table 1. On average, individuals had 2.76 and 2.0 HbA1c measurements with sufficient pump data, corresponding to a total of 598 and 341 90-day windows, in the pediatric and adult populations respectively. Although two to three HbA1C measurements on average are seemingly few for a seven-year period, no patient had data available for the full study period, and most patients only had data available for a significantly shorter duration (less than six months on average). Many 90-day windows preceding HbA1C measurements were excluded because the patient did not meet our strict adherence criteria.

Patient inclusion flowchart, pediatric and adult. The majority of exclusions in both populations (74% pediatrics, 89% adults) were due to a lack of information in the Diasend database. Most of the remaining exclusions (16% pediatrics, 10% adults) were due to a lack of treatment adherence.
Population Characteristics.

All measurements at the patient level, except HbA1c which is calculated at the window level.
Abbreviation: HbA1c, glycated hemoglobin.
In our pediatric cohort, 97% of 90-day observation periods had more days that differed from the previous day than those that did not (IQR 72%-94%) (Figure 3a). The total amount of basal differed from the previous day by less than 2.5% in the majority of cases (IQR 0.6%-2.4%) (Figure 3b). When comparing the frequency of change with the magnitude of change, we found a significant positive correlation z = 6.4, P < .001, (Figure 3c); individuals who make many changes also make larger changes. Frequent changes were associated with lower HbA1c (Figure 3d), (z = -3.4, P = .001), with windows in the upper two quintiles having an average HbA1c of 7.8% (5.3-9.9) vs 8.2% (6-9.9) in the lower two. We found no statistically significant relationship between magnitude of change and HbA1c (Figure 3e) (z = -1.2, P = .23).
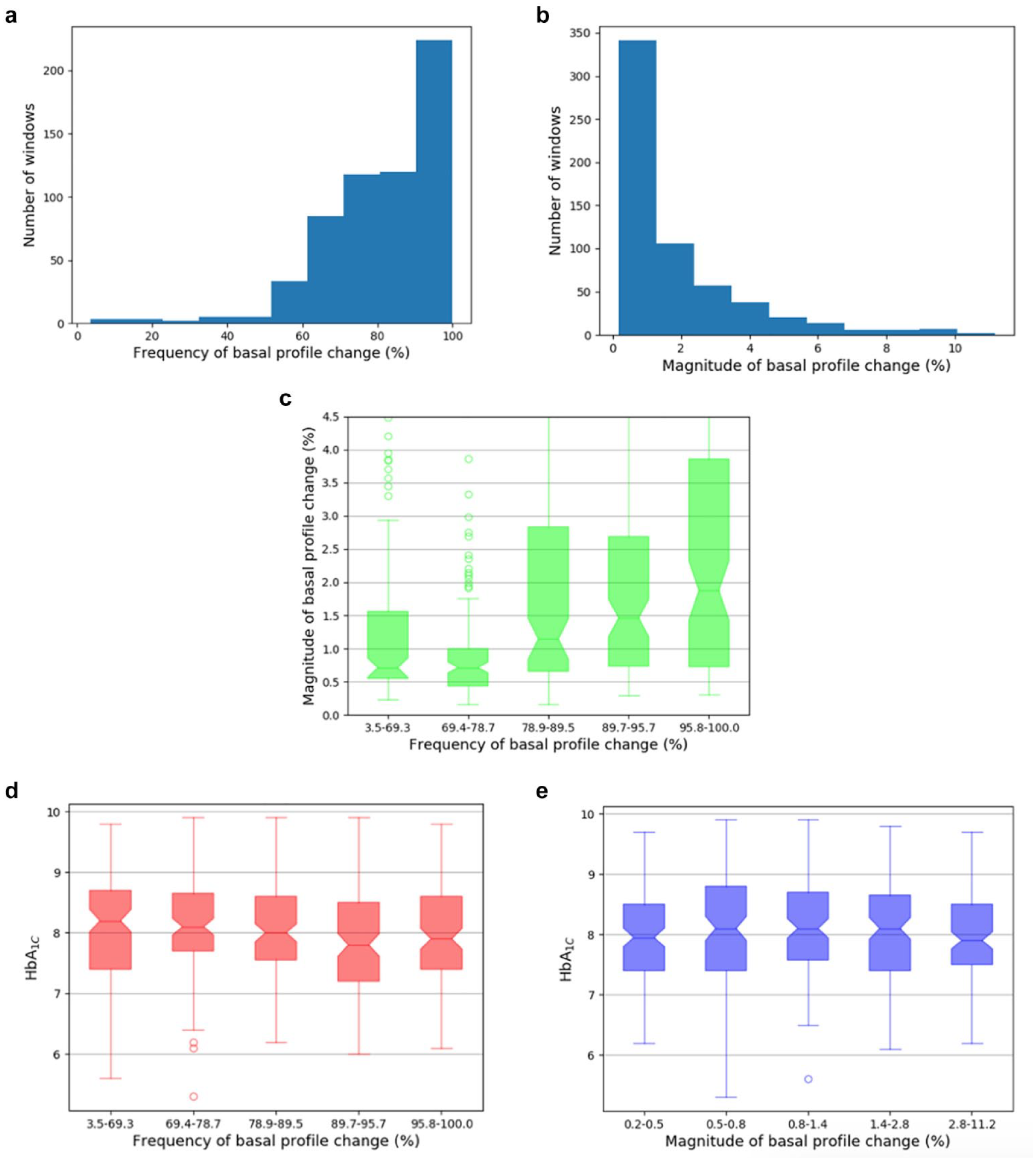
Results for pediatric population. (a) Distribution of frequency of basal profile changes: for most windows, the majority of days have different total basal values from the previous. (b) Distribution of magnitude of basal profile changes (across days with any changes). Most median changes are of fairly low magnitude. (c) Distribution of daily basal amount changes; magnitude vs frequency of change. (z = 6.4, P < .0001). (d) HbA1c vs frequency of basal profile change. Patients who change their basal profiles more frequently tend to have lower HbA1c (z = -3.4, P = .001). (e) HbA1c vs magnitude of basal profile change. There is no linear association (z = -1.2, P = .23).
For adults, 92% of observation periods had a majority of days that differed from the previous (IQR 69%-94%) (Figure 4a), and 75% of windows had a magnitude of change lower than 2% (IQR 0.4%-1.8%) (Figure 4b). Frequency and magnitude of basal change were not correlated (P = .18), and neither were significantly associated with HbA1C (Figure 4c-e).
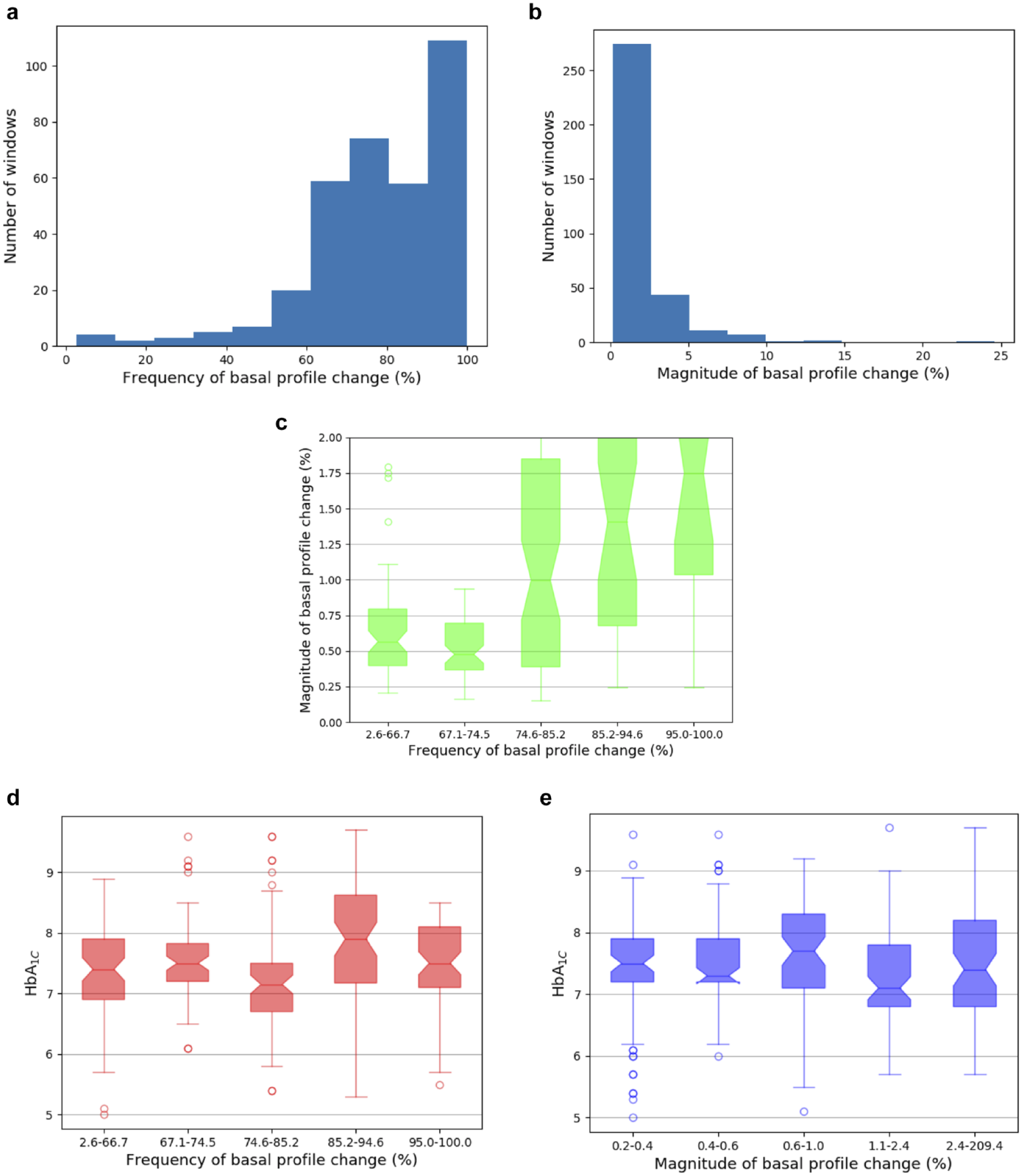
Results for adult population. (a) Distribution of frequency of basal profile changes: for most windows, the majority of days have different total basal values from the previous. (b) Distribution of magnitude of basal profile changes (across days with any changes). Most median changes are of fairly low magnitude. (c) Distribution of daily basal amount changes; magnitude vs frequency of change (z = 1.6, P = .18). (d) HbA1c vs frequency of basal profile change. There is no linear association (z = -1.5, P = .14). (e) HbA1c vs magnitude of basal profile change. There is no linear association (z = -0.76, P = .45).
Our findings in the pediatric cohort hold in repeated analyses where patient-windows with HbA1c >10% are not excluded; notably frequency of basal profile change and HbA1c are associated (z = -2.4, P = .017).
Within our study cohort, 56 and 29 patients had sufficient CGM data to analyze hypoglycemia, corresponding to 136 and 46 windows, for the pediatric and adult populations, respectively. Although the population with CGM data that was complete enough to use was relatively small, this analysis was included to examine hypoglycemia, since hypoglycemia is a risk factor that cannot be detected with HbA1c. For the pediatric population, frequency of basal profile change and HbA1c remained associated, after controlling for time hypoglycemic (z = -3.2, P = .001), but time hypoglycemic and frequency of basal change were not associated (z = 0.88, P = .38) (Figure 5). None of our findings in the adult population were statistically significant.
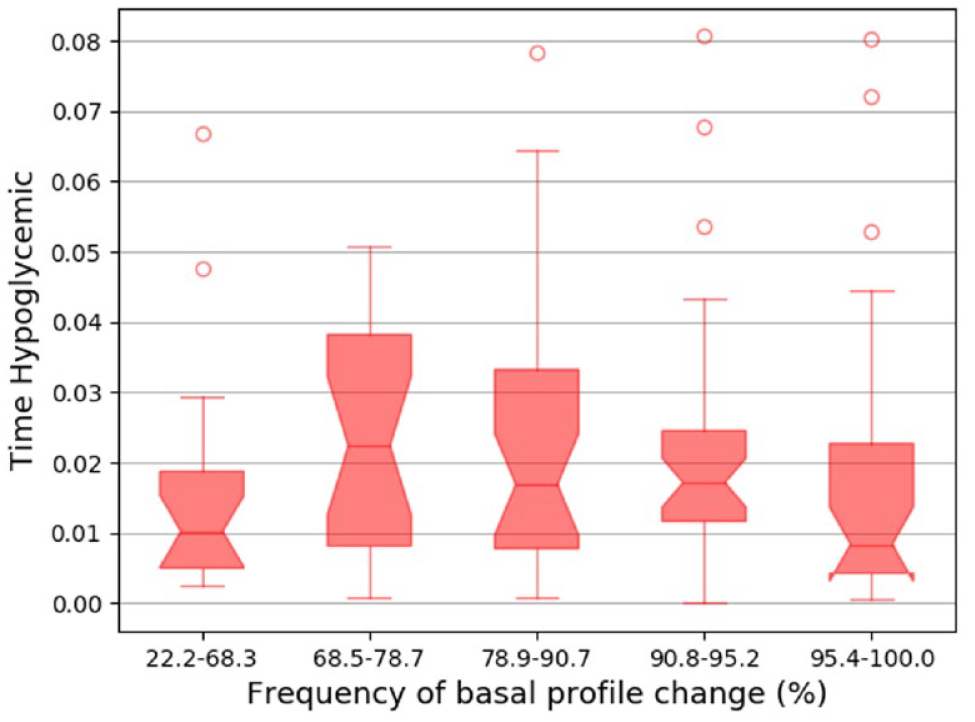
Proportion of time hypoglycemic vs frequency of basal profile change in the pediatric cohort. There is no linear association (z = 0.88, P = .38).
Neither HbA1c nor frequency of basal profile changes were significantly associated with average number of boluses (P > .5 for all analyses).
Discussion
Our finding that the frequency of pump basal profile changes is significantly associated with lower HbA1c and not associated with increased hypoglycemia in a pediatric cohort suggests that pediatric patients who perform more frequent day-to-day basal profile adjustments experience overall better outcomes, even if the magnitude of the HbA1c change may appear relatively modest. Although it is impossible to be certain of the cause of the observed basal profile adjustments (eg, factors such as pod changes and parental management strategies were not recorded), this finding matches clinical intuition in that children and adolescents often experience rapid growth and development during pubertal maturation necessitating frequent adjustment. Each patient follows a personalized approach to long-term dose adjustments, reflected at a daily, weekly, or monthly levels. Since nearly all patients make some profile adjustment every week, we analyzed differences in behavior at the daily level. We found no significant relationship between magnitude of daily change and HbA1c in either population, indicating that the degree of alteration is not necessarily a factor in this effect. Our observation of many daily pump changes over the 90-day windows might indicate the presence of one-time adjustments or suspensions, rather than long-lasting profile changes. This coupled with our findings regarding magnitude of changes indicates that even small, temporary changes can be beneficial, as long as they are frequent. Visual inspection of the basal profile data showed that the majority of days with observed changes had either pump suspensions or small changes in basal amount or timing (ie, changes of less than an hour or less than 20% for a small window).
The observed association between HbA1C and frequency of basal rate adjustments in pediatric patients is not necessarily causal. Such a relationship could arise if both HbA1c and frequency of basal rate adjustments shared a common cause. For example, patients who are more involved in their care overall may have both lower HbA1C and more frequent basal rate adjustments. Our exclusion criteria controlled for this to a certain extent. We included only those patients who were likely more adherent to treatment given that they bolused at least three times a day. Nonetheless, in a follow-up analysis, we found that neither HbA1C nor frequency of basal profile adjustments were associated with average number of daily boluses administered. We acknowledge that other factors such as more accurate carb counting could have contributed to improved blood glucose management, but the data do not permit us to examine this.
Our findings with regard to frequency of basal profile changes and HbA1c were not replicated in the adult population. This could be because adults do not have changes in body composition to the same extent as observed in children, or because adults exhibited lower overall HbA1c, leading to fewer required day-to-day insulin adjustments, or because parents monitor their children more closely than an adult might monitor themselves, and thus make more impactful changes.
We are unaware of studies that have directly examined basal dose changes and their correlations with HbA1c in a pediatric or adult population with T1D. Past findings about insulin management education and confidence rely on qualitative measurements, such as self-reported insulin dosage changes. Our findings complement these findings and expand on them by moving from qualitative to quantitative metrics.
With the right guidance, pump users who do not usually make regular updates to their profiles may be empowered to do so, and users who already do so could be encouraged to make these changes more effectively. Future work developing data-driven treatment-recommendation algorithms is necessary. Although artificial pancreas and similar systems have shown improvement in blood glucose control, 7 reliable closed-loop systems are likely many years away. Meanwhile, open-loop treatment recommendation algorithms have been widely used by individuals worldwide since the results from the Diabetes Control and Complications Trial demonstrating the beneficial effect of intensive therapy on the long-term complications in patients with T1D.8,9 Systems that recommend profile changes when necessary are therefore immediately actionable and widely applicable. Individuals with T1D who do not have insulin pumps or CGMs are unable to use closed-loop systems and rely on open-loop recommendation and management systems.
This study is not without limitations. First, we did not account for comorbidities that affect HbA1c (eg, chronic kidney disease) or for factors that might affect basal profile changes including socioeconomic factors and access to diabetes education. The current standard of clinical care in diabetes recommends general education around insulin management, although there were changes in these recommendations over time during the course of data collection. It is important to note that all participants were part of an academic institution that as a whole has a long track record of implementing measures to ensure adherence to the current standard of care, and also benefits from accredited diabetes education programs for both the pediatric and adult populations. Thus, these could have contributed to raise the level of engagement of the cohort analyzed. However, we do not have granular information as to what extent specific individuals were educated on how to actively titrate insulin dose including basal rates on their own. While it might be interesting to consider how our findings hold across different subgroups of participants, our current cohort is too small to support such analyses. Second, we did not account for the fact that some individuals may have been using CGM-augmented automatic pump systems. These data were unavailable in our sample, but it is unlikely that more than a few (if any) individuals were using such systems in our cohort since the majority of patients using such systems are in Tandem or Medtronic, which were not included. Based on the availability of CGM data, we estimate that at least 42% and 34% of pediatric and adult patients, respectively, used a CGM at some point during data collection. Third, with our dataset, we are unable to determine definitively if more frequent day-to-day basal profile adjustments led to better clinical outcomes, or vice versa. However, either causal direction would signify an interesting relationship. Fourth, our analysis was restricted to changes in basal insulin. Without direct access to pump profile settings, we did not have the ability to evaluate changes to bolus insulin (eg, carbohydrate ratios). Studying the effects of profile changes to bolus insulin presents an interesting future direction, although our work is still widely relevant, since basal insulin generally represents around half of administered insulin. Finally, we limited our study cohort to those patients with sufficient treatment adherence, and thus our findings may not generalize to patients who are less active in their treatment management, although such patients do not necessarily represent the norm.
Conclusions
Our findings highlight that pediatric insulin pump users who implemented more frequent daily basal insulin changes in their treatment management experienced slightly decreased HbA1c without an increase in the incidence of hypoglycemia. Treatment strategies aimed at empowering users to make more self-directed day-to-day basal pump adjustments could lead to further improvements in patient outcomes.
Footnotes
Abbreviations
CGM, continuous glucose monitor; EHR, electronic health record; HbA1c, glycated hemoglobin; IQR, interquartile-range; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Lee serves as a consultant to T1D Exchange, has received grant funding from Lenovo, and is on the medical advisory board for GoodRx. All other authors have no relevant conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JDRF, MCubed at the University of Michigan, and the Elizabeth Weiser Caswell Diabetes Institute at the University of Michigan.