
Abstract
Background:
Vascular assessment of the lower limbs is essential in patients with diabetes. In the presence of noncompressible arteries, the ankle brachial index (ABI) can either be inconclusive or provide false-positive results. Toe pressure measurement has been suggested as an alternative as a noninvasive method for detecting peripheral arterial disease (PAD). Toe pressure measurement can be performed either by photoplethysmography (PPG) or by Laser Doppler flowmetry (LDF). The aim of this study was to determine correlations between the two techniques in order to promote the use of PPG in clinical practice.
Methods:
This was a prospective correlational study of 108 consecutive recruited adult patients, with and without diabetes, with at least one lower limb wound from a University-affiliated hospital wound care clinic. Toe pressure measurements were both performed with PPG and LDF devices.
Results:
Mean toe pressure values for PPG and LDF were, respectively, 83.7 (SD 35.4) and 79.5 (SD 32.0) mmHg (with a paired t-test 3.969, P < 0.01). In patients with at least one lower limb wound, a strong linear relation was found between PPG and LDF toe pressure techniques with a Pearson’s r correlation coefficient of 0.920 (P < 0.001).
Conclusions:
PPG and LDF toe pressure techniques are equivalent in patients with at least one lower limb wound, irrespective of the presence of diabetes. Therefore, in the presence of an ABI with inconclusive results, such as in a patient with noncompressible vessels, both toe pressure techniques can be used for assessing the vascular supply of the lower limb with a wound.
Keywords
Introduction
Peripheral arterial disease (PAD) is a chronic vascular disease that can impact both the upper and lower extremities, yet occurring with greater frequency in the lower limbs. 1 About 200 million people worldwide are estimated to experience a lower extremity PAD. 2 Arterial disease occurring in the lower extremity often results in tissue ischemia and ulceration and is a significant barrier to the wound healing process.1,3 Patients who fail to heal may progress to gangrene and/or chronic limb-threatening ischemia (CLTI) and finally toward an amputation process.4-6 Due to its numerous impacts on patients and its socioeconomic burden, PAD demands a responsive approach to ensure the early detection, with noninvasive tests, and treatment.4,7,8
Current clinical guidelines recommend to perform a comprehensive vascular assessment of lower limbs with the ankle brachial index (ABI) in patients with a lower limb wound.7-10 However, the validity of this test is known to be suboptimal in the presence of medial wall calcification of the main arteries, especially in the population with diabetes.9,11,12 Moreover, noncompressible arteries may affect the ABI by providing falsely elevated or normal values in patients with diabetes, chronic renal insufficiency, or advanced age, 6 then with inconclusive, distorted results or potentially overestimating the actual vascular flow.
To a lesser extent, the arteries of the halluces are considered less prone to calcification, and accordingly, measuring toe pressure gives more accurate results with fewer false-positive values.13-16 Therefore, toe pressure is considered more sensitive than ABI in diagnosing PAD.6,16-20 Moreover, toe pressure has also been associated with amputation risk and cardiovascular mortality.21-23 Toe pressure can be measured either with a photoplethysmography (PPG) or with a laser Doppler flowmetry (LDF) device. 24 Reported normal toe pressure values are between 70 and 100 mmHg, and values to be considered for insufficient arterial blood supply are <30 mmHg or ≥100 mmHg. 25
Also, LDF is rated as being more precise, especially with lower toe pressures, as it assesses blood velocity, whereas PPG is based on opacity changes and changes in blood volume.24,26 However, the LDF device is more expensive, while PPG has a low cost, is rapid, simple to use, and has better portability. 27
Hence, we believe that corroborating the relation between PPG and LDF toe pressure measurement techniques could allow a further argument fostering the use of the measurement of the toe pressure in clinical practice. Therefore, the present study aims to determine the relation between the PPG and LDF toe pressure measurement techniques in patients with at least one lower limb wound, with and without a diagnosis of diabetes. Accordingly, the null hypothesis chosen depicts that there is no relation between the two types of toe pressure measurements.
Methods
Population Study
Patients, aged ≥18 years, having at least one lower limb wound were recruited for this prospective study and treated at the Complex Wound Care Clinic of a Canadian University-affiliated regional hospital, between May and August 2017. For the purposes of this study, patients were included if they had any kinds of wounds located on the lower limbs, irrespective of the diagnosis of diabetes, PAD, and CLTI. Patients with prior amputation of a hallux and/or patients with a wound located on a hallux were still recruited to this study, as those patients were recruited prospectively for a larger study not only regarding toe pressure measurement. Exclusion criteria included having a major neurocognitive disorder, or not being able to give proper consent to this study, and having received any previous hyperbaric oxygen treatment.
Institutional and University Ethics Board approvals (Université du Québec à Trois-Rivières CER-17-235-10.02) were obtained for this study. Written informed consent was obtained and documented from every patient retained in this study (including publication of images), according to the study protocol.
Measurements of toe systolic pressure using both techniques (PPG and LDF) were carried out in controlled conditions, as patients rested at least 20 minutes in the supine position in a room with a stable temperature between 20 °C and 22 °C while answering a questionnaire. Measurements were obtained from the hallux of each foot of all patients, except for those who had a wound on the proximal phalanx of the hallux or had their hallux amputated.
Toe pressure was first measured with PPG bilaterally at both digital dorsal arteries of the hallux, with a photoplethysmography probe adaptor (Huntleigh Doppler DMX Digital Doppler with Waveform, Arjo Inc., Addison, IL, USA). To do so, a sensor was attached to the tip of the hallux with a 10 × 10 cm adhesive tape (Mefix, Mölnlycke Health Care Canada, Oakville, ON, Canada). A small (UDC 1.9) or larger (UPC 2.5) cuff (Hokanson, Bellevue, WA, USA) was wrapped around the proximal phalanx of the hallux depending on its size (Figure 1a). When a cyclic waveform was detected on the monitor display, the cuff was inflated until the visible signal disappeared. Then, the cuff was slowly deflated until the cyclic waveform first reappeared. PPG then provided one measurement, corresponding to the toe systolic pressure.
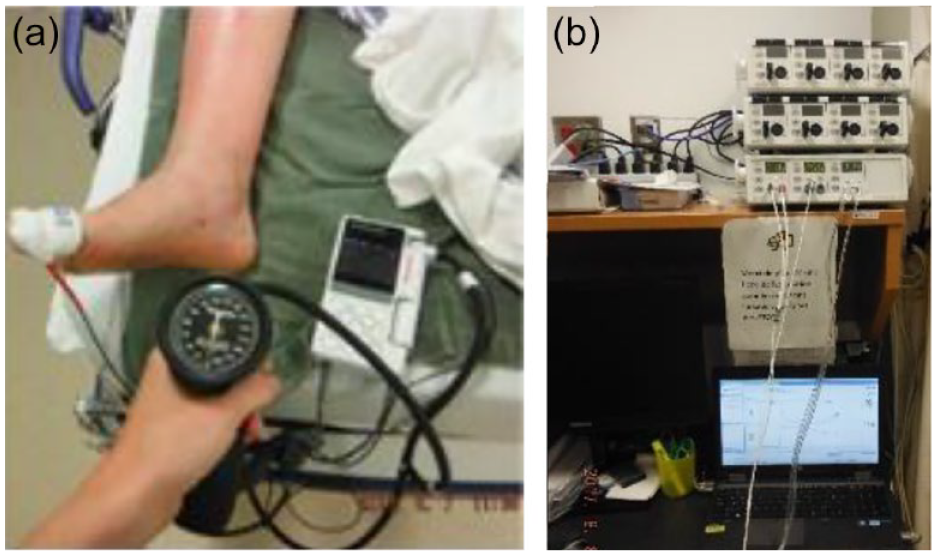
Measurement of toe pressure using the photoplethysmography device (a) and laser Doppler flowmetry device (b).
Then, measurement of toe systolic pressure using the LDF (Perimed PeriFlux System 5000 Doppler device, Perimed Inc., Ardmore, PA, USA) was completed thereafter, bilaterally, on the same digital dorsal arteries of both halluces. Probe 457 laser sensor was fixed to the tip of the hallux with a Perimed (PF 105-3) adhesive bandage. A small (UDC 1.9) or larger (UPC 2.5) Hokanson cuff was also used (Figure 1b). The LDF device was used according to the manufacturer’s instructions. 28 Measurement of toe systolic pressures using the LDF provided three consecutive readings for each hallux: toe systolic pressure corresponds to the average of these three measurements. The device was related to computer software (PeriSoft for Windows, Perimed Inc., Ardmore, PA, USA) which translates the measurements of toe systolic pressures on a graph and automatically calculates the mean value.
Statistical Analysis
Statistical analyses were performed with Microsoft Excel 2019 and SPSS software, Version 24, IBM, Armonk, NY, USA. For descriptive analyses, continuous data were reported as means, median, SD, and range (min-max), while categorical data were expressed as proportions. Paired t-tests were performed comparing mean toe pressure values for PPG and LDF techniques. Pearson’s r correlation coefficients comparing both toe pressure measurement techniques for each proper hallux side were calculated.
Results
A total of 108 patients with lower limb wounds were recruited in this study. Patients’ characteristics are represented in Table 1. Left and right PPG toe pressure measurements were obtained, respectively, on 100 and 96 patients, while left and right ones for LDF were obtained, respectively, on 100 and 98 patients. Figure 2 depicts the flowchart of the population under consideration and details specific reasons regarding exclusions. A total of 185 pairs of PPG-LDF data could be statistically analyzed. Mean toe pressure values for PPG and LDF were, respectively, 83.7 (SD 35.4) and 79.5 (SD 32.0) mmHg (with a paired t-test 3.969, P < 0.01), and their linear correlation was 0.920 (df = 183, P <0.001), confirming a strong linear correspondence between the two measures.
Patients’ Characteristics.
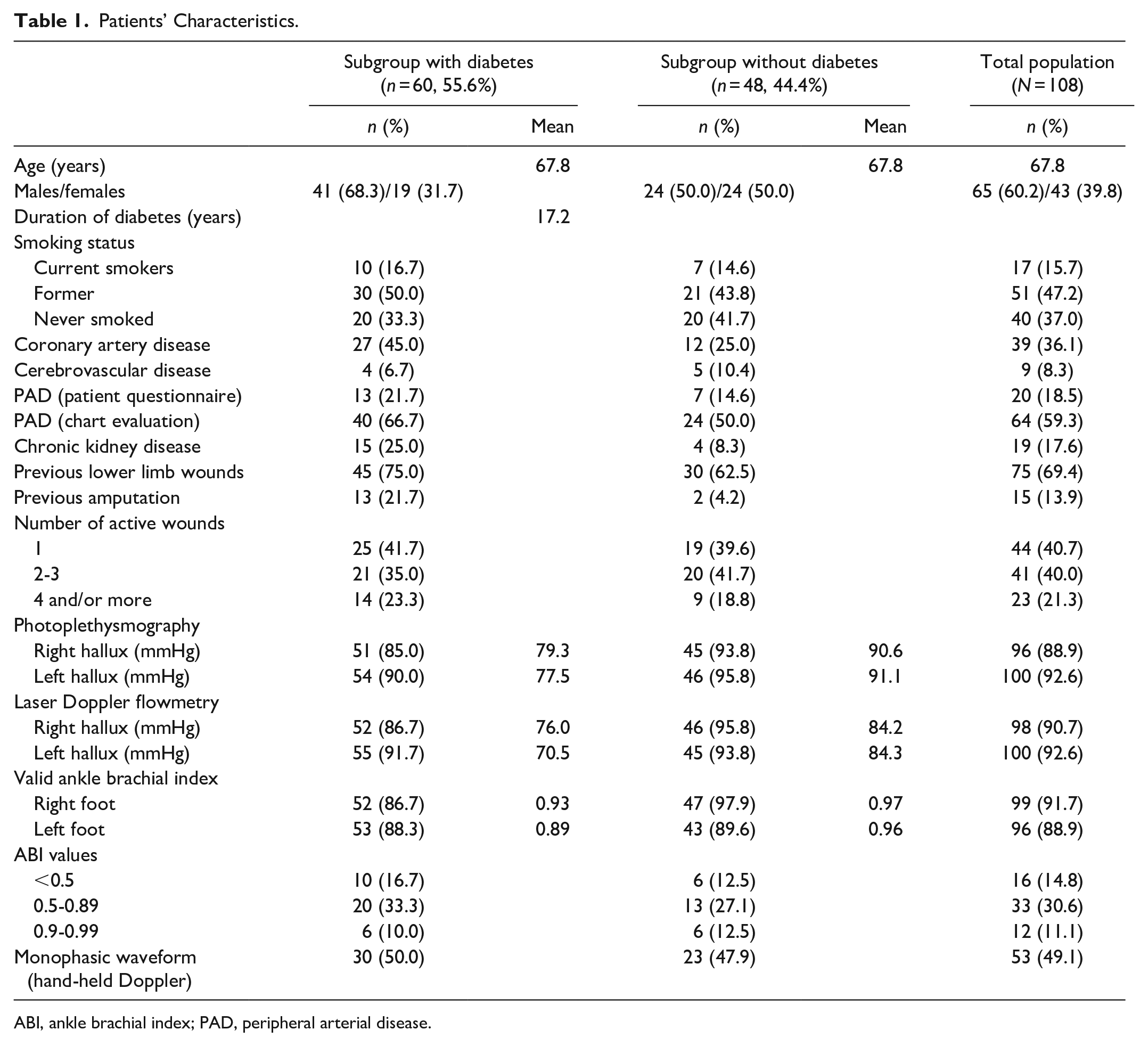
ABI, ankle brachial index; PAD, peripheral arterial disease.
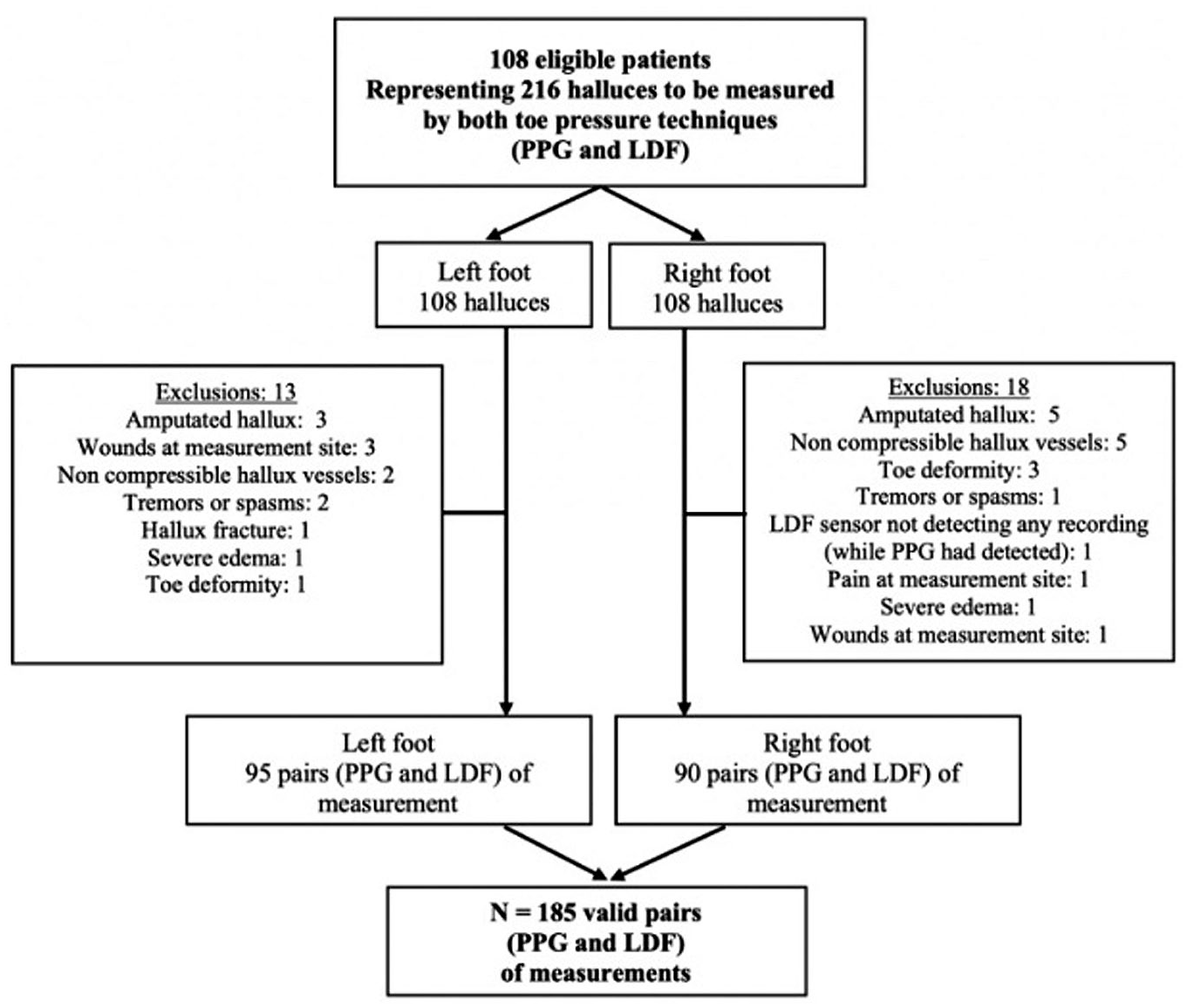
Flowchart of the cohort.
Three linear regression models were calculated to assess the degree of equivalence between the PPG and LDF toe pressure techniques. These models were analyzed using the data of the 185 pairs of measurements (from left plus right feet) of the two types of measurement. On the first model, we considered the correlation in a weighted linear relation (with a difference between the two measurement techniques); the second one was calculated also in a weighted linear relation (without considering a difference between techniques), and the third one was a direct score to score relation (Table 2).
PPG Versus LDF Toe Pressure Measurement Techniques.
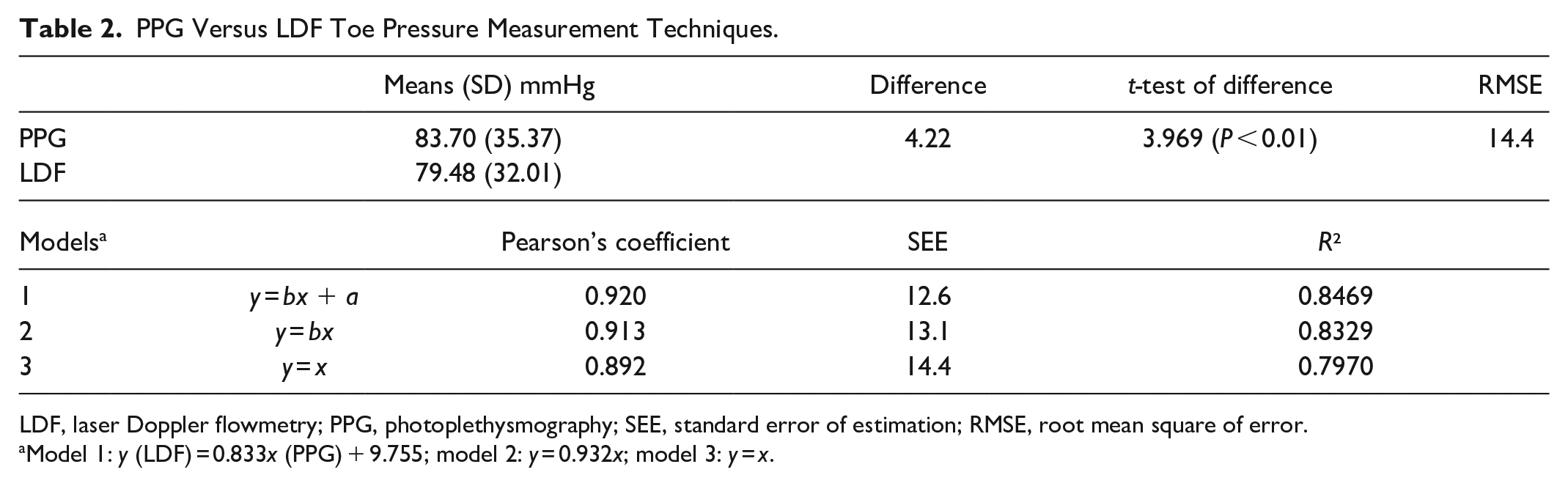
LDF, laser Doppler flowmetry; PPG, photoplethysmography; SEE, standard error of estimation; RMSE, root mean square of error.
Model 1: y (LDF) = 0.833x (PPG) + 9.755; model 2: y = 0.932x; model 3: y = x.
The relation between two types of toe blood pressure measurements, however good, could hardly be one-to-one, in as much as each measure carries its own uncertainty. Various parameters can also impact clinical data, notably the devices, the health-care providers performing the measurement, the kind of cuff used, the occurrence of keratosis on the toe, and the patient himself. Moreover, a significant difference between the two techniques is that the datum of LDF toe pressure is averaged from three measurements, whereas the PPG is obtained from one single measurement. Accordingly, it is appropriate to look for the global difference between the mean values issued from the two procedures. The mean difference observed (Table 2) is 4.22 mmHg and, albeit systematic (t-test = 3.969, P < 0.01), represents only 12.5% of the combined observed scatter of both measurements. At the same time, obviously, we cannot simply consider the results of PPG and LDF measurements as equivalent, as the observed difference must be taken into account. Thus, our third model is invalidated.
Statistical results confirm a strong linear relationship between the PPG and LDF toe pressure techniques in the three models, with Pearson’s correlation coefficients of 0.920, 0.913, and 0.892, with further confirmation from the convincing scatterplots in Figure 3a and b (with R², respectively, of 0.847 and 0.833). This also reflects that a very large portion of the LDF measurements can be predicted by the PPG data, and conversely. 29
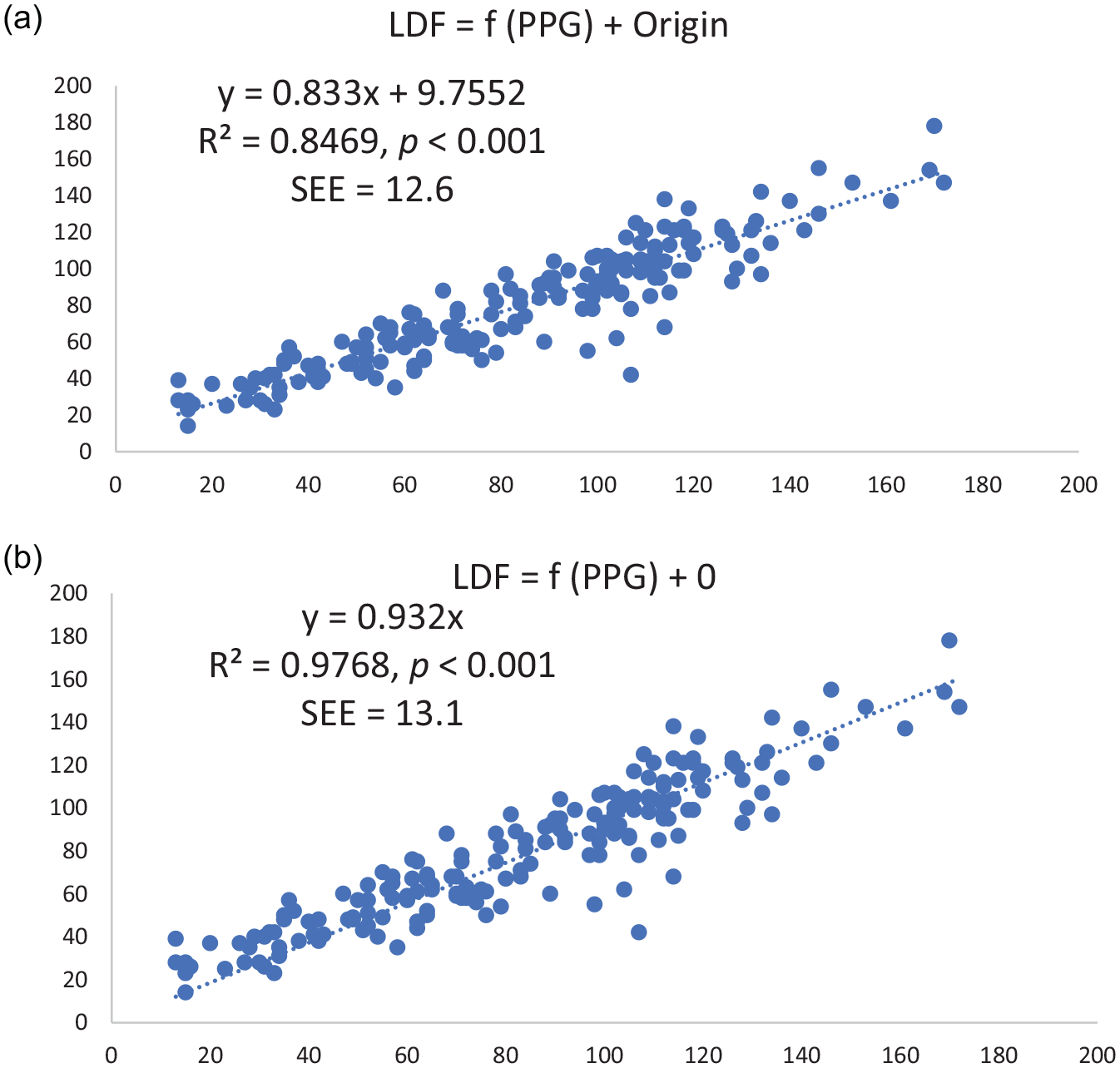
(a) Correlation between laser Doppler flowmetry and photoplethysmography toe pressure values (model 1). (b) Correlation between laser Doppler flowmetry and photoplethysmography toe pressure values (model 2).
In detail, the standard error of estimation which reflects the accuracy of models’ prediction is approximately of 13 mmHg for models 1 and 2. This amount of residual error in the models could be ascribed to random variation or lack of precision of the PPG data if the stability or purity of the LDF data were ascertained, which is not the case. Indeed, even if the PPG technique is liable to a greater dose of wavering (with a somewhat larger variance, ≈22%), there are still sources of random variance for the LDF technique which could explain some part of this residual (and random) error. Model 3, with a zero imposed origin, assumes that the two techniques have no mutual differences, contrary to the demonstrated difference of ~4 mmHg, and the (hidden) coefficient b=1, that the two techniques use the same measurement scales, producing the same approximate variance. The root mean square of error (RMSE) of 14.4, higher than the standard error of estimation (12.6) of the full model 1, reflects these differences. In model 2, the function with origin zero has a better slope (0.932), closer to 1, than that of model 1, and its standard error is not noticeably increased. However, the inescapable and significant non-zero difference invalidates model 2. Overall, model 1 offers the statistically best rule of correspondence between our PPG and LDF toe pressure measurements as depicted by a Pearson’s correlation coefficient of 0.920 (P < 0.001), and accounting both for the relative difference between the two procedures and the somewhat larger variance for the PPG measurements versus the smaller variance for the LDF measurements (t = 3.451, df = 183, P < 0.01).
Finally, correlational subgroup analyses were performed for PPG and LDF values. Pearson’s coefficients were 0.835 for patients without diabetes and 0.901 for patients with diabetes.
Discussion
This study has examined the statistical relation between the PPG and LDF toe pressure techniques with patients having a lower limb wound, either in the presence or the absence of diabetes. Our study highlights that these two techniques have a strong linear correlation. It also upgrades the validity of both techniques for its important purpose in clinical practice, especially in patients with diabetes, when assessing lower limbs’ vascular supply. Our study also supports toe pressure use, as almost every patient had the examination performed, independently of the arteries compressibility. Both subgroup analyses also revealed strong linear correlations in a subgroup of patients with and without diabetes.
The difference of 4.22 mmHg seen in mean toe pressure values for PPG and LDF was minimal. However, this difference could be judged not clinically significant, as a strong linear correlation was notably found between the two techniques.
Our results may have been different in other types of populations. It should be remembered that toe pressure measurements were performed in a population of patients from an interdisciplinary wound care clinic from a University-affiliated hospital. Accordingly, every patient presenting with at least one lower limb wound of different etiologies was included. Patients’ characteristics also reflect that more than half of the population had a diagnosis of PAD, and the ABI values reflect the spectrum of PAD. That difference could have been potentially greater if more end-stage PAD patients were recruited. Also, it should be noted that toe pressure measurements were not possible to be obtained or performed for 9.3% (20/216) of patients with the PPG and for 8.3% (18/216) of patients with the LDF.
Toe pressure measurements being recommended, a few other studies examined the relation between plethysmography and LDF techniques.26,30-33 A previous study examined the reliability and repeatability of toe pressures measured with LDF and with two different stationary PPG devices. 30 Authors reported that toe pressure values obtained varied greatly depending on the device used, but measure repeatability was acceptable. 30 Another previous study showed a good correlation between the LDF and strain gauge plethysmography in a population of patients with known or suspected PAD. 31 Our results concur with this last study, even though our population had a greater proportion of patients with diabetes. Other studies have also examined and demonstrated good correlations between LDF with PPG.26,32,33
However, our study had some limitations. First, the main inherent limitation of the instrument is that we were not able to measure toe pressure in individuals with amputated hallux. This is an obvious limitation, but for standardization purposes, we decided not to take a toe pressure measurement at the second toe, even if this is performed in clinical practice with patients with amputated hallux. Taking toe pressure measurements on the second toe could have potentially biased our results. Second, while toe systolic pressures are measured from rather objective devices, interpretation of results of both PPG and LDF devices is operator dependent. 1 Third, results pertaining to the PPG procedure could have been potentially different if three successive measurements had been taken instead of just one (as performed with the LDF technique). Fourth, results may have been different, if a greater proportion of patients with PAD or with end-stage CLTI was included.
Clinical guideline recommendations, such as TASCII, recommend using toe pressure measurement in addition to the ABI and transcutaneous oximetry for diagnosing PAD and CLTI. 1 While transcutaneous oximetry is considered being the most predictive for arterial microcirculation at the wound site of the lower limb34-40 and wound healing itself,36,38,40,41 it is not easily accessible.1,42,43 This emphasizes the importance of implementing toe pressure measurement for every health-care providers dealing with patients with risk factors of PAD or presenting with a lower limb wound. At this time, we may only surmise that proactive screening of PAD with toe pressure measurement is probably cost-effective in reducing cardiovascular morbidity and mortality. As Ubbink cited previously, the more we do, the better would be the detection of PAD. 32
Conclusion
In conclusion, the PPG toe pressure technique has a strong linear relation to the LDF toe pressure technique in patients with at least one lower limb wound, irrespective of the presence of diabetes. Our study adds validity and supports PPG toe pressure measurement in clinical settings when assessing the vascular supply to the foot. Therefore, in the presence of an ABI with inconclusive results, such as in a patient with noncompressible vessels, both toe pressure techniques can be used for assessing the vascular supply of the lower limb with a wound.
Footnotes
Acknowledgements
Thanks to the patients and the interdisciplinary team from the Complex Wound Care Clinic of the Centre hospitalier affilié universitaire Hôtel-Dieu de Lévis du CISSS de Chaudière-Appalaches and J. Vaillancourt Corp Ltd/Ltée, Médicanada from Verchères, Canada, for the donation of the photoplethysmography DMX Doppler toe pressure device.
Abbreviations
ABI, ankle brachial index; CLTI, chronic limb-threatening ischemia; DFU, diabetic foot ulcer; LDF, laser Doppler flowmetry; LEA, lower extremity amputation; PAD, peripheral arterial disease; PPG, photoplethysmography; RMSE, root mean square of error; SD, standard deviation.
Author Contributions
MB and LL contributed to the conception and design and statistical analysis. Data collection was performed by JB. MB, LL, and JP performed the analysis and interpretation. All the authors contributed to the writing of the article, critical revision of the article and final approval of the article.
Overall responsibility: MB.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.