
Abstract
Background:
The purpose of this study was with a simple clinical setting to compare skin temperature changes in the feet before and after revascularization and to identify possible correlation between ankle brachial index (ABI) and toe pressure (TP) values and foot skin temperature patient with and without diabetes.
Methods:
Forty outpatient clinic patients were measured ABI, TP, and the skin temperature using infrared thermography (IRT) at the foot before and after revascularization. Patients in the revascularization group were divided into subgroups depending on whether they had diabetes or not and a wound or not.
Results:
There were clear correlation between increase of ABI and TP and increase of the mean skin temperature on the feet after revascularization. The temperature was higher and the temperature change was greater among patients with diabetes. Side-to-side temperature difference between the revascularized feet and contralateral feet decreased after treatment. The mean temperature was higher in the feet with wound whether patient had diabetes mellitus or not.
Conclusion:
The simple, prompt, and noninvasive IRT procedure showed its potential as a follow-up tool among patients with diabetes or peripheral arterial disease and previous lower limb revascularization.
Introduction
Peripheral arterial disease (PAD) refers to atherosclerosis involving the aorta, the iliac artery, and the lower extremity arteries. The major risk factors for PAD are also common to other atherosclerotic diseases. They include smoking, diabetes mellitus (DM), renal failure, dyslipidemia, and aging.1,2 The natural course of chronic disease is difficult to predict. Symptoms do not always progress gradually from the severity to the next. Approximately half of patients suffering from critical ischemia have previously suffered symptoms of claudication and the first symptoms might be pain at rest and/or ulcers. DM is strongly associated with PAD. Among people with diabetes, PAD rate shows to be 11% compared with 4% among those without diabetes.3,4 Critical limb ischemia portends a severe diminution in quality of life and is associated to a high rate of amputation and a marked increase in short-term mortality.5-9
An ankle brachial index (ABI) is the most used screening method for evaluating vascular disorders in lower limb. ABI < 0.9 is ~95% sensitive in identifying PADs that are detectable on arteriograms. 1 The high prevalence of medial sclerosis, which can render arteries incompressible upon cuff inflation, may lead to falsely elevated ABI values (ABI >1.4) in approximately one-third of patients with DM.4,10 In those cases, a measurement of toe pressure (TP) provides a more accurate estimation of circulation. Infrared thermography (IRT) has several advantages of being noninvasive, safe, and does not require physical contact.11-15 Skin temperature variations seem to be useful for identifying pathological situations especially in the diabetic foot.16-18 Strong asymmetry appears to be a sign of abnormality, whereas symmetrical bilateral distribution of skin temperature is physiological.19,20
Earlier studies suggest that IRT may be clinically feasible for estimating effective vascularization. IRT can be a revealing tool, especially among people with diabetes, and provides valuable information among PAD patients; however, temperature variation is not as broad as among patients with diabetes.21,22 Surgical or endovascular procedures for stenotic arteries of leg peripheral circulation are intended to lead to sufficient blood flow. The purpose of this study was with a simple clinical setting to compare skin temperature changes in the feet before and after revascularization and to identify possible correlation between ABI and TP values and foot skin temperature.
Methods
Subjects
Study participants were recruited by vascular surgeons from a heterogeneous group of patients at the outpatient clinic of the Oulu University Hospital between November, 2016 and May, 2018. Peripheral vascular status was evaluated during a routine clinical investigation. Evaluation included medical history, comorbidities, symptoms, and signs. Bilateral brachial blood pressure, ABI, TP, and toe brachial index (TBI) were measured in all patients. Examination also included routine duplex ultrasound flow measurement by a vascular surgeon. The extent of neuropathy was diagnosed mostly at the diabetic clinic. When clinical examination indicated a circulatory disorder, the assessment of arteries was performed by magnetic resonance angiography (MRA) or CT angiography (CTA). Some patients directed straight-forward procedure using digital subtraction angiography (DSA) and revascularization.
Participants were divided into two groups. Patients, who needed a treatment for a circulatory disorder, were assigned to the revascularization group (n = 40). All other patients, who had previously been treated with a satisfactory treatment outcome or who were considered to have sufficient follow-up without treatments, were included in the follow-up group (n = 14). The follow-up group could not be well matched in size of group to the other group because of difficulty in requiring subjects. Statistical analysis was performed between subgroups with DM (n = 21) or without DM (n = 19) and with a wound (n = 22) or without a wound (n = 18). According to the findings at MRA, CTA, or DSA, an appropriate revascularization method was selected according to generally accepted policies of treatment. Revascularization methods included percutaneous transluminal angioplasty (PTA), intra-arterial stent implantation, peripheral bypass surgery, and/or femoral thromboendarterectomy. A separate analysis was also performed according to the method of treatment: endovascular—PTA or stenting—and surgical—bypass or plasty—subgroups. After revascularization, patients were controlled at outpatient clinic on average one month. Patients underwent same investigation protocol at the first visit. After revascularization 11 patients had longer follow-up times with three or four visits. Patients were excluded from the study if they exhibited venous insufficiency requiring treatment, an active infection, or arthritis. Study protocol has been approved by the local Ethics Committee.
Thermographic Analysis
In this study, we prepared the vascular measurements according to the existing routine protocol at the outpatient clinic with constant room temperature (21°C-24°C). Before IRT, the patients were placed in a supine position maintained for 15-20 minutes during the routine vascular examinations. The camera was set about a distance of 1 m. IRT was performed on both the plantar and dorsal sides of the foot, at five circular sites with a nine-pixel diameter (Figure 1). The measurement sites roughly represented the angiosomal areas. All IRT measurements were recorded using a digital IR camera (FLIR A325sc) with a spatial resolution of 320 × 240 pixels, and a thermal resolution of 0.05°C. The IRT data were analyzed using the Thermidas Imager and FLIR ResearchIR programs.
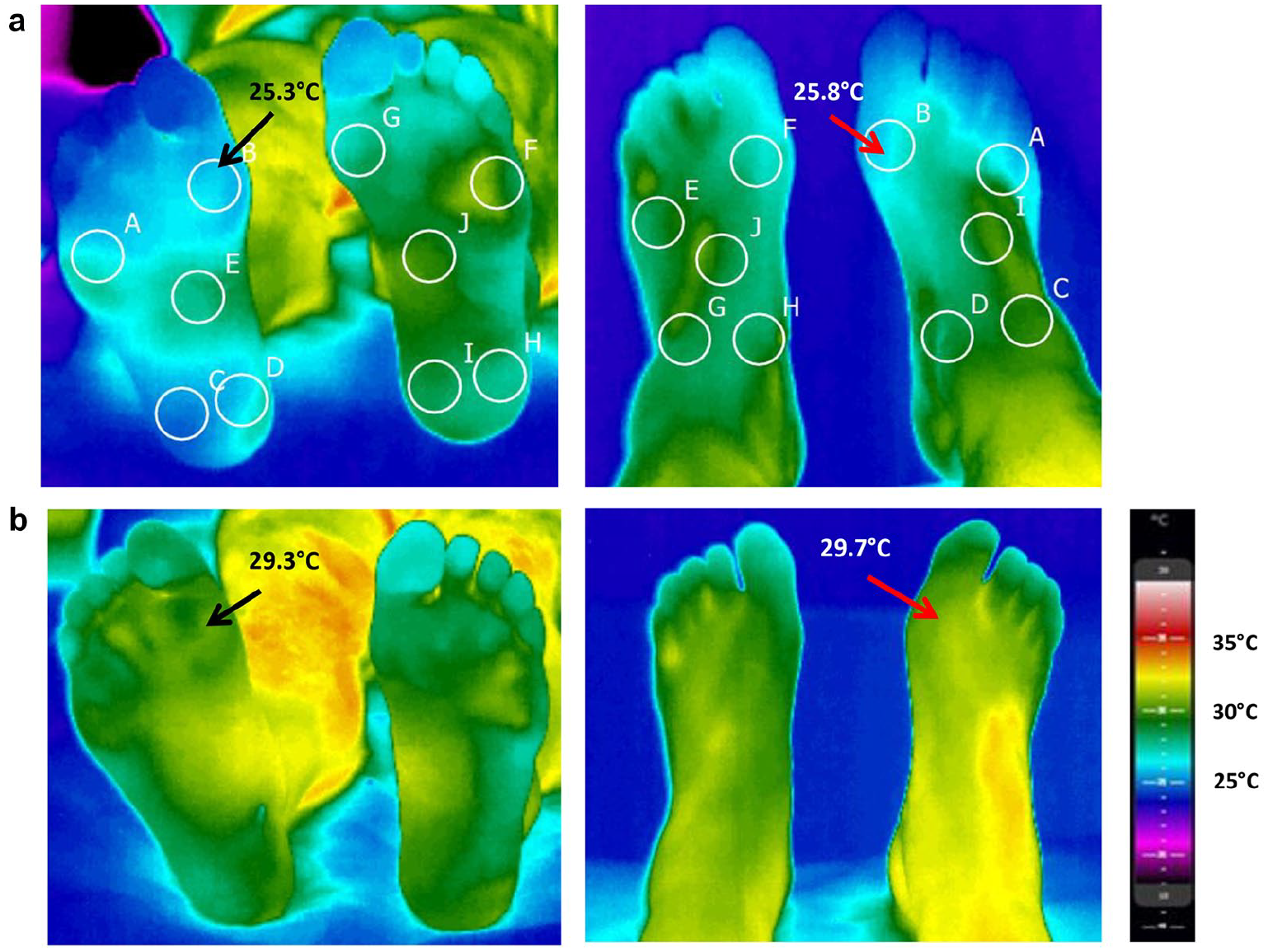
Infrared thermograms indicate temperature gradients. Five measured sites are shown (circles) on the (left) plantar and (right) dorsal surfaces. (a) The patient before revascularization—ABI 0.55 and TP 57 mmHg on the right side. (b) The same patient after treatment—ABI 0.75 and TP 78 mmHg on the right side.
Statistical Analyses
Continuous variables are expressed as the mean ± standard deviation, unless otherwise stated. Simple between-group comparisons were made using the t-test or Wilcoxon’s test for continuous variables and using Pearson’s chi-squared test for categorical variables. Two-tailed P-values are reported. Statistical analyses were performed with SPSS 25.0.
Results
In this study, 54 patients with 122 visits in the outpatient clinic were included. There were 40 patients in the revascularization group with a total of 50 procedures, some bilateral. The follow-up group included 14 patients with a total of 31 follow-up visits. The average follow-up period was 2 ± 1 months in the revascularization group and 6 ± 4 months in the follow-up group, three patients had a follow-up of one year. Table 1 shows the baseline characteristics. Among the study groups were 24 (43%) patients with diabetes, 2 (9%) of them with type 1 diabetes and 21 (91%) with type 2 diabetes, and 30 (57%) patients with atherosclerosis without diabetes. There were four previous amputations in the revascularization group—one major and three minor amputations.
Demographic data for the study population.
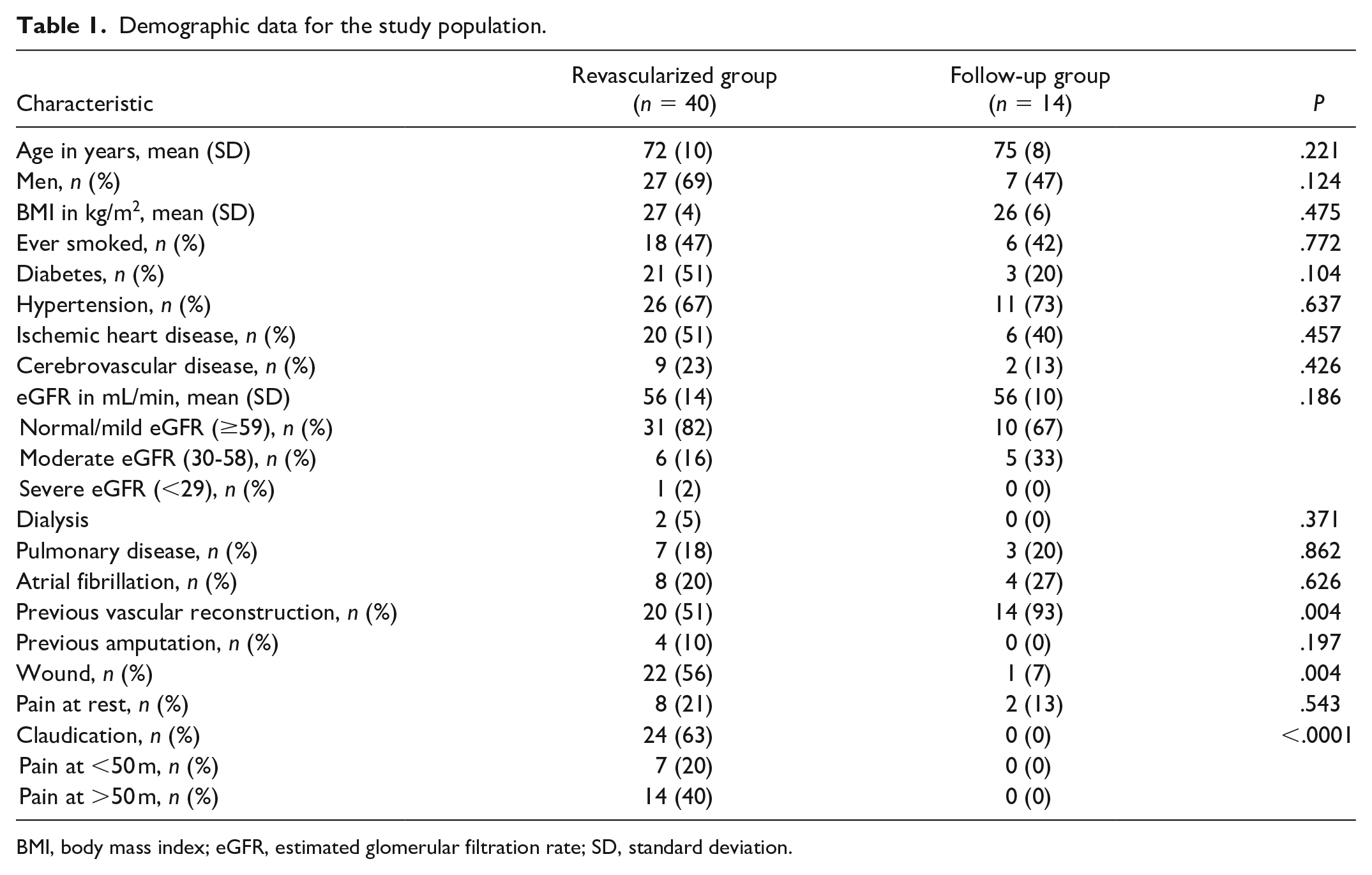
BMI, body mass index; eGFR, estimated glomerular filtration rate; SD, standard deviation.
After the operation, ABI, TP, and TBI increased significantly as expected (Figure 2). Patients with clear decrease in these measurement values (n = 3) had lost their revascularization result. In the revascularized legs the mean change before and after procedure was statistically significant in the ABI (0.28 ± 0.2, P < .0001), TP (21.6 ± 30.8 mmHg, P < .0001), and TBI (0.14 ± 0.19, P < .0001) measurements (Table 2). Also, the mean temperature increased after operation (Figure 2). In the revascularization group the mean temperature change before and after procedure was 0.5 ± 2.6°C (P = .02) on the plantar side and 0.6°C ± 2.3°C on the dorsal side (P = .03). The relation between the increase of the temperature and the increase of the value of ABI and TP in the revascularized foot is shown in Figure 3.
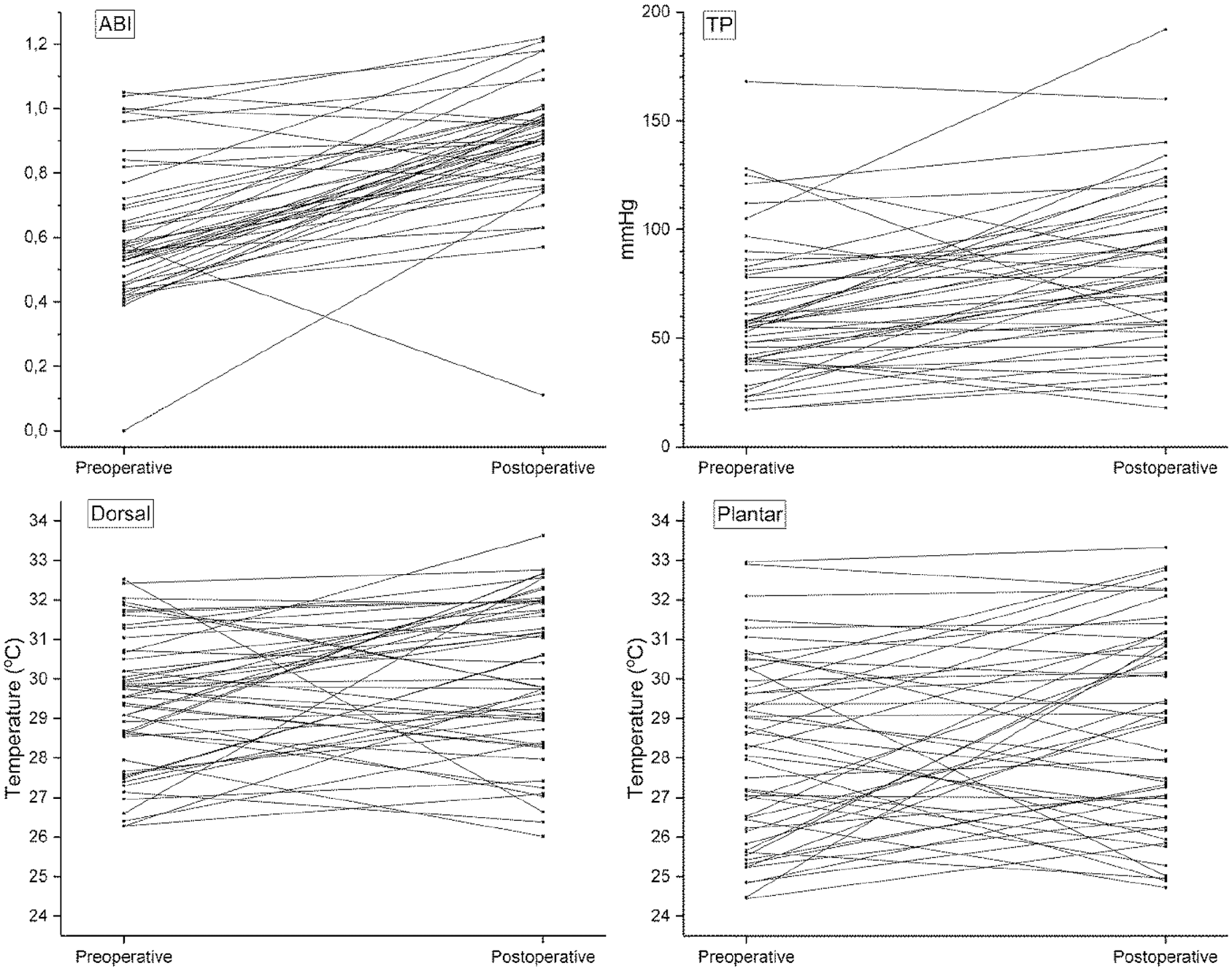
Differences in ankle brachial index, toe pressure, and temperature on the plantar and dorsal sides of the foot before and after the revascularization.
Changes in Values in the Revascularized and Follow-Up Groups. Values Before and After Mean Preoperative and Postoperative Measurements in the Revascularized Group and the First and the Second Visits in the Follow-Up Group.
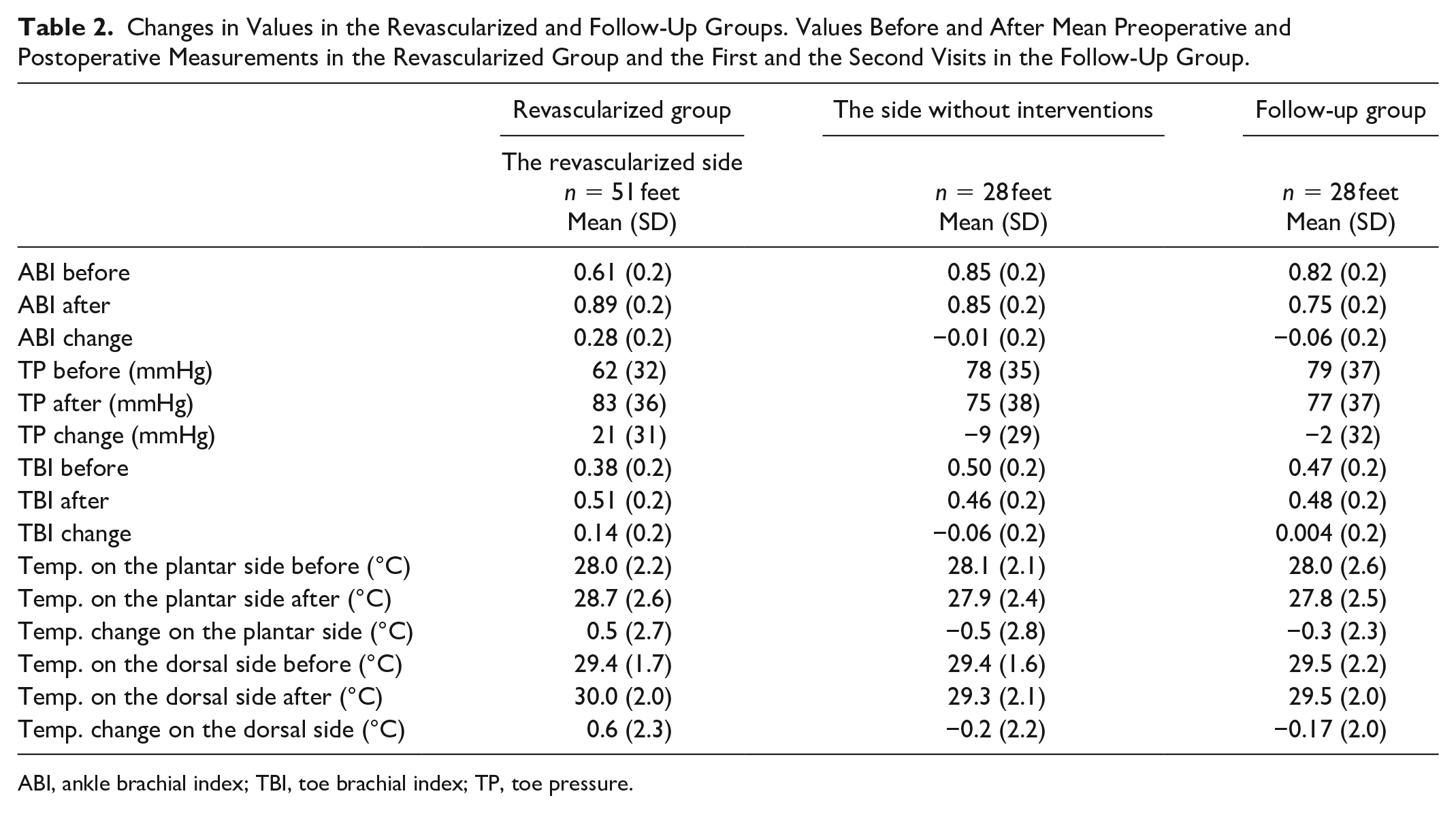
ABI, ankle brachial index; TBI, toe brachial index; TP, toe pressure.
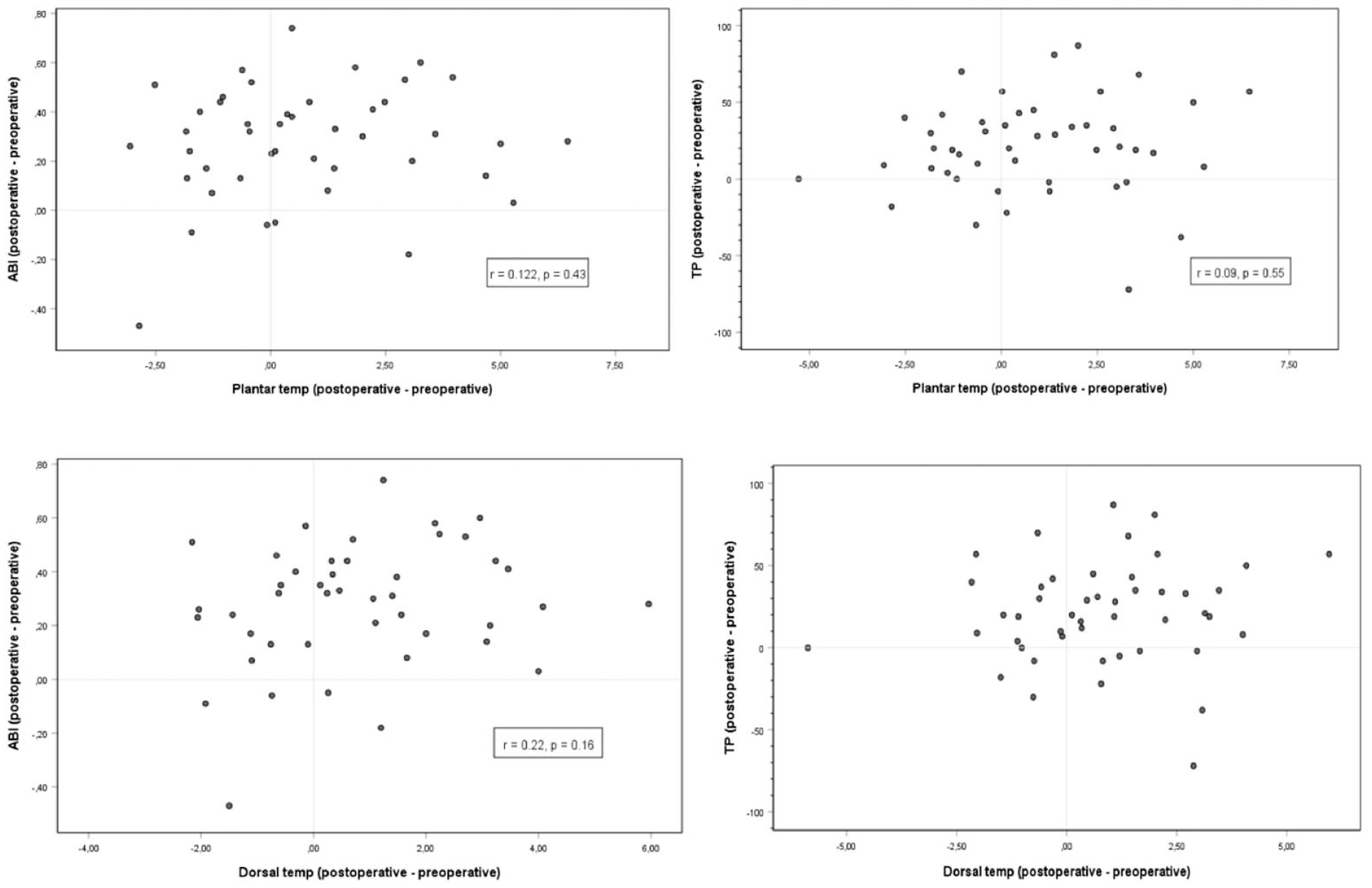
The relation of temperature differences before and after revascularization with changes in ankle brachial index and toe pressure.
Statistically significant differences were demonstrated in the data analyses comparing the revascularized foot to the contralateral foot. The temperature decreased in the contralateral foot. The mean temperature change in the contralateral foot was −0.52°C ± 2.8°C (P < .001) on the plantar side and −0.22°C ± 2.2°C (P = .002) on the dorsal side. In the follow-up group, changes in ABI, TP, TBI, and IRT measurements were slight, and there were no interventions necessary with regards any decrease in ABI, TP, or TBI during the follow-up period. The obtained results of ABI, TP, TBI, and IRT measurements are presented in Table 2.
Side-to-side difference between the skin temperatures of feet decreased after revascularization. On the plantar side, side-to-side difference was 1.3°C ± 1.1°C and on the dorsal side 1.2°C ± 1.0°C before procedure. After revascularization, side-to-side difference decreased and was 0.9°C ± 0.6°C (P = .02) on the plantar side and 0.8°C ± 0.6°C (P = .04) on the dorsal side. There were five patients with side-to-side difference increased over 1.0°C after treatment. Four of them had worsening critical ischemia on the contralateral side requiring additional measures and one was later diagnosed with osteomyelitis. In the follow-up group, side-to-side difference decreased slightly during the control period both sides on the feet. On the first visit it was 1.1°C ± 1.0°C and on the second visit 0.9°C ± 1.3°C (P = ns) on the plantar side and 1.2°C ± 1.3°C and 1.1°C ± 1.2°C (n = ns) on the dorsal side.
In a separate analysis, patients were divided into subgroups, based on DM or without DM. Patients with diabetes had more critical ischemia with lower baseline of ABI, TP, and TBI. The mean temperature before and after revascularization both on the plantar and dorsal sides was higher and change greater on the diabetic feet (Table 3). Thirteen patients with DM (62%) had neuropathy and three (14%) patients only angiopathy. Five (24%) patients had noncomplicated DM without distal angiopathy or neuropathy. There were more wounds in the diabetic feet (14 [64%] patients with DM and 8 [36%] patients with PAD without DM). Statistically significant differences were demonstrated using data analysis comparing the mean temperature of the affected foot (i.e. with wound) to the contralateral foot. In general, the mean temperature was higher in the affected foot whether or not they had diabetes. In patients with a wound, the change in ABI, TP, and TBI measurements was smaller than in patients without a wound, but with a greater change in temperature after revascularization.
Change of Values Between Subgroups With DM or Without DM and Between Subgroups With the Wound or Without the Wound in the Revascularized Group.
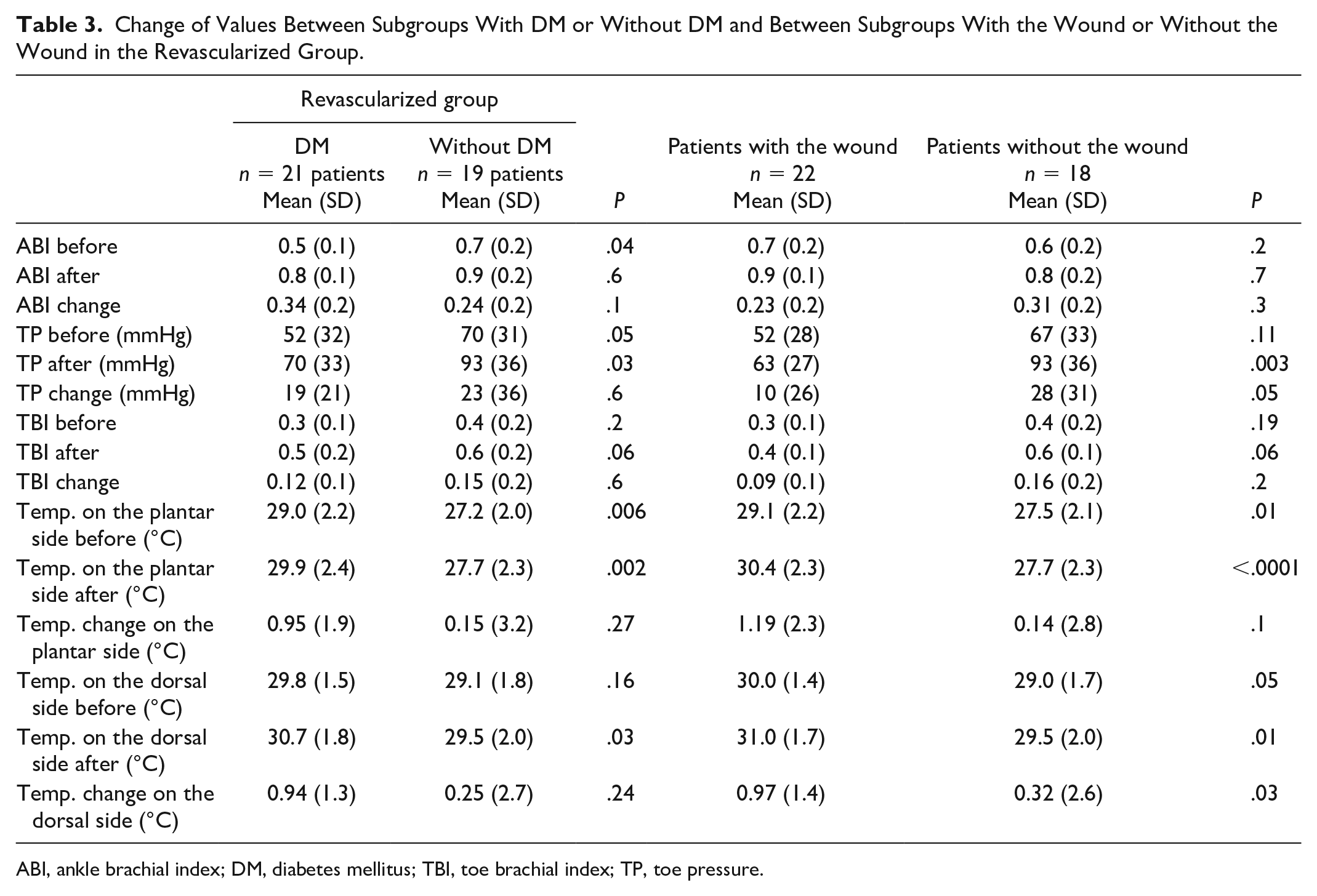
ABI, ankle brachial index; DM, diabetes mellitus; TBI, toe brachial index; TP, toe pressure.
The patients were treated with endovascular (39 legs, 78%) or surgical (11 legs, 22%) methods. There were no statistically difference between surgical and endovascular groups before and after revascularization in the ABI, TP, TBI, and IRT measurements. In the endovascular subgroup, the mean change was in the ABI 0.3 ± 0.2, TP 18 ± 31 mmHg, and TBI 0.1 ± 0.2 measurements. In the surgery group, the mean change was in the ABI 0.3 ± 0.1, TP 34 ± 26 mmHg, and TBI 0.2 ± 0.1 measurements. The mean temperature change was 0.6°C ± 2.8°C on the plantar side and 0.6°C ± 2.2°C on the dorsal side in the endovascular subgroup, and 0.5°C ± 2.3°C on the plantar side and 0.8°C ± 2.0°C on the dorsal side in the surgery subgroup.
Discussion
The present study yielded three major findings. First, there were clear correlation between increase of ABI and TP and increase of the mean skin temperature on the feet. Second, the side-to-side difference in skin temperature between the revascularized feet and contralateral feet without any interventions decreased after treatment. Third, the mean temperature was higher in the feet with wound whether patient had DM or not.
The purpose of this study was to describe the thermal changes of foot by using IRT in patients before and after revascularization and to compare these IRT measured thermal changes with the determination of ABI and TP. The presence of PAD is defined as a nonpalpable pulse and an ABI of <0.9, which are widely used criteria for the screening and diagnosis of PAD. TP or TBI is the recommended measurement for PAD assessment in people suspected to have arterial calcification.1,2,23 IRT effectively revealed differences in temperature between different skin areas and IRT can characterize temperature gradients of regions affected with vascular disorders.24,25 Staffa et al reported about the correlation between the surface temperature obtained by the IRT and ABI in the case of limbs treated by PTA. 26 Our present results support previous findings. The change of ABI, TP, and TBI is associated with the change of skin temperature in the revascularized leg regardless of whether an endovascular or surgical method was used. In clinical decision making the method of treatment chosen will be most affected by the artery to be targeted and the severity of the PAD disease, but also by the patient’s general condition and other comorbidities. In this respect, the groups may not be identical. However, this did not affect the correlation between ABI and TP measurements and skin temperature. In summary, revascularization enhanced lower limb circulation, which was confirmed by ABI and TP. At the same time, skin temperature increased, as measured with IRT .
Skin temperature normally shows symmetrical bilateral distribution; thus, strong asymmetry indicates an abnormality.19,20,27,28 Skin temperature variations of over 2.0°C may be useful for identifying pathological situations in the diabetic foot.24,29,30 Our present results showed the mean side-to-side difference between feet was higher before revascularization and diminished after the procedure. On the revascularized feet skin temperature increased and on the contralateral feet without any treatments skin temperature stayed stable or slowly decreased during the follow-up, so the difference narrowed and the asymmetry decreased. On those five patients with increase in the change of mean temperature over 1.0°C occurred new circulatory disorder or subclinical osteomyelitis during the follow-up period in the non-revascularized contralateral leg. In the follow-up group, asymmetry decreased slightly during the control period.
Increased local skin temperature is a classic sign of wound infection, repetitive trauma, and deep inflammation. Common clinical practice for temperature assessment involves manual palpation of the foot. However, the temperature changes are typically too small to be reliably determined by hand. Thermography has been used to monitor healing of Charcot’s arthropathy in diabetic feet.31,32 Hot and cold spots in the feet seem to be predictive of the development of ulceration. 14 Important risk factors for amputation include neuropathy (sensory, motor, or autonomic) and arterial disease with or without foot ulcer.9,33,34 In our earlier studies, we found that the skin temperature of the feet in patients with diabetes was higher than in patients with PAD or healthy controls. In particular, neuropathy and neuroischemia raised the skin temperature of the foot. Present study supports our earlier findings. But with or without DM a wound itself even without infection increases the temperature of the skin. The change in ABI, TP, and TBI measurements was smaller in patients with a wound than in patients without a wound, but with a greater change in temperature after revascularization. And when a wound had healed the temperature decreased. This could be explained by microvascular dysfunction. In the microcirculation blood flow is composed of the skin nutritional capillaries and thermoregulatory arteriovenous (AV) shunts. Glabrous skin, which is non-hairy skin the soles of the feet and the palms of hands, get 25% of its skin blood flow from nutritional capillaries and 75% from AV shunts. Non-glabrous skin does not possess AV shunts, and blood flow is composed almost completely of nutritional capillaries. Endothelial dysfunction in small vessels is an early marker of vascular disease. Microvascular dysfunction is a systemic process, where symptoms of PAD are caused by a lack of blood flow in the nutritional capillaries of the microcirculation that does not meet the metabolic demand of the surrounding tissues. When blood flow turns normal again after revascularization, the need of AV shunting decreases.35-37 This point can be utilized in evaluating wound healing as set in the following examples.
There were interesting individuals in the revascularization group whose findings we want to point out. There were 11 patients whose follow-up continued after first month; however, that extra period does not include to the study. During that period, we could see the whole healing process of the wound. There were two patients with diabetes with neuropathy but no wounds and two patients without DM or wounds. On them, the temperature decreased and the side-to-side change become even, with other blood flow indicators remaining unchanged. This seems to be a healthy reaction. Deep nutritive blood flow turns to normal after revascularization and decreases shunting through microvascular AV fistulas. So autologously the skin temperature appears to decrease as well. Similarly, in three patients, the wound healed during longer follow-up. At the same time, skin temperature continued to decrease and the side-to-side difference diminish consistently. The rise in skin temperature, as well as the side-to-side difference, is indicative of pathology, as stated previously. Thus, one concrete sign to be detected using IRT is if the temperature stays at high level or continues to increasing on inspected as normal feet. That might raise a suspicion of latent wound infection, osteomyelitis, or skin ulcer. That came up in four patients before there were any other signs that would have occurred according to standard examination practice. Also, patients in the follow-up group, who had previous treatment, skin temperature decreased and asymmetry decreased during the control period without any sign of worsening ischemia. For further investigation, longer follow-up period with larger amount of patients is required.
As reported in our previous studies, we have investigated the use of IRT as a diagnostic tool among PAD patients and patients with diabetes.21,22 Our outcome here in the present study strengthens these earlier findings and suggests that one of the most effective ways to use IRT is to use it as a follow-up tool among people with diabetes. It is also a valuable tool in the follow-up of PAD patients and patients with diabetes, who have had previous revascularization. On follow-up protocol, a bypass grafts malfunction can be easier detected by routine duplex ultrasound combined with ABI or TP/TBI measurements, and result of endovascular outcome is more difficult. Wound healing is often a slow process, despite sufficient local treatment. Adequate blood circulation assessment may also be difficult and require additional imaging. In that group of patients, IRT provides valuable information by means of systematic skin temperature follow-up and temperature variation interpretation.
Conclusion
IRT is interesting novel tool for screening skin temperature changes after lower limb revascularization. It has several possible advantages of being simple, noninvasive, and prompt. However, further studies are needed to clarify its position.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.