
Abstract
Background:
Irremovable total contact casts (TCCs) are the gold standard to offload diabetic foot ulcers (DFUs) and to immobilize feet with active Charcot neuro-osteoarthropathy (CN). They do not allow checks of the foot and are contraindicated in people with peripheral arterial disease (PAD). Frequently, removable TCCs and other removable devices are used because they allow wound care, modifications of the inner surface of the cast, and checks of the foot. The authors propose TCCs with ventral windows (VW-TCCs) whenever patients with high-risk conditions show poor adherence to wearing a removable cast all the time and access to the foot is necessary.
Methods:
This retrospective study compares treatments with bivalved, removable TCCs applied prior to the introduction of the novel design (from 1 January 2016 to 1 July 2017, “c”) to treatments in the following period (t) with both bivalved removable TCCs and VW-TCCs in use.
Results:
Forty-five treatments after introduction (17 with the VW-TCC) showed a 52.8% lower median time to reach remission of the DFS than 41 controls (128/267 days, log-rank test P = .013). Reasons given for not using the novel design were: sufficient offloading with a removable TCC (16), patient preference (six), anatomical conditions (two), casts applied as a service for other facilities (three), and calf ulcers (one). Adverse effects from both designs were uncommon and not severe.
Conclusions:
VW-TCCs combine advantages of both removable and irremovable TCCs. Complications do not limit the use, even in patients with PAD.
Introduction
Diabetic foot syndrome (DFS) is a lifelong complication of diabetes mellitus with alternating active and inactive phases. Active phases include diabetic foot ulcers (DFUs, 98%) and Charcot neuro-osteoarthropathy (CN; 2%). DFS is important because it is frequent (lifetime risk about 15% in people with diabetes),1-4 may lead to death,5-8 and to amputations.9-13 It compromises mobility and therefore affects independence and quality of life. 14 Active phases often take several months or years until stable load-bearing is restored.15,16 The long period of illness in many cases adversely impacts important aspects of personal life such as employment.11,16
Loss of protective sensation (LOPS) is the core aspect of this syndrome and offloading the most important causal treatment. A nonremovable total contact cast (TCC) has been considered to be the gold standard since the 1970s. 17 During that period, an average time of about six weeks needed to end the active phase was described.18,19 Initially it was made from plaster of paris, and later from synthetic material. Fitted tightly to distribute as much pressure as possible to the lower leg, it prevented access to the foot. Wound treatment and regular checks for complications were impossible. Peripheral arterial disease (PAD) is thus often seen as a contraindication. 20 The synthetic material weighs less and allows the TCC to be cut into two valves. In this way, the TCC can be opened, the plantar, inner surface can be modified, the foot can be cared for, and ulcers can be treated. The TCC is then closed, usually with straps. Having the possibility to open the TCC makes everyday life much easier. However, patients under study conditions take only an average of 28% of the steps in a TCC if it is removable. For the remaining portion, they walk with less effective devices or no protection at all. 21 This is associated with poorer outcomes. 22 “Off the shelf” walkers are also available. However, these boot-like offloading devices are usable only with normal shaped legs. Results similar to those obtained using a TCC have been reported, 23 especially when cable ties or other closures are used to prevent removal. However, wound care personnel must be able to remove the offloading device. Rendering these walkers irremovable is therefore not regularly put into practice. 24
Windows in irremovable TCCs have been studied since the era of plaster of Paris25-27 but have not found generally acceptance. Ulcers could be treated through a window that was then closed with a lid. Difficulties arose with the stable fastening of the lid. Pressure from the tilted lid or from the edge of the window often led to new ulcers.
We developed a bivalved TCC with the front shell divided into an upper and a lower half. The upper half is at least ten cm large and is sealed again leaving a ventral window (TCC with ventral window [VW-TCC]) in the lower part. The technique to apply the TCC is described in detail elsewhere. 28 The cast material in contact with the tibia is carefully padded. The foot can be partially pulled out of the TCC and treated (Figure 1). Since its introduction in July 2017 in the Cologne network for Diabetic Feet, selected patients have been treated with the VW-TCC. The aim of this study is to evaluate the feasibility and the possible effects on treatment results of the VW-TCC and to specify indications and contraindications.
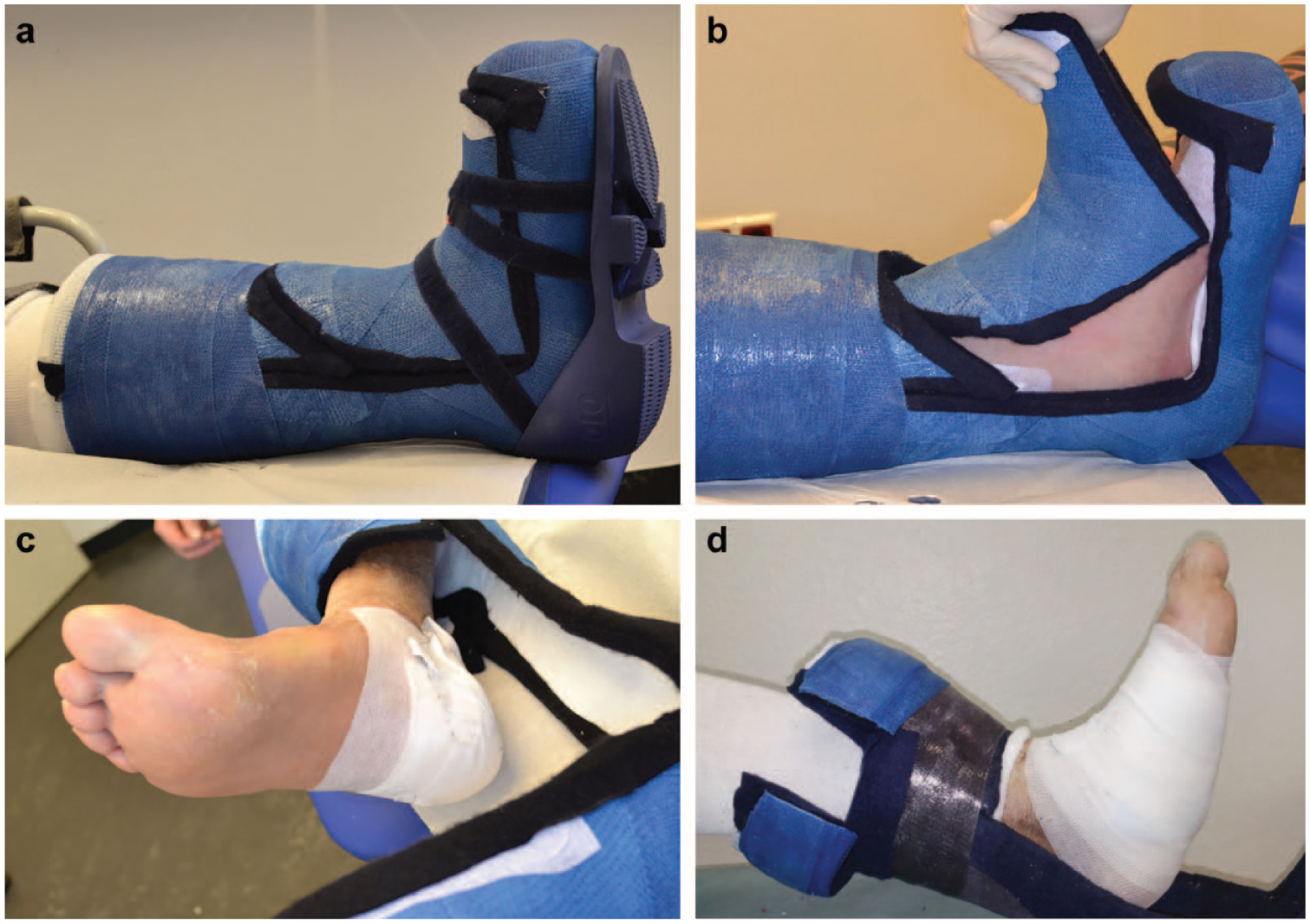
Ventral windowed total contact cast (VW-TCC): (a) closed with Velcro straps and sole applied; (b) opening and closing of the window; (c) optimized for heel ulcer; (d) optimized by additional lid at the calf.
Methods
This study is a retrospective cohort study evaluating outcomes of patients with a TCC applied in the 15 months prior to the introduction of the VW-TCC compared to the treatments with TCCs in the succeeding nine months. The casts were applied at the Outpatient Centre for Diabetology, Endoscopy and Wound Healing, a large outpatient foot clinic in the north of Cologne where the VW-TCC had been developed. After introduction of the VW-TCC, only patients showing a high risk stage of the disease (CN, recent surgical procedures in weight-bearing areas, plantar heel ulcers, other plantar ulcers with PAD or reaching deep tissues or not successfully offloaded using other devices) and poor adherence to wearing a removable cast all the time were treated with the novel design.
Patient records with reports between January 1, 2016 and March 31, 2018 containing the word “TCC” were selected. Data on risk factors and outcomes have been collected as part of the German DFS register. 29 The time needed from the start of treatment with a TCC to recover unharmed weight bearing was expressed as “time to remission” expressing the time needed to induce remission of the active phase of the disease. This meant the ability to walk with protective footwear a similar number of steps as was usual before the active period of the disease. It was assessed by the treating physician as sufficient thickness of the skin and controlled after two to four weeks. Further outcome measures were: amputations, death, hospital stays, and complications. Outcome measures were captured until October 15, 2018. Treatment episodes were divided into episodes with a TCC applied before July 1, 2017 (c) and episodes thereafter (t). The latter have been distinct in removable (r) and VW-TCCs (n). A distinction was made between the indications “CN,” “heel ulcer,” “securing a result of surgery” such as a local flap, and “ulcer at a location other than the heel.”
The data were collected in MS Access 2016 (Microsoft Corporation, Redmond, USA) and statistically evaluated using R in the Version 3.5.1 (July 2, 2018) and RStudio Version 1.1.456 (RStudio, Inc., Boston, USA). The t test was used for continuous variables, the χ² test for discontinuous variables, and the log-rank test to compare the time to remission.
Results
Data were found on 132 patients with 138 episodes of foot disease. Fifty-two were excluded because of: a TCC applied before January 1, 2016 (29), no TCC applied (seven), a TCC replacing a prosthesis permanently (seven), lost to follow up (four), irremovable TCCs before July 1, 2017 (three), suspected CN not confirmed, (one) and a CN but no diabetes (one). The final data set consisted of 86 treatment episodes in 85 patients (c: 41, t: 45). General data (Table 1) and risk factors (Table 2) showed no statistically significant differences between both periods. In the control group, CN was significantly more often the indication (Tab1e 3). Within the period with VW-TCCs, the group with removable casts showed some significant difference to the group with VW-TCCs as part of the selection process.
General Data.
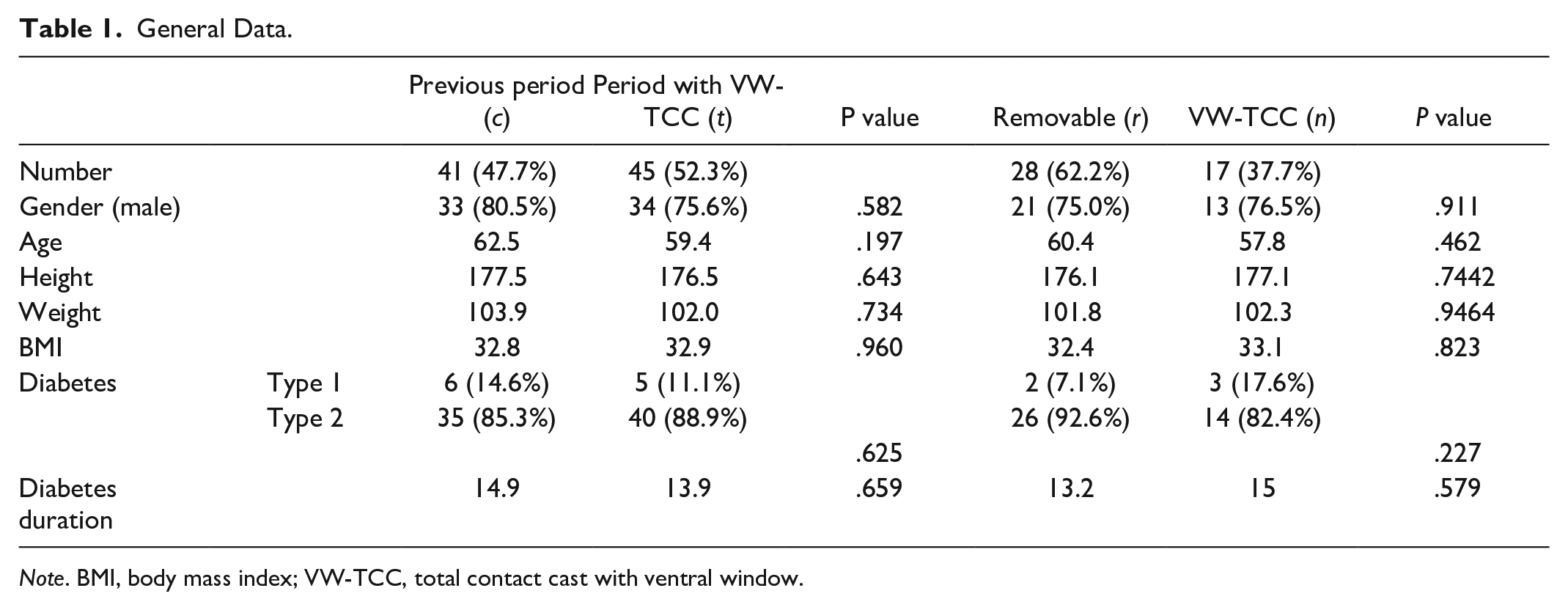
Note. BMI, body mass index; VW-TCC, total contact cast with ventral window.
Risk Factors for Negative Outcome.
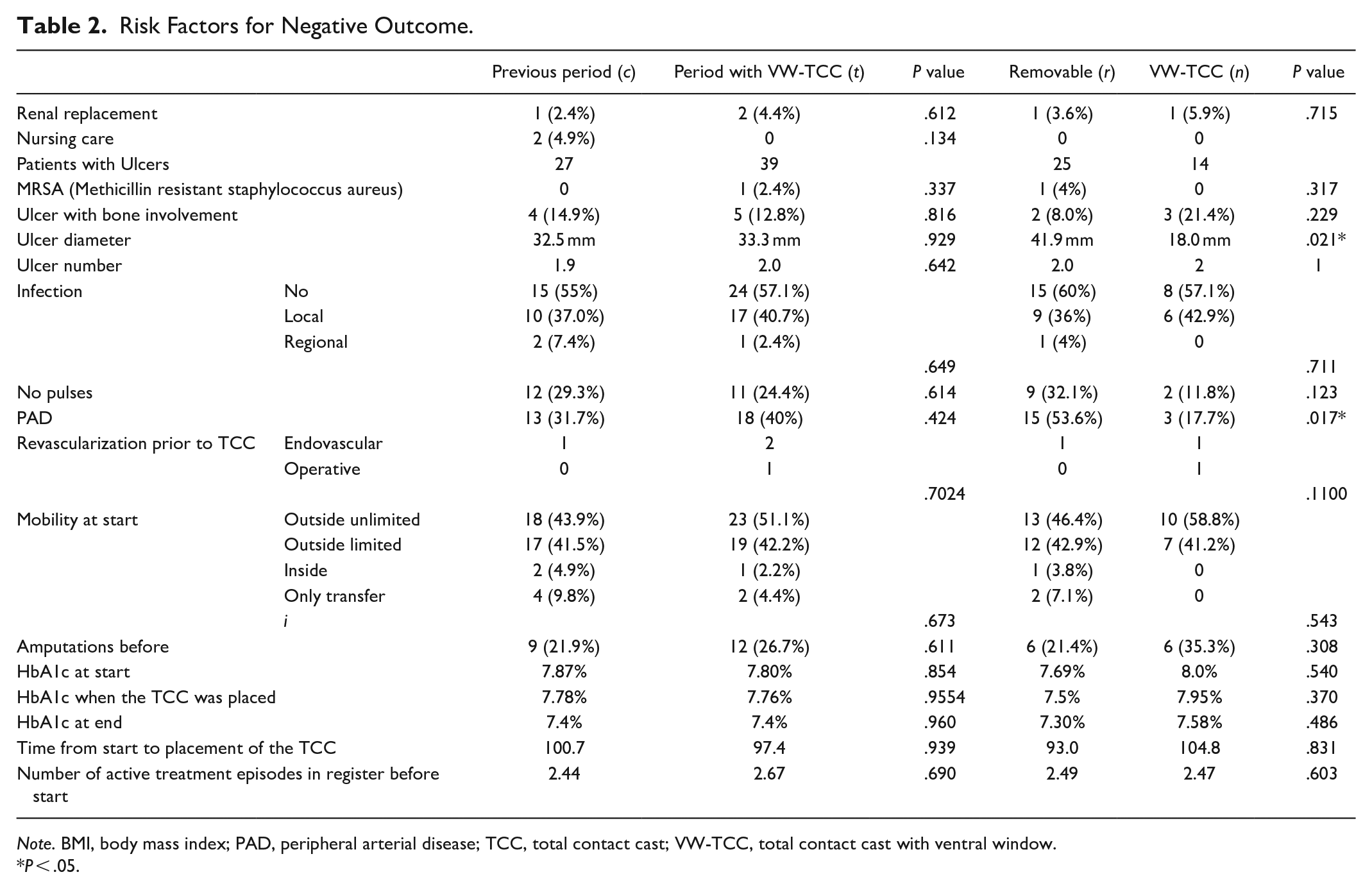
Note. BMI, body mass index; PAD, peripheral arterial disease; TCC, total contact cast; VW-TCC, total contact cast with ventral window.
P < .05.
The time between start of treatment with a TCC and stable wound closure (time to remission) was significantly shorter in the period after introduction of the VW-TCC. This is expressed as episodes in remission within 90 days (c: 12.2%/t: 35.6%, P = .011) or as Kaplan-Meyer-curves (log-rank test P = .013; Figure 2). The average is biased due to the different observation time and is mentioned only for completeness. The median duration was reduced from 267 to 126 days (-141 days or 52.8%; Table 4). With all indications, remissions occurred earlier after introduction of the VW-TCC.
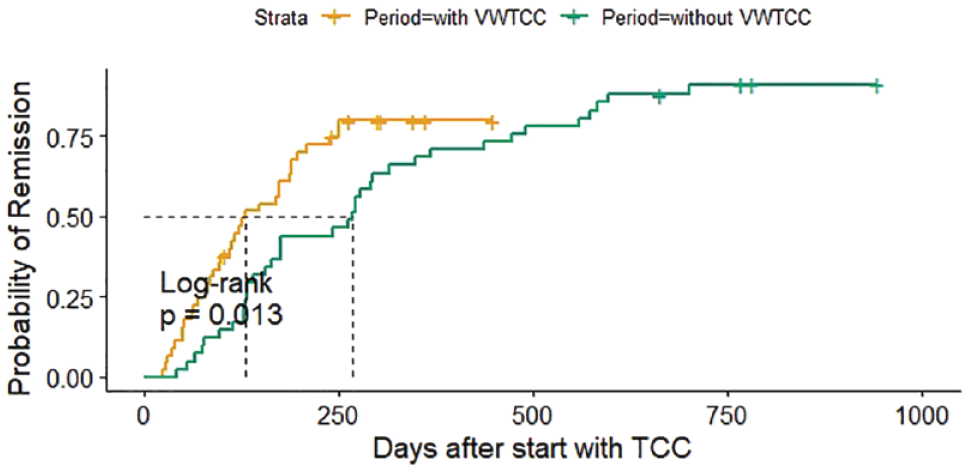
Time to remission from the begin of the use of the TCC. The green line denotes the treatments in the control period, the yellow line denotes the treatments after the introduction of the VW-TCC, using both types of TCC. A cross is used to mark censored cases due to the end of the observation period. TCC, total contact cast; VW-TCC, total contact cast with ventral window.
CN indicated a treatment in a TCC in a significantly higher proportion in the period before the introduction of the VW-TCC (Table 3). We additionally stratified for indications. For all indications, the treatment was shorter during the period in which the VW-TCC was used than in the period before (Table 5).
Indications for the Use of a TCC. The Intention to Protect the Vulnerable Result of Recent Surgical Intervention Was Expressed as “Secure Result of Surgery.”
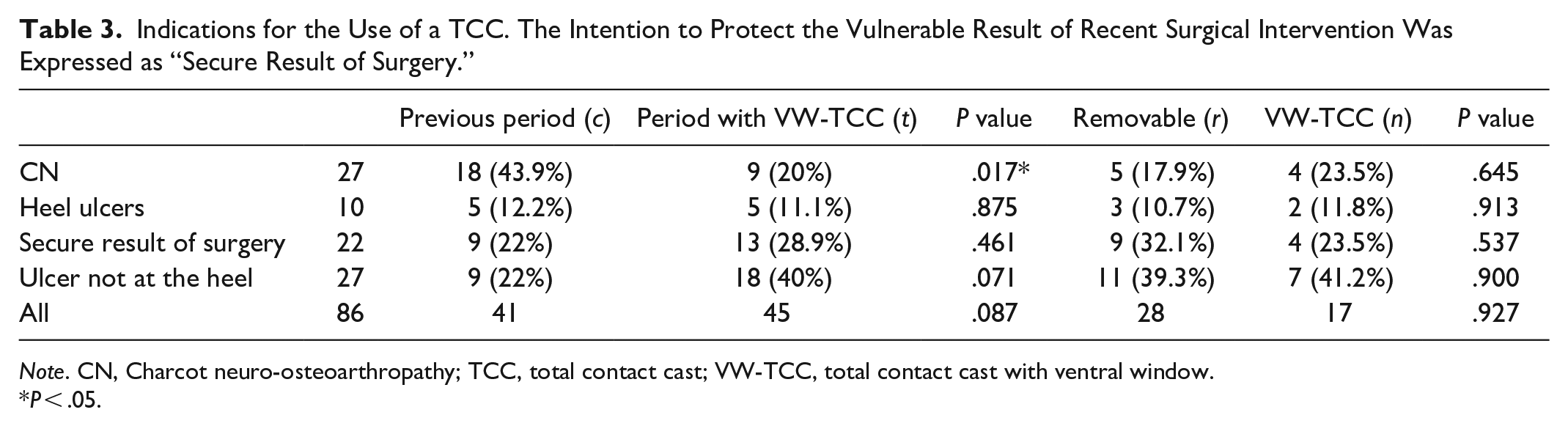
Note. CN, Charcot neuro-osteoarthropathy; TCC, total contact cast; VW-TCC, total contact cast with ventral window.
P < .05.
Time to Remission.
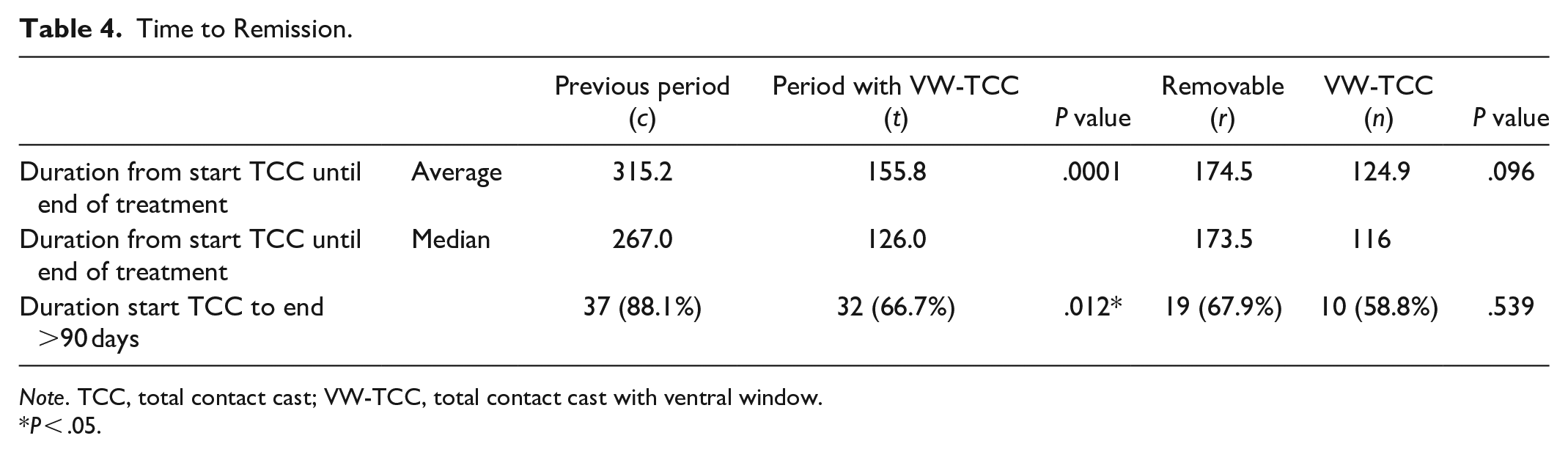
Note. TCC, total contact cast; VW-TCC, total contact cast with ventral window.
P < .05.
The Advantage Was Confirmed When Stratifying for Indication. The Period With Use of the VW-TCC Presents a Smaller Proportion of Treatments Longer Than 90 Days in Every Group of Indications.
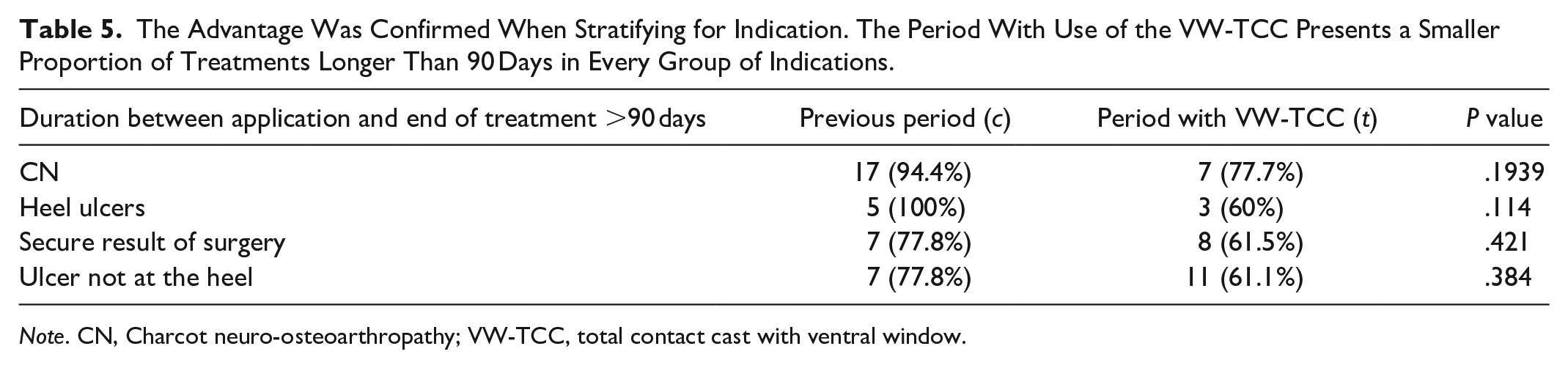
Note. CN, Charcot neuro-osteoarthropathy; VW-TCC, total contact cast with ventral window.
At the end of the follow-up, the treatment episode of 14 patients had not been completed (c: 4, r: 8, n: 2). Results—usually determined at the end of the treatment episode, such as amputations, hospital stay, and death—were calculated for the 72 finished treatment episodes. There was no significant difference in treatments requiring hospitals stays due to DFS (c: 26.9%/t: 31.1%, P = .6623), death (c: 4.9%/t: 2.2%, P = .2542), and amputation (c: 7.3%/t: 0.0%, P = .0647). The number of deaths and amputations were low and no definitive conclusion might be drawn from this evaluation (Table 6).
Death, Inpatient Treatment, and Amputation With the TCC.
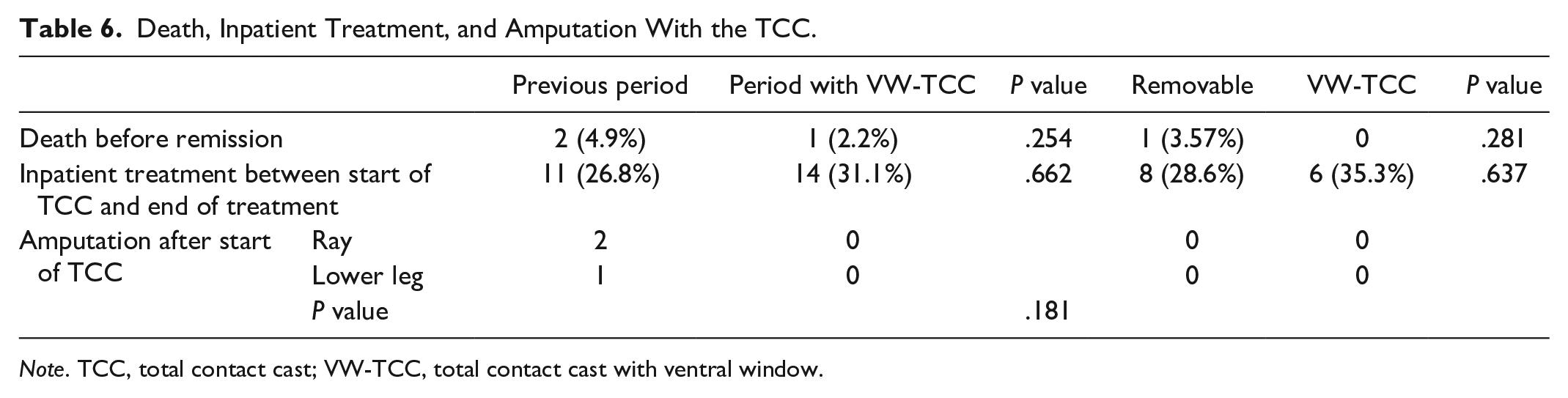
Note. TCC, total contact cast; VW-TCC, total contact cast with ventral window.
The following considerations were the reasons for the 28 cases when a removable variant was chosen after June 31, 2017 despite the introduction of VW-TCCs:
- Rejection of the VW-TCC by the patient (six).
- Treatment as service for other facilities unable to manage a nonremovable TCC (three).
- Anatomical conditions, so that the VW-TCC was not possible: (a) atrophy of the calf, so that pulling the lower leg partially out of the TCC does not allow movements at the level of the ankle; (b) after removal of the tuber calcanei or in people with very large calves, the foot can be pulled completely out of the VW-TCC (two).
- Ulcers at the calf (one).
- Necessity to apply compression bandages (0).
- Patients who were thought to take no steps without the TCC, even if removable, received a removable TCC (16).
As technical variants, TCCs had the incision at variably dorsal levels. They could feature flaps, for example, in the calf area or a raised heel (see also Figure 1).
In two cases, both with VW-TCCs, a revascularization was performed after the TCC had been applied because of insufficient progress in wound closure due to PAD. The TCC was continuously used also after the interventions.
Negative side effects of the VW-TCC were blisters in three patients, superficial skin defects on the tibial crest (three), and an injury of the external malleolus due to an unstable ankle joint in the context of a CN. One patient opened the VW-TCC with a handsaw without injuring himself. With a removable TCC, ten patients had injuries, three at the tibia, four on the forefoot, and two on the lateral side of the foot. In one case, superficial injury occurred during cutting of the cast. In none of these cases did these events lead to an inpatient stay, an amputation, an extension of the time to remission, or permanent damage.
Discussion
The importance of nonremovable offloading devices in the cure of people with DFS is undisputed. Nevertheless, they are not universally used as they are frequently perceived to be impractical when access to the foot is needed for dressing changes, ulcer treatment, or checks. In addition, patients often prefer to be able to decide themselves in any situation whether to wear the device or take it off. This attitude is subject to cultural and individual fluctuations.
This publication presents for the first time, to our knowledge, a construction that allows to remove a TCC only partially, so that practicability and medical requirements can be met. Patients give informed consent and agree to wear the device, but they no longer decide to wear it or not based on circumstances of everyday life. The introduction of this VW-TCC and its use in people who, according to medical assessment, combine a high risk of unfavorable outcome and an exposure to risky compromises, leads to a significant reduction in the time required to achieve remission of an active phase of the disease. This is consistent in various statistic approaches with a median time reduced from 267 to 126 days (141 days or 52.8%).
A limitation of this study is the selection of patients using the novel design by the treating physician. To overcome this possible bias, we compared the entire period when the VW-TCC was in use, whatever type of TCC has been chosen, with a historic control group. This mix in the treatment period might have levelled out some of the beneficial effect of the unremovable cast. To be sure that patients in both periods are comparable, we looked for all possible confounders. Only the indication showed a significant difference. Stratifying for the indication, the benefit was similar in each subgroup, but the numbers of patients were too low to show statistically significant results in any subgroup.
Current guidelines often list PAD among the contraindications of a TCC. The designs used in this evaluation permit checks. PAD is in important risk factor for adverse outcome and was considered rather an indication than a contraindication for a TCC. Usual care included revascularization of critical limb ischemia where indicated. In seven cases, revascularization was performed prior and in two cases after the TCC had been applied. Revascularization in these two cases was needed because of insufficient progress in wound closure, not because of complications in relation to the TCC. Both were VW-TCCs. One intervention was endoluminal and one a bypass. The VW-TCC was continued after the intervention. All revascularizations were considered as part of the assessment of risk due to PAD. With the applied technique, no event occurred that would support the traditional notion of PAD as a contraindication for TCCs. This is in line with a recently published review. 30
The injuries caused by the TCC during or after the construction were superficial and had no influence on the further course.
The introduction of the VW-TCC leads to an extension of the range of options for offloading, which may lead to a significant shortening of treatment times. There are few contraindications to the VW-TCC. The most important is the refusal by patients who, depending on the situation, want to decide when to wear the TCC and when not.
Conclusion
The use of a VW-TCC is possible even in patients with PAD.
The use of a VW-TCC in high-risk conditions considerably shortens the duration of the treatment compared to removable casts.
Adaption of the inner surface of the cast might allow optimized load distribution.
Contraindications for the application of a VW-TCC are in the order of frequency: a. Rejection by the patient. b. Anatomical conditions so that the VW-TCC is not possible such as an atrophy of the calf. c. Ulcers on the calf and in the transition area to the Achilles tendon. d. Necessity of applying a compression bandage.
Footnotes
Abbreviations
DFS, diabetic foot syndrome; DFU, diabetic foot ulcers; CN, Charcot neuroosteoarthropathy; TCC, total contact cast; VW-TCC, ventral windowed total contact cast; PAD, peripheral arterial disease.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding Source: This work was investor-initiated without sponsoring.