
Abstract
Background:
The purpose of this study was to determine the accuracy of wound area measurement at a curved surface using a digital planimetry (DP) with the newly proposed adaptive calibration.
Methods:
Forty wound shapes were printed and placed at the side surfaces of cylinders with diameters of 9.4 and 6.2 cm. Area measurements were carried out using a commercial device SilhouetteMobile (Aranz, New Zealand) and the planimetric app Planimator. Planimetric area measurements were carried out using 2 one-dimensional calibration markers placed above and below the wound shape. The method of adaptive calibration for DP was described. Reference area values of wound shapes were obtained by pixel counting on digital scans made with an optical scanner. Relative errors (REs) and relative differences (RDs) for area measurements were analyzed.
Results:
The median of REs for the DP with adaptive calibration (DPwAC) was equal to 0.60% and was significantly smaller than the median for the SilhouetteMobile device (SMD) (2.65%), and significantly smaller than the median for the DP (2.23%). The SD of RDs for the DPwAC of 0.87% was considerably lower than for the SMD (6.45%), and for the DP without adaptive calibration (2.51%). The mean of RDs for the DPwAC (0.082%) was not significantly different from zero, which means that the systematic error was not present for the DPwAC.
Conclusions:
The use of the adaptive calibration in DP to measure the areas at curved surface resulted in a significant increase of accuracy and precision, and removal of systematic error. The DPwAC revealed 4.4 times lower error and 7.4 times higher precision of area measurement at curved surfaces than the SMD.
Keywords
Introduction
Treatment of chronic wounds (ulcers) is a long-term process that requires specialized and multidisciplinary care. 1 In the process of assessing the treatment used, an index of percentage reduction in the wound’s area over a certain interval can be used. The Wound Healing Society recommends clinical procedures’ reevaluation if the ulcer surface area does not decrease by more than 40% in four weeks. 2 In 2016, three American societies involved in the treatment of people with diabetic foot ulcers (Society for Vascular Surgery, the American Podiatric Medical Association, and the Society for Vascular Medicine) recommended adjunctive wound therapy options such as negative pressure therapy, biological treatments, or hyperbaric oxygen therapy if the reduction of the ulcer area is lower than or equal to 50% after a minimum of four weeks of standard wound therapy. 3 The authors state that “wound area reduction of 10% to 15% per week or ≥50% area reduction in 4 weeks results in an increased likelihood of healing with decreased complications of infection and amputation,” and “by measuring wounds at 1- to 4-week intervals, the clinician documents healing progress and identifies the basis for treatment modification.” One can deduce that change in wound surface area is a very important parameter in wound assessment. Thus, measurements of wound area should be accurate as the therapeutic decision may depend on them.
There are various methods for measuring wound surface area.4-8 Digital planimetry (DP) is a method of measuring surface area, in which a digital camera is used as a device to take a digital photo of the measured region and the calibration marker placed next to this region in the same plane. Using the appropriate software, the surface area of the region is found and then converted into surface area units using a calibration coefficient calculated based on the calibration marker used. The measurement result is biased when the planes in which the measured area and the calibration marker are located do not overlap. It is common, especially at nonflat surfaces. One example of the use of DP at nonflat surfaces is measuring a wound surface area on the skin. In addition, a frequently raised problem that reduces the accuracy of measurement is the incorrect position of camera lens optical axis to the skin surface with the wound. The angle between the wound plane and the lens optical axis should be equal to 90°, otherwise, the measurement result is not accurate. The use of 2 one-dimensional (1D) calibration markers (rulers) located on both sides of the wound significantly reduces the measurement error and increases its precision. 9 Further improvements allow to make measurement corrections by using (a) a weighted calibration coefficient depending on the distance of the calibration line segments from the center of gravity of the wound outline and (b) a correction coefficient based on the calculated angle between the optical axis of the camera lens and the normal to the plane in which the wound is located. 10 All the above features are embedded in the Planimator app. It was developed in the Nalecz Institute of Biocybernetics and Biomedical Engineering, Polish Academy of Sciences (Warsaw, Poland) in 2015. It is not an open source product but it can be sent to users for noncommercial use. Its accuracy was tested and the median of REs for the area measurement of wound shapes located at flat surface was 0.32% for the Planimator app and 2.09% for the SilhouetteMobile device (SMD) (Aranz, New Zealand). 10 These errors may increase if the measured area is located at a curved surface.
The commercial device that has been verified regarding the accuracy of the surface area measurement is MolecuLight i:X device (MolecuLight, Toronto, Canada). 11 It uses DP to measure the wound area based on one or two dedicated two-dimensional (2D) calibration markers placed on opposite sides of the wound. When two calibration markers are used, the average error of area measurement with this device at flat and curved surfaces is 5.28%-5.46%. 12 Unfortunately, this error can increase to 15% when the measurement is performed with the use of only one marker. 13
The measurement of the wound surface can also be carried out using three-dimensional (3D) methods, which additionally give the opportunity to measure the volume of the wound, that is, tissue lost volume. Some of these techniques are based on stereophotography, and others use the projection of light patterns such as grids, lines, or dots at the surface on which the measured object is located, 14 while in others the structure from motion method is used. In the last method, it is necessary to place a calibration marker next to the wound to obtain a result in standard units of area or volume. Treuillet et al 15 described a two-camera system for assessment of skin wounds. The system requires a 2D or 3D marker to be present near the wound for its further area or volume calculations. Pavlovcic and Jezersek 16 described a 3D measurement system based on a digital single-lens reflex camera and a light pattern projector. The accuracy of their system in area measurement was 95%. Mirzaalian-Dastjerdi et al 17 showed a 3D wound measurement system based on the video taken from different angles showing a wound to be measured and a calibration ruler. They reported a mean relative error (RE) of their system of 4.22% ± 0.45% on phantom images. Jorgensen et al 18 presented a 3D wound assessment monitor camera consisting of three cameras and a mesh projector. Three photos from different angles are necessary to build a 3D image of the wound. The authors did not determine the accuracy of the 3D method they used but they found a high correlation of 3D method of area measurements with the results of 2D method, which was DP. The eKare Inc (Fairfax, USA) offers a 3D wound assessment device called inSight, which is a combination of iPad tablet (Apple, USA), structure sensor (Occipital, USA), and a software. 19 The device is able to measure wound area with an error up to 5%. 20
The purpose of this study is to determine the accuracy of surface area measurement at curved surfaces using DP with and without a newly developed adaptive calibration. The accuracy of these two approaches will be compared to the accuracy of a commercial device. The Planimator app will be used in DP measurements and the SMD will serve as a commercial device.
Methods
Digital Planimetry
For planimetric measurements, the smartphone app Planimator 10 was used in this study. During measurements at a curved surface, self-adhesive 1D calibration markers were placed below and above the wound shape parallel to each other and perpendicular to the longitudinal axis of the cylinder, whose lateral surface was a curved surface (Figure 1).
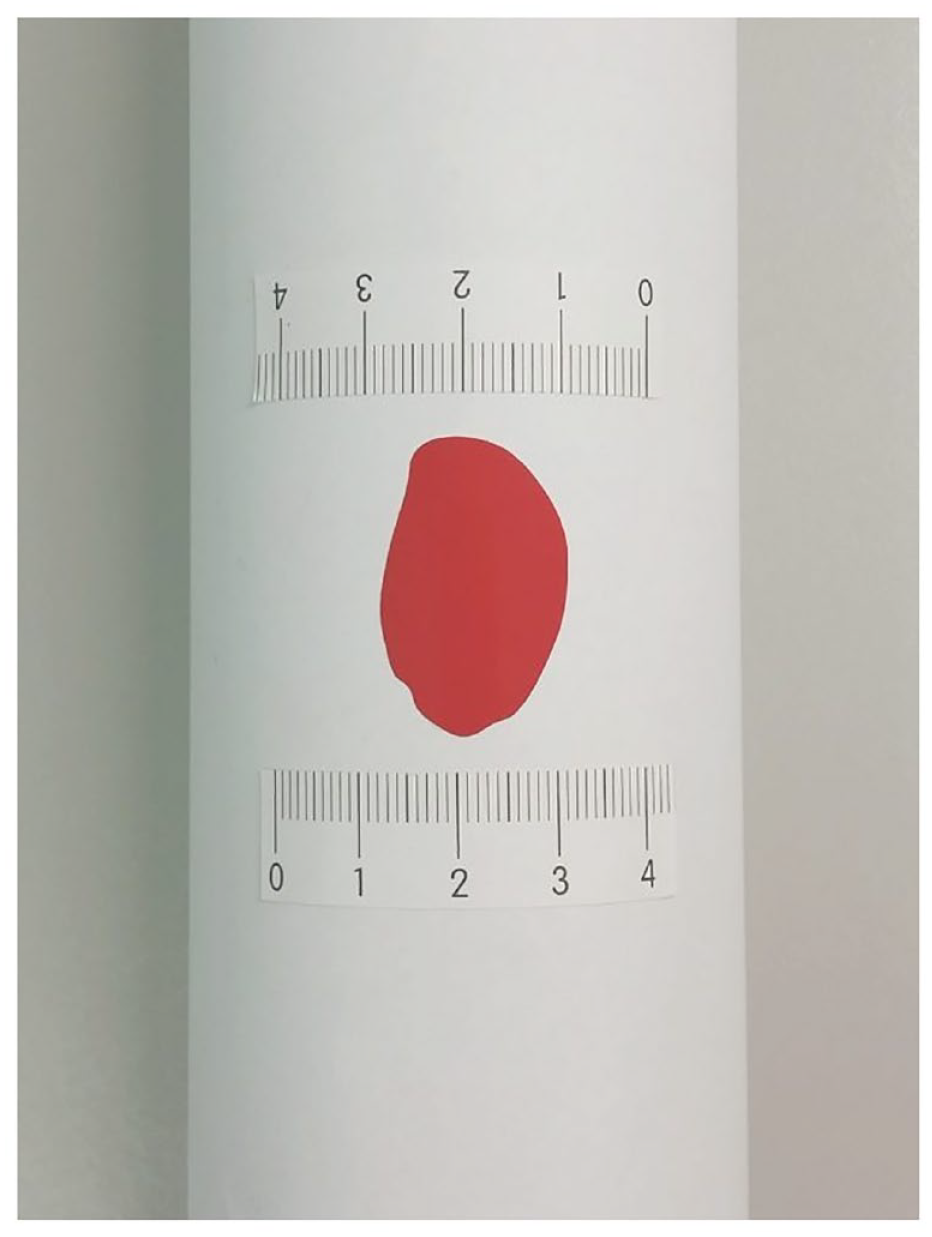
Photo showing the mutual position of a wound shape and calibration markers during surface area measurement of this shape placed at a curved surface, which was the lateral surface of a cylinder.
Based on preliminary measurements of the surface areas of the wound shapes placed at curved surfaces, it could be concluded that when the pictures were taken from too short distance, large distortions were present and it was difficult to draw calibration line segments at the calibration markers. The analysis of deviations of the measurement results from the reference values revealed that the result is influenced by the ratio of the calibration segment length and width of the measured wound shape. The impact of the length of the calibration line segment was manifested as follows: too long its length caused overestimation of the measurement result, and too short caused underestimation. In Figure 1 it can be seen that the distances between adjacent ticks at the calibration marker are not uniform over the entire length of this marker placed at the curved surface. Drawing a calibration line segment at such a marker with a length of, for example, 2 cm (for instance between ticks “1” and “3”) in order to obtain a calibration coefficient (number of pixels per 1 cm), and then drawing a line segment twice as long (for instance, between ticks “0” and “4”) will cause, with very high probability, that the calibration coefficient will change. Such a change will obviously affect the result of the area measurement because to obtain the measurement result in units of area (eg, “cm²”) the surface area expressed in pixels must be divided by the calibration coefficient raised to the second power. 10
Model Study: Adaptive Calibration
What length should the calibration line segment be so that the measurement result is as close to the correct value as possible? In order to answer this question, the region whose area is to be found will be divided into bars of very small width. Now, to accurately measure the actual height of such a bar with a width Δx (eg, yi bar in Figure 2), it is necessary to draw the calibration line segment with the same length as the yi bar and calculate the calibration coefficient ki, and then the actual length of this bar will be equal to its height expressed in pixels divided by ki. To measure another bar with a different height, the corresponding calibration coefficient should be found in the same way. The average calibration coefficient in the form of an arithmetic mean should be calculated for the whole measured region from the coefficients calculated for each of the bars. This procedure would be time-consuming; therefore, it will be modified so that the average height of the bars is found first, and then the average calibration coefficient is determined for it.
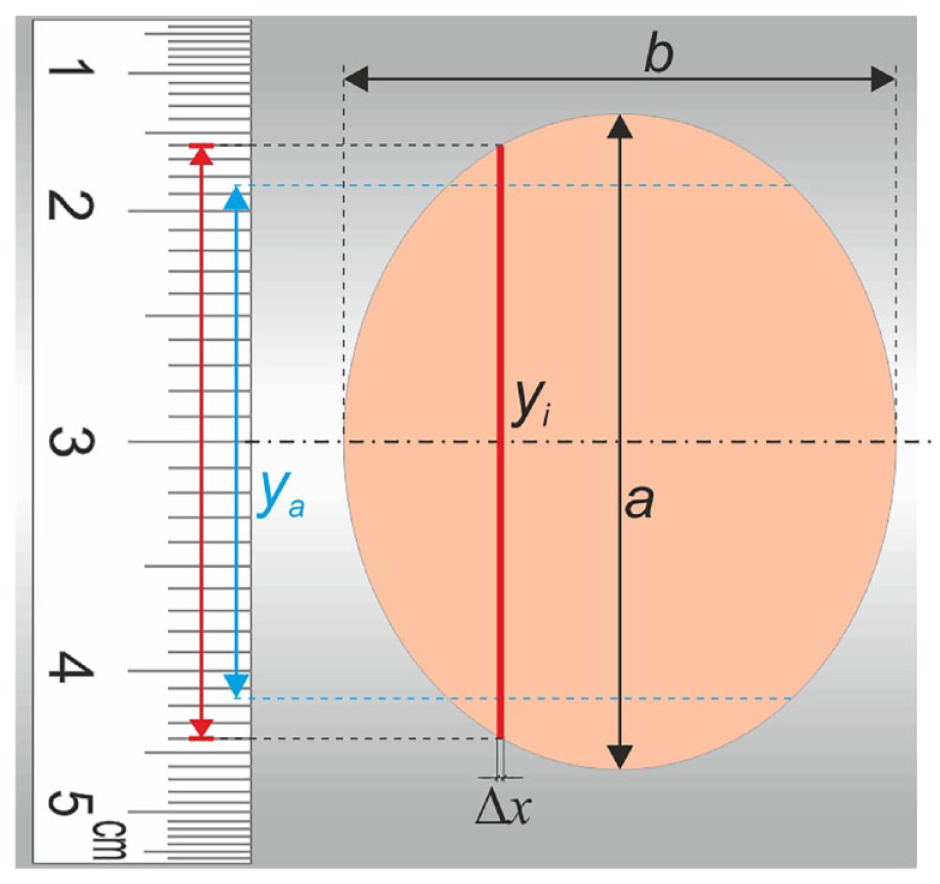
An elliptical shape placed at a curved surface and a one-dimensional calibration marker placed next to it. The ellipse can be divided into n bars y1 . . . yn with a width of Δx, whose sum of areas will be equal to the area of the ellipse. The height of the ellipse is equal to a, while b is its width. The curvature of the surface causes that adjacent ticks at the calibration marker are not visible at constant distances from each other.
Figure 2 shows an ellipse and a calibration marker placed at a curved surface. The ellipse was chosen because the shape of most wounds is elliptical. If this ellipse is divided into n vertical bars (y1 . . . yn) with width Δx, then their average height ya can be calculated according to the following equation:

In the digital image, the smallest object has a size of 1 pixel, so the minimum width of bar yi can be equal to 1 pixel, and its height will also be expressed in pixels. In this image, n will be equal to the width of the ellipse b expressed in pixels, while the

The area A of the ellipse can be expressed as

After calculating ya based on the above equation, it may not be possible to draw a calibration line segment of such length at the calibration marker, because the calibration line segment must have its beginning and end at the middle of the tick. The operator performing the measurement should draw a calibration line segment with a length best suited to its calculated length. Then it is possible to calculate the calibration coefficient by dividing the length of the calibration line segment expressed in pixels by the distance between the ends of this line segment expressed in units of length (eg, centimeters). Calibration markers with rarely spaced ticks, for example, every 5 or 10 mm, cannot be recommended for adaptive calibration, because then the adjustment of the length of the calibration line segment will not be accurate.
Measurement Procedure
The entire procedure of measuring the surface area requires two calibration coefficients from each of the two calibration markers placed on both sides of the measured region. In the Planimator app, the calculation of the calibration coefficient is automatic after the operator indicates the beginning and end of the calibration line segment. Figure 3 shows the measured shape with width a and calibration markers on which calibration line segments y1 and y2 are drawn with lengths equal to approximately
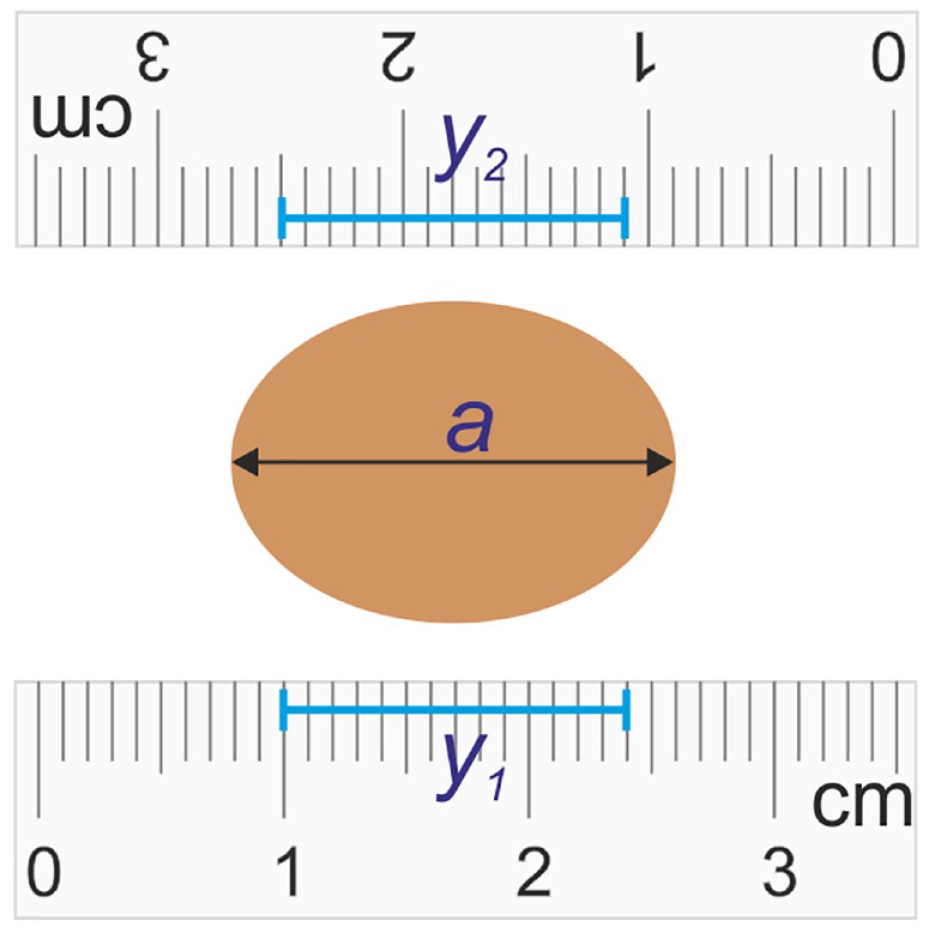
The principle of adaptive calibration in digital planimetry with the use of 2 one-dimensional calibration markers. For an elliptic wound of width a, the calibration line segments y1 and y2 should be drawn at calibration markers with lengths equal to πa/4 ≅ 0.79a.
Main Experiment
A set of 40 wound shapes21-23 were created in CorelDraw (Corel Corp., Ottawa, Canada) based on real wounds from patients with diabetic foot syndrome. Each wound shape had a gray color (50% black) and was printed on a white paper. Their actual (reference) areas were measured after scanning them with an optical scanner (600 dpi × 600 dpi) and counting the number of pixels in wound shape. The wound shape area expressed in cm² was obtained as the product of the number of pixels belonging to the measured wound shape and the area of a single pixel expressed in cm². The range of wound shapes areas was 0.14-31.72 cm². Then the surface areas of these wound shapes were measured using the SMD and the Planimator app installed at the Samsung Galaxy S5 smartphone and compared with reference values of the area. Each wound shape was attached to the lateral surface of a cylinder. Verified calibration markers were attached below and above the wound shape in that way that they were parallel to each other and perpendicular to the longitudinal axis of the cylinder (Figure 1). The markers’ verification was performed after scanning them with an optical scanner with a resolution of 1200 dpi and 24 measurements of the distance between ticks, which should be spaced by 5 cm, taking each time two other ticks. Markers revealed to be shorter by 0.093%, and the corrected value of 0.99907 was used in the Planimator settings.
The diameters of cylinders were 9.4 and 6.2 cm. The larger cylinder diameter may roughly correspond to the diameter of the lower part of the human lower limb, and the smaller diameter to the human upper limb. Other authors used similar cylinder diameters to simulate a curved surface, for example, 8.8 cm for the Silhouette device’ 24 or 9.0 cm in or the MolecuLight i:X device. 12 Gentler surface curvatures were used in Mirzaalian-Dastjerdi et al 17 with cylinder diameters of 17 and 39 cm.
The operator performing measurements using standard DP technique was drawing the calibration line segments according to the principle previously given, 10 that is, they should be approximately equal to the width of the measured region. The operator using the DP with adaptive calibration (DPwAC) technique was drawing the calibration line segments according to the rules of adaptive calibration and kept the distance of taking the photo large enough that the calibration markers were not strongly arcuate at the photo and positioned the smartphone camera so that the wound shape was in the center of the photo, and the arches of the calibration markers in the photo were approximately the same (Figure 1).
One of the wound shapes (#40 23 ) was so large that after placing it at the cylinder, it was not fully visible in one photo. Therefore, it was virtually divided into two parts, whose areas were separately measured, and their sum gave the area of this wound shape. The time needed to perform a single measurement with the Planimator app was from one to four minutes depending on the size of the wound shape.
REs and relative differences (RDs) were calculated from the measurement results and reference surface area values. RE was obtained by dividing the absolute difference of measurement result and the reference value by the reference value. Therefore, RE can achieve only non-negative values. RD is the result of dividing the difference of measurement result and the reference value by the reference value. The lower the SD of RDs, the higher the precision is (ie, repeatability) of the measurement method.
Statistical Analysis
The Kruskal–Wallis test and the median test were used for comparison of medians of REs. SDs of RDs were compared using F-test for variance comparison. Normality of data distribution was verified using Kolmogorov–Smirnov, Lilliefors, and Shapiro–Wilk tests. One-sample t-test was used for testing whether the mean differs from zero. Analyses were performed in Statistica software v. 10 (StatSoft, Inc., Tulsa, OK, USA). P-value lesser than .05 was considered statistically significant.
Results
Figure 4 presents the box plot of REs for the methods used in the study and P-values for comparisons of medians of these errors for the used methods on two diameters of the cylinders constituting curved surfaces. Significant differences between these medians were for the DPwAC and the DP (P < .0001) and for the DPwAC and the SMD (P < .0001). Insignificant differences (P = .25) were between the DP and the SMD.
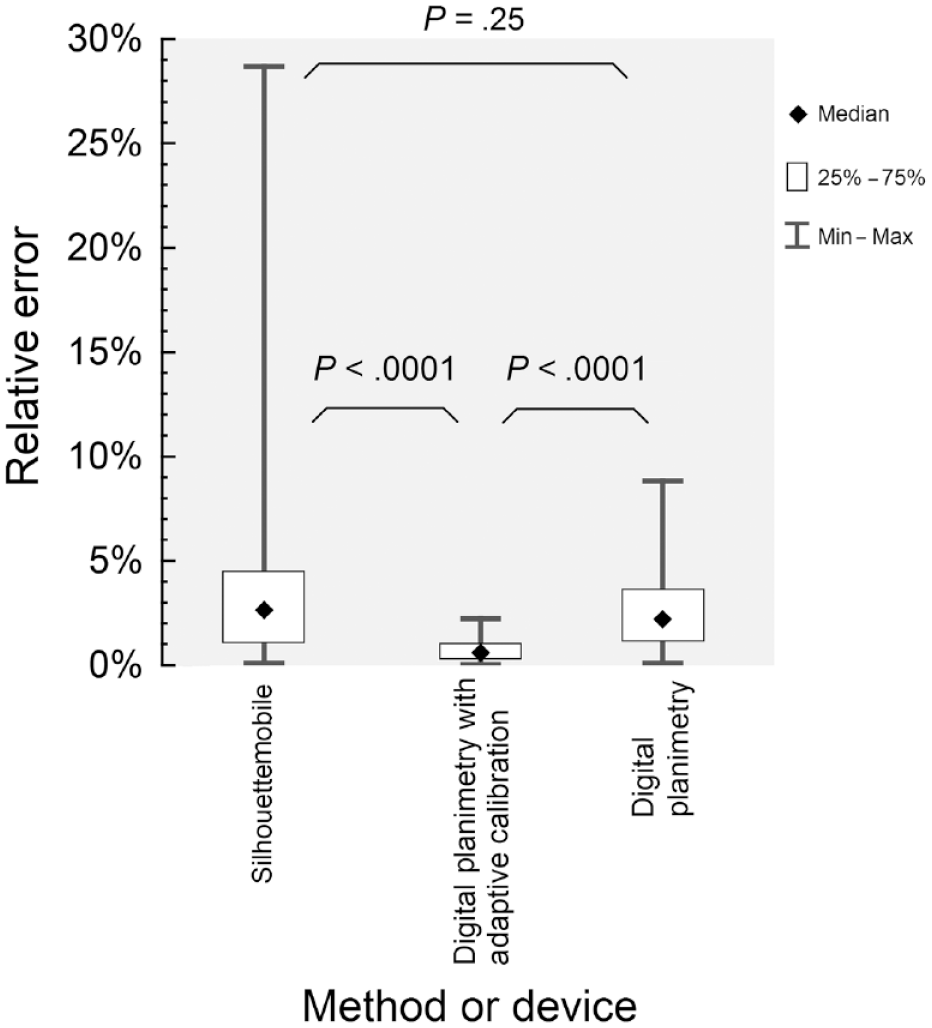
Comparison of relative errors for surface area measurements with the SilhouetteMobile device, the digital planimetry with adaptive calibration, and the digital planimetry. Wound shapes were printed on paper and placed prior to measurement at the lateral surface of a cylinder with a diameter of 9.4 or 6.2 cm (N = 80).
Table 1 contains medians and ranges of REs for the measurement methods used and the ratio of median of REs for a certain method and median of REs for the DPwAC. Since the lower is the median of REs, the more accurate is the measurement method, the DPwAC was the most accurate method in the current study. Less accurate methods with larger medians of REs were the SMD and the DP. Their medians of REs were at least four times larger than for the DPwAC.
The Medians and Ranges of REs for the SMD, the DP, and the DPwAC.
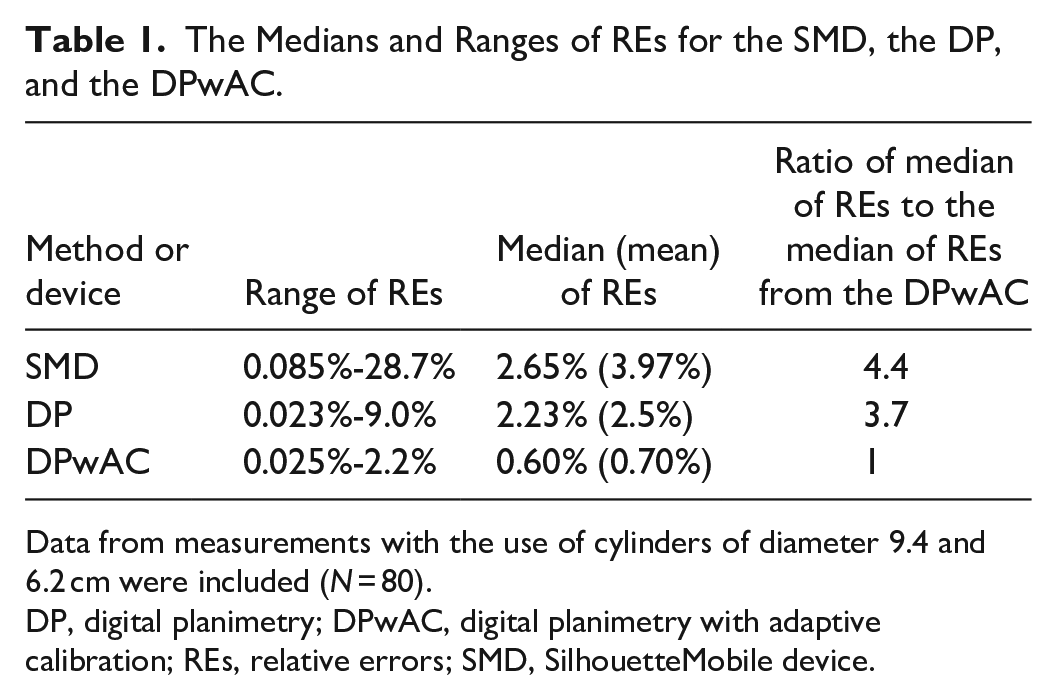
Data from measurements with the use of cylinders of diameter 9.4 and 6.2 cm were included (N = 80).
DP, digital planimetry; DPwAC, digital planimetry with adaptive calibration; REs, relative errors; SMD, SilhouetteMobile device.
The distributions of RDs were tested for normality (Figure 5). For the DPwAC and the DP there were no significant deviations from the normal distribution (P > .20), while significant deviations were found for the SMD with P < .01.
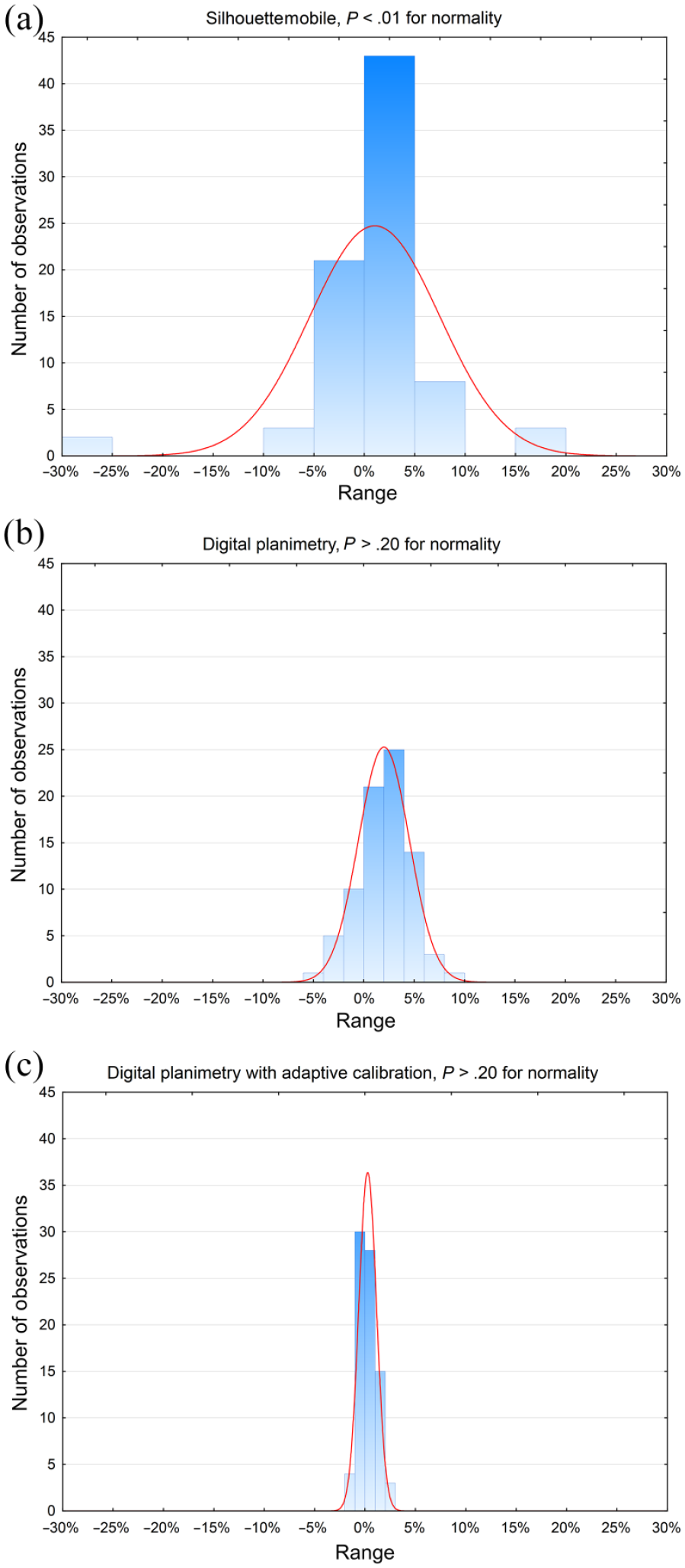
Distributions of RDs for the SMD (a), the digital planimetry (b), and the digital planimetry with adaptive calibration (c). Normality of distribution occurred for the last two measuring techniques (P > .20), while for the SMD the distribution of RDs significantly deviated from normality (P < .01) .
Table 2 shows the values of calculated mean, SD, and range for RDs. Next to the mean in column 2, the P value is given for a test assessing whether this mean differs from zero, which is equivalent to testing the significance of systematic error. The test was not performed for the SMD because the distribution of RDs was not normal and the t-test could not be used. The mean of RDs for the DP (1.82%) was significantly different from 0 (P < .0001), whereas the mean for the DPwAC (0.082%) was not significantly different from 0 (P = .40).
Means, SDs, and Ranges of RDs for the SMD, the DP, and the DPwAC.
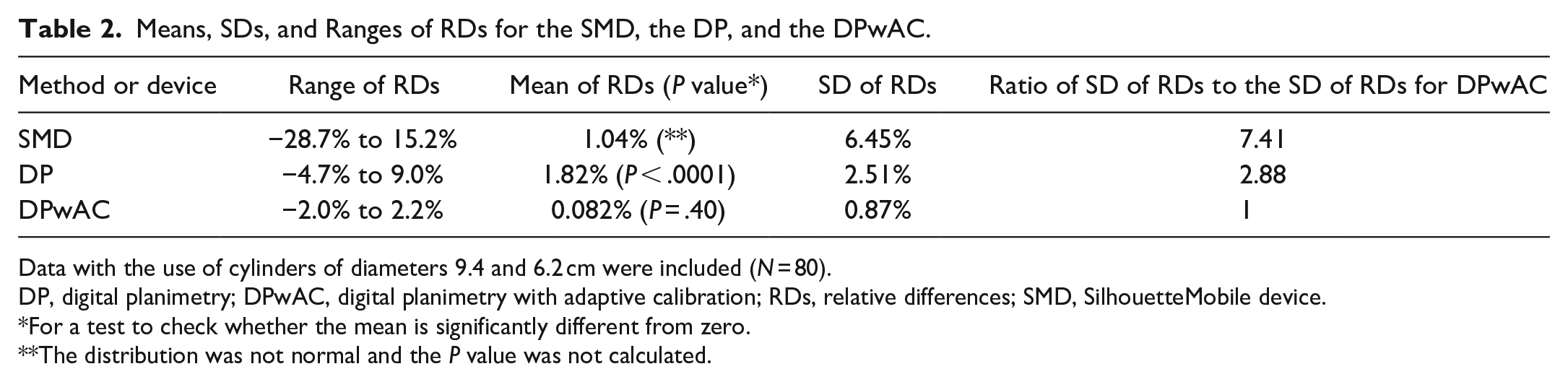
Data with the use of cylinders of diameters 9.4 and 6.2 cm were included (N = 80).
DP, digital planimetry; DPwAC, digital planimetry with adaptive calibration; RDs, relative differences; SMD, SilhouetteMobile device.
For a test to check whether the mean is significantly different from zero.
The distribution was not normal and the P value was not calculated.
The SDs for the used methods were also compared with each other. The SD for the SMD (6.45%) was significantly higher than for the DP (2.51%) and for the DPwAC (0.87%) with P <.0001 for both cases. The last comparison of SDs revealed that SD for the DP was significantly higher than for the DPwAC (P < .0001).
Table 3 shows REs of all methods used in the study for both cylinders of diameter 9.4 and 6.2 cm. The number of errors that were larger than 5% were 16 for the SMD, 7 for DP, and none for the DPwAC.
Relative Errors for the SMD, the DP, and the DPwAC.
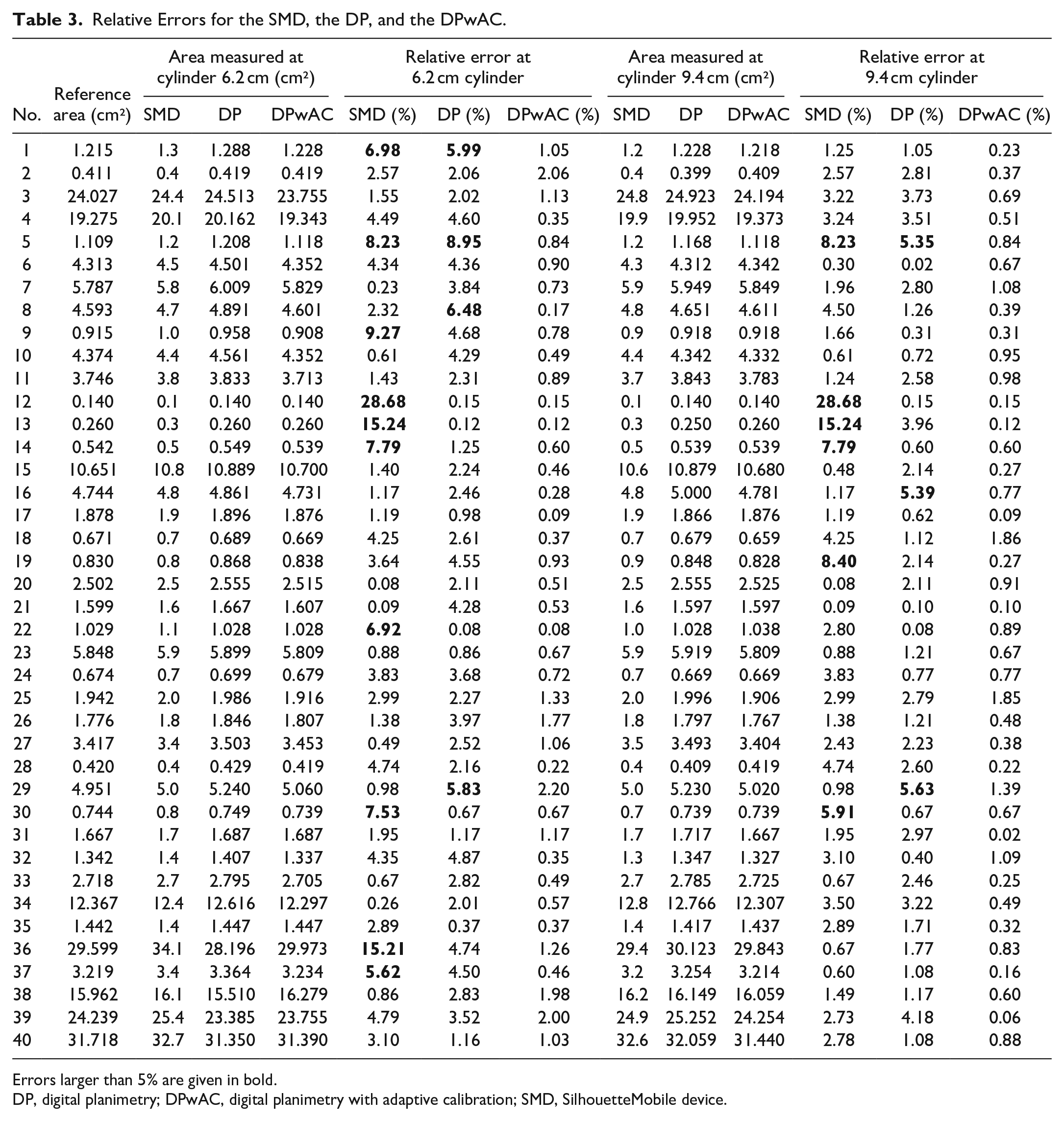
Errors larger than 5% are given in bold.
DP, digital planimetry; DPwAC, digital planimetry with adaptive calibration; SMD, SilhouetteMobile device.
Discussion
Three-dimensional methods of measuring the wound surface area due to the possibility of mapping the skin surface are intuitively treated as more suitable for measuring the wound surface area than 2D methods based on a 2D image. This may be due to the fact that very often the skin surface with the wound is not flat, while the photo of the wound, based on which the measurement is performed, is 2D and is only a certain projection of 3D surface onto a flat surface. The current study was intended to verify the accuracy of DP in wound area measurement at a curved surface. Several advantages of a 1D calibration marker (such as thin adhesive ruler) were exploited. Such a marker adheres well to the skin and reflects its curvature, and, more importantly, it enables adaptive calibration based on adjusting the length and location of the calibration line segment according to the width of the measured wound. This helps to increase the accuracy of surface area measurement at curved surfaces, which was confirmed by the current study results. The median of REs for the DPwAC of 0.60 (0.025%-2.2%) was 3.7 times lower than the median of REs for the DP without adaptive calibration and simultaneously 4.4 times lower than the median of REs for the commercial device (SilhouetteMobile). These results demonstrate the effectiveness of the presented rules of measurement using DP at curved surfaces.
The comparison of SDs for RDs revealed another advantage of the DPwAC, that is, higher repeatability. This SD of 0.87% for the DPwAC was 7.4 times lower than for the SMD, and about 2.9 times lower than for the DP without adaptive calibration. Therefore, presented in the present study, adaptive calibration revealed its impact on increasing the measurement precision.
The comparison of the accuracy of measurement methods obtained in this study with the results provided by other authors can only be approximate because there are differences in the methodology of experiments. For example, for the MolecuLight i:X device, the average error of about 5% is given for flat, flat slanted, curved, and curved slanted surfaces. 12 For the Silhouette device (Aranz Medical, New Zealand), the surfaces were flat, curved, concave, and convex. 24 Other authors had a small sample size based on which the error was estimated.16,17 In the studies presented in the Introduction section, the average error of area measurement was about 5% ± 1%, and it was larger than the mean error obtained in this study for the DPwAC of 0.70% (Table 1).
Mean of RDs, which is a measure of systematic error, should be zero for an unbiased measurement method. This was the case for the DPwAC since the mean of RDs equal to 0.082% was not significantly different from zero (Table 2). Significantly different from zero was the mean for the DP (1.82%). The mean for the SMD (1.04%) was not tested due to lack of data normality.
The proper calibration marker to be used in adaptive calibration must have ticks spaced relatively in short distances in relations to the size of the wound and to the curvature of the skin to assure good positioning and length of the calibration line segment. For wounds up to about 30 cm², the calibration marker should have these ticks every 1 mm, not, for example, every 5 mm.
It should also be mentioned that the camera lens can introduce image distortions, which can additionally increase measurement error. Whether the camera lens produces distortions can be easily determined after photographing a grid chart for the distortion tests. In the photo the lines of this grid should be straight and parallel to each other. Barrel or pincushion lens distortions 25 may be the sources of additional errors, and cameras with such lenses should be avoided in area measurements.
When testing the accuracy of DP without adaptive calibration at flat surfaces, the median of REs was 0.32% with range (0.0008%-1.6%), 10 and at curved surfaces it increased to 2.23%, while for the SMD it was 2.09%, range (0.09%-28.7%) for measurements at flat surfaces 10 and increased to 2.65% in this study at curved surfaces. A similar trend can be seen when looking at the measurement precision. The SD of RDs for the DP without adaptive calibration at flat surfaces (ie, method Planimator at Table 2 in Foltynski 10 ) was equal to 0.52%, and at curved surfaces it increased to 0.87% in the current study. For the SMD, SD of RDs was 5.83% at flat surfaces, and also increased to 6.45% at curved surfaces. The increase in measurement error and decrease in precision when changing surfaces from flat to curved is rather obvious as the curvature of the surface is an additional adverse factor in the surface area measurement.
Based on the current study, DP based on two 1D markers proved to be a method of area measurement at curved surfaces no less accurate than a commercial device. The adaptive calibration in DP, presented here, significantly increases the accuracy of area measurement at curved surfaces. It seemed quite natural to some developers of 3D techniques that a 2D technique cannot be accurate on curved surfaces but this study did not confirm this.
Some clinical experts may suggest that they do not need a very accurate method for wound area measurement. They may claim that the error of 5% is acceptable but they also assume that each measurement will have an error no higher than 5%. The number of errors larger than 5% (Table 3) was 16 for the SMD, 7 for the DP, and all errors for the DPwAC were lower than 5%. Therefore, only the DPwAC met the requirement. The conclusion is that it was necessary to increase the accuracy of the DP by the adaptive calibration, because without it, the DP, although had a mean error of 2.5%, would not meet the requirement.
Footnotes
Abbreviations
DP, digital planimetry; Res, Relative errors; RDs, relative Differences; DPwAC, digital planimetry with adaptive calibration; 2D, two dimensional; 3D, three dimensional; SD, standard deviation; SFM, structure from motion.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.