
Abstract

In advance of the upcoming academic year, parents of students of all ages are receiving severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) related updates. Generally, parents are offered two options: (1) send children back to school or (2) continue remote learning.
This is the decision facing one of our patients, a 42-year-old woman with type 1 diabetes mellitus (DM1), who has two healthy school-age children. She desired to have her children return to school but was concerned that they could be exposed to SARS-CoV-2 at school and transmit the infection to her.
Though the link between type 2 diabetes mellitus (DM2) and increased mortality from SARS-CoV-2 has been established, data on patients with DM1 remain sparse. 1 Preliminary data have shown no increase in hospitalization rate in patients with DM1, as well as lower mortality in patients with DM1 compared with patients with DM2 infected with SARS-CoV-2.2,3 Similarly, low reported SARS-CoV-2 case count in patients with DM1 has led to hypotheses that younger age, lower cardiovascular risk, and the autoimmunity associated with DM1 may be protective. 4
There are evidence-based guidelines favoring in-person schooling for children in general. 5 However, the benefits of in-person schooling must be balanced against the health risk to an adult with a chronic condition. In the absence of any current published guidance, we sought advice from a consortium of experienced leaders in diabetes care at leading institutions in the United States.
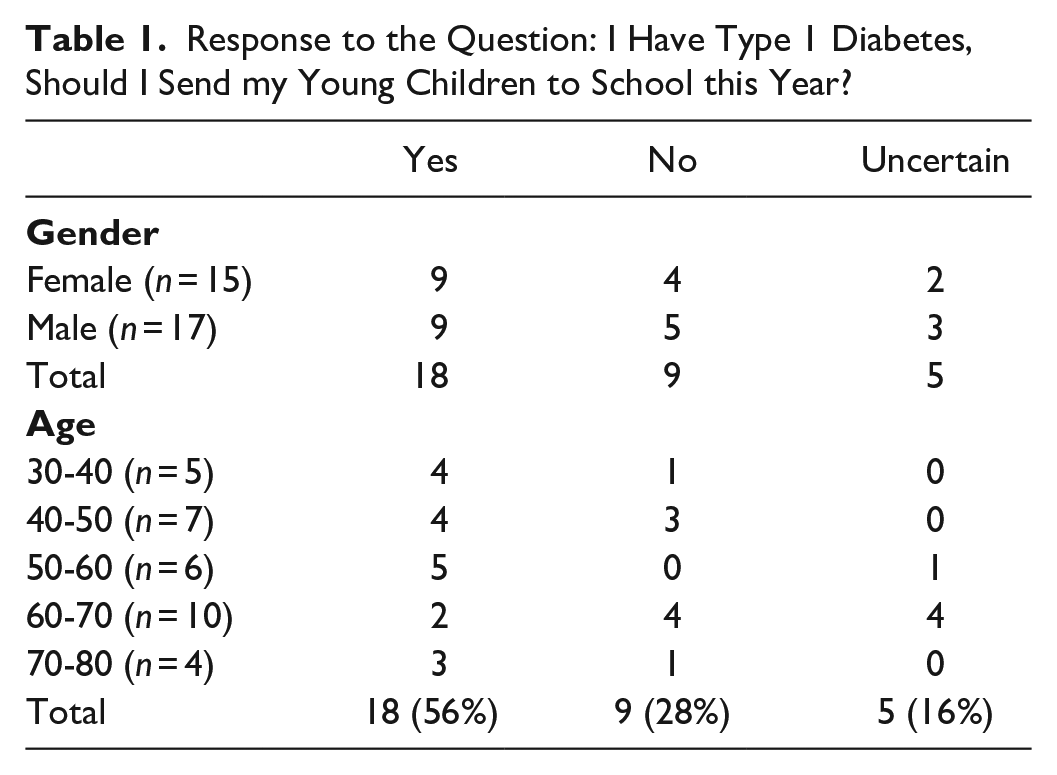
We received 32 responses from a variety of providers (28 physicians, 3 nurse practitioners/registered nurse, 1 clinical pharmacist) (Table 1). When stratified by age, 72% of providers under age 60 recommended sending the children to school compared with 36% of providers over age 60. Three respondents have DM1 (two of whom have school-age children), and all three recommended sending the children to school.
Response to the Question: I Have Type 1 Diabetes, Should I Send my Young Children to School this Year?
When reviewing comments in favor of sending the children to school, prominent themes included beliefs that (1) the risk increase for DM1 is not significant, especially if well controlled; (2) in-person schooling is crucial for children’s growth; and (3) infection prevention/hygiene measures work. Those who were not in favor of sending the children to school expressed concerns related to the lack of adherence to infection prevention measures, especially in groups of children. Those who felt uncertain about making a recommendation generally cited the lack of evidence and careful weighing of the risks and benefits.
When evidence is lacking, we often turn to an expert consensus. The heterogeneity in this survey of a panel of diabetes leaders highlights the uncertainty of the current moment. While there was no clear consensus, the majority of respondents would ultimately advise the patient to send her children to school and seem to believe the benefits of children receiving in-person education outweigh the risks to a parent with DM1. Notably, there seemed to be a divide based on provider age, as “younger” (age <60) providers (including three who have DM1 themselves) were more willing to recommend sending the children to school than their “older” (age >60) counterparts. However, reservations remain given the lack of peer-reviewed evidence and unreliability of adherence to infection prevention measures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.