
Abstract
Diagnosing the underlying cause of persistent, mild hyperglycemia can be challenging. In normal weight adults, the differential diagnosis includes glucokinase mutation-maturity onset diagnosis of youth, or “MODY 2” (GCK-MODY), a stable, benign, autosomal dominant condition with an elevated glucose set-point. 1 It also includes early type 1 diabetes (T1DM). 1 Traditionally, clinical phenotype is obtained at presentation from history and laboratory results, followed by a period of observation to assess disease progression. Clinical work-up might include genotyping, but turnaround time is typically slow, also genotyping is relatively expensive. The two patients outlined below presented with a similar degree of hyperglycemia. Interstitial glucose monitoring was used to help with the underlying diagnosis: In classical GCK-MODY, average (median) glucose is elevated, yet glycemic variability is normal.1,2 In contrast, early T1DM is associated with an increase in glycemic variability. 3
Presenting Clinical Features
We describe two European New Zealanders who pre-sented with mild hyperglycemia, in whom endocrine and medication-related causes of hyperglycemia had been excluded.
Patient 1 aged 32 years, BMI 23, had a family history of ‘type 2 diabetes’. HbA1c was 40 mmol/mol. Fasting plasma glucose was 115 mg/dL, GAD (glutamic acid decarboxylase) antibody titre was normal. A second degree relative with ‘mild diabetes’ had a gene mutation consistent with probable GCK-MODY, but also had evidence of an autoimmune tendency (autoimmune thyroid disease, weakly positive GAD antibodies). It therefore seemed likely the relative had GCK-MODY, but this diagnosis was not confirmed. Patient 1 was given a provisional diagnosis of GCK-MODY. Patient 2 aged 33 years, BMI 26, presented with non-specific tiredness. A first-degree relative had T1DM. Fasting glucose was 124 mg/dL, HbA1c was 42 mmol/mol and the GAD antibody titre was just above the reference range. A provisional diagnosis of early T1DM was made, but GCK-MODY could not be excluded at the time of clinical review.
Use of Interstitial Glucose Monitoring as a Diagnostic Aid
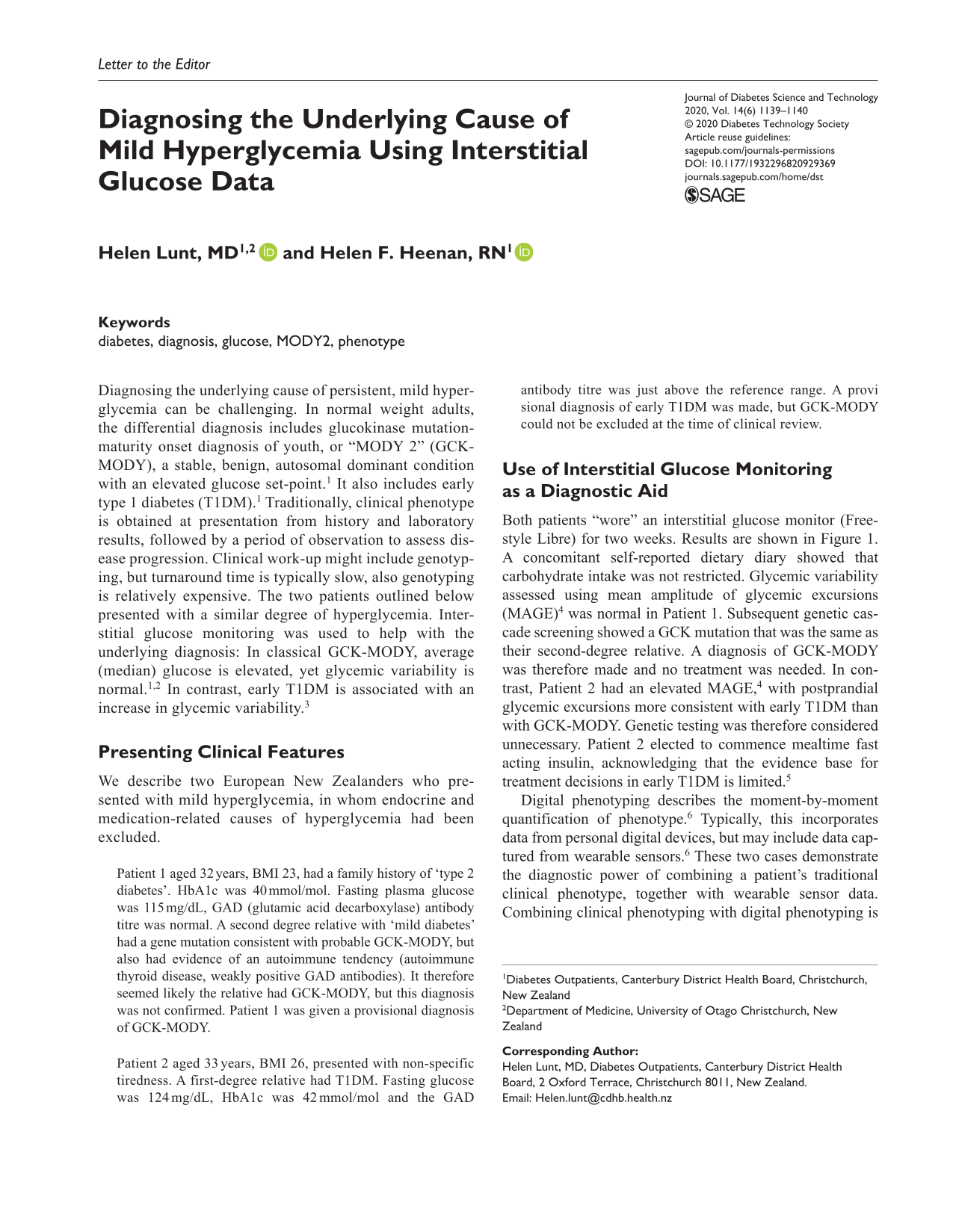
Both patients “wore” an interstitial glucose monitor (Freestyle Libre) for two weeks. Results are shown in Figure 1. A concomitant self-reported dietary diary showed that carbohydrate intake was not restricted. Glycemic variability assessed using mean amplitude of glycemic excursions (MAGE) 4 was normal in Patient 1. Subsequent genetic cascade screening showed a GCK mutation that was the same as their second-degree relative. A diagnosis of GCK-MODY was therefore made and no treatment was needed. In contrast, Patient 2 had an elevated MAGE, 4 with postprandial glycemic excursions more consistent with early T1DM than with GCK-MODY. Genetic testing was therefore considered unnecessary. Patient 2 elected to commence mealtime fast acting insulin, acknowledging that the evidence base for treatment decisions in early T1DM is limited. 5
Two weeks of interstitial glucose data. (A) Patient with GCK-MODY. (B) Patient with untreated early T1DM. GCK-MODY, glucokinase mutation-maturity onset diagnosis of youth; T1DM, type 1 diabetes.
Digital phenotyping describes the moment-by-moment quantification of phenotype. 6 Typically, this incorporates data from personal digital devices, but may include data captured from wearable sensors. 6 These two cases demonstrate the diagnostic power of combining a patient’s traditional clinical phenotype, together with wearable sensor data. Combining clinical phenotyping with digital phenotyping is likely to become commonplace in settings where relevant biosensor information is easy to obtain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.