
Abstract
Background:
Support groups play an important role in diabetes understanding and education. This study aims to find connections between participating in diabetes-related online communities (groups and forums) and the self-reported degree of self-care management and health problems associated with type 1 and 2 diabetes.
Methods:
A cross-sectional study using an online survey was conducted and 307 participants were recruited. Participants were asked about diabetes self-care management (glucose management, healthcare, dietary restrictions, and physical activity) and complications related to the disease, as well as their participation in online social groups and forums (duration, time, and intensity).
Results:
Belonging to diabetes-related online support groups (OSGs) was associated with lower scores in healthcare and self-management of diabetes (M = 2.98, SD = 1.07, n = 207, for belonging to OSGs; and M = 4.22, SD = 0.59, n = 97, for not belonging to OSGs). These differences were not statistically significant for type 1 diabetes individuals (M = 4.33, SD = 0.47, n = 28, for belonging to OSGs, and M = 4.29, SD = 0.48, n = 52, for not belonging to OSGs), but were highly significant for type 2 diabetes (T2D) individuals (M = 2.41, SD = 0.68, n = 144, for belonging to OSGs; and M = 4.14, SD = 0.64, n = 61, for not belonging to OSGs). People with both type 1 and 2 diabetes reported to have suffered more complications derived from diabetes when they belonged to an OSG, but greater statistically significant differences were found in type 2 individuals.
Conclusion:
Patients with T2D who participate in OSGs show a higher correlation with having lower levels of diabetes self-care management as well as health complications related to the disease.
Introduction
Diabetes is one of the most prevalent long-term diseases (LTDs) of this age. Nowadays, people affected by an LTD 1 are increasingly participating in digital communities, 2 often referred to as online support groups (OSGs), to share feelings, gain emotional support, and obtain information about the disease. Diabetes care requires both disease understanding and disease education, as well as emotional and informational support for both types of diabetes—in type 1 diabetes as a new learning outcome in their early education and in type 2 adult-onset diabetes as a relearning outcome once they have already established their habits.
Online Support Groups
Online support groups can be forums where participants feel supported in instances of emotional distress rising as a result of the highly demanding self-care regimes and medical complications in diabetes mellitus. The stress-buffering model explains how social support may give tools to manage the self-care of diseases and even improve their condition through support satisfaction.3,4 In the case of type 2 diabetes (T2D), a study by Lee et al showed the importance of informal support (family and friends) in giving the patient autonomy and agency to empower them and make them able to take their own decisions in order to cope with the daily routines involved in managing the disease. 5
Professionally operated support groups were first conceived after proving useful in improving quality of life through emotional support in women with metastatic breast cancer in the 1980s. 6 This kind of group required the presence of a medical team (doctors, therapists, and nurses), so were costly to implement. Online Support Groups, however, have been flourishing in the last few years and are, on the contrary, self-help support groups, fully organized by their members with no professional management. Online Support Groups combine the concept of a support group with an online forum. Online forums are “groups of people with common interests and practices that communicate regularly and for some duration in an organized way over the Internet through a common location or mechanism. 7 ” Online forums are characterized by 24/7 ubiquitous availability, anonymity, selective disclosure, and social networking. 8
The core activity of these groups revolves around sharing personal opinions and experiences, in addition to selecting and distributing information in order to meet each poster’s needs. 9 Discussion threads in online forums can be viewed as a form of group communication, since they have the same features of face-to-face support groups, namely size, interdependence, task, identity, and norms. 10
Some popular sites like Facebook (FB) or Twitter have turned into community spaces where people affected by an LTD can interact with each other in a similar way to how they would on a forum. 11 With 1.59 billion daily active users on average, 12 Facebook is one of the most popular sites among today’s population. Facebook allows for an agile and easy organization and management of public, private, or secret groups, often with very few participants, on any topic its users may be interested in. To enter a private group, an outsider must be invited by an existing user. 13
In general, FB groups and online forums on health issues are thriving and provide support to their users. 14 This support can be of different nature, specifically in terms of confirmation, information, advice, and empathy. 15 In general, health-related OSGs may be used either to meet an information requirement—which is strongly related to asking specific questions—or to gain emotional support—which is about sharing opinions and providing support for others.16-18
Diabetes-Specific OSGs
People with diabetes come to diabetes online communities in order to find both health information and social or emotional support, meaning that these OSGs become a source of health information and a resource to provide a sense of community. 19
However, and although many users with diabetes may indeed seek to participate in these OSGs for emotional support exclusively, the main function of most OSGs is to provide instrumental support, as an information source. 20 In addition, although users may be aware of the nonexpertise of the source, the information shared in OSGs gains credibility through social validation 21 —a user consensus is reached through comments of agreement and a general lack of criticism, regardless of the information’s veracity and the expertise of the source.
The quality of information differs among different OSGs. A study by Weitzman et al 22 found that although information may be aligned with diabetes science or clinical practice recommendations, there are gaps in medical disclaimer use, external review approaches (outbound links), and internal approaches (moderation). Hence, misinformation about diabetes, including its “cure”, has been found. As users become more connected and attached to these communities, the information they access through these networks becomes more meaningful to them. 23 The fact that information shared and consumed in OSGs may not be 100% rigorous and veracious adds to the problematic connection between these groups and overall diabetes self-care management.
Therefore, participating in such health-related OSGs can be problematic, especially in the case of diabetes care as it involves serious dietary restrictions and self-care management routines. 24 Instead of giving autonomy and agency to self-manage the disease according to the aforementioned buffering model, OSGs may be used to gain supportive information on consolidated negative habits that are hard to change. In communication studies, an individual’s internal self-aware inconsistencies have been theorized as a cognitive dissonance. 25 According to this theory, the individual feels the need to alleviate the distress caused by inconsistencies in beliefs, ideas, values, and behaviors. More recently, in the social networking age, the social reinforcing spiral 26 poses that media is used selectively as a social reinforcement of pre-existing attitudes and beliefs through the individual exposing themselves to information that reaffirms them.
The Outcomes of Diabetes-Related OSGs
Some studies show that a diabetes self-management program, based on professional and clinical guidelines, can be beneficial in terms of improving the emotional well-being of the user, quality of life, and hemoglobin A1c (HbA1c),27-29 although it may not always imply changes in other health or behavioral indicators.28,30
Another study suggested that reading blogs is associated with lower HbA1c values, 31 but this association does not prove causation, and the study did not specify the clinical quality of the blogs that participants read.
Although the existing literacy suggest that participating in diabetes online communities provides more benefits than negative consequences regarding the emotional well-being and quality of life of people with diabetes, including social support or diabetes self-care levels, it is unknown if participating in these digital online communities has any effect on health outcomes.29,32
Furthermore, participant involvement may rely heavily upon reminders and encouragement from a diabetes educator and immediate family members, 33 who may not be part of diabetes online communities or OSGs. We could not find other studies focusing on the association between diabetes self-management and belonging to an OSG without professional management.
This study specifically aims to find correlations between participating in diabetes-related online forums or social groups and the degree of self-care management and health problems that may be associated with diabetes. 34
To the best of our knowledge, no studies have delved into the way participating in diabetes-related online communities and support groups without professional management affect patients’ health and diabetes self-management:
RQ1: Is belonging to a diabetes online social group correlated to mean Diabetes Self-Management Questionnaire (DSMQ) score?
Furthermore, and although the rise of obesity levels among children is contributing toward an increase in juvenile cases of T2D, 35 patients with T2D tend to be an older and more heterogeneous segment than type 1 in the moment of the diagnosis, with more problems related to hypoglycemia and hyperglycemia. A side effect of type 2 segment’s sociodemographic and lifestyle characteristics is functional impairment and comorbidities—the confluence of different diseases, which may be reasonably treated individually: 36
RQ2. Is the association between belonging to a diabetes online social group and the individual’s healthcare and self-management of diabetes different for type 1 and 2 diabetes?
Methods
A cross-sectional study using an online survey was conducted between May 19 and September 6, 2018. The study was approved by the Ethical Committee of the University of Pompeu Fabra. The questionnaire was created using Google Forms. Participants were recruited online via a banner on a website named “Dulces Diabéticos” 37 and through posts in both diabetes online forums (being posted once in “Diabetes Foro”) 38 and FB groups related to diabetes. Participants took as much time as needed in order to complete the survey (an average estimated time of five minutes). It was stated in the consent that the survey was voluntary and participants were not going to be compensated for completing it. Only datasets with complete data were analyzed. Two participants were excluded from data analyses because they did not provide their consent to participate in the study. Thirty five more participants were also excluded because they claimed not to have diabetes. The final sample contained 307 Spaniard participants (mean age: 43-44; SD = 9.45; 49% men). Their academic studies included elementary school (8%), secondary school (42%), bachelor’s degree (39%), master’s degree (7%), PhD studies (1%), or none (2%). A total of 210 participants had T2D (68%), 82 had type 1 diabetes (27%), and the rest reported having other types of diabetes.
The survey consisted of four parts and was conducted in Spanish. First, participants were asked to answer questions related to diabetes and their behavior as patients, including the age of diagnosis and the medications being taken. The following set of questions referred to their internet usage, membership of online social groups, and the reasons why they belonged to these groups. Of all the participants, 68% were members of OSGs related to diabetes, while 32% were not. Among those who were members of OSGs, 90.8% were members of a FB group, 41.5% of a diabetes-related forum, 3.9% of a health-related forum and, finally, 1.4% were members of other online forums. Regarding the duration of belonging to these forums, 4.3% of them had been members of online forums for less than 6 months, 58.9% between 6 months and 3 years, and 36.7% for more than 3 years.
Regarding their medication, 68.1% of participants belonging to a diabetes OSG (n= 207) reported the intake of oral antidiabetics; 48.3% reported the intake of insulin; 7.2% were medicating on natural remedies; 4.3% reported no intake of medication and 1.4% reported the intake of other medication. On the other hand, 62.9% of people not belonging to a diabetes OSG (n = 97) reported the intake of oral antidiabetics; 45.4% reported the intake of insulin; 3.1% were medicating on natural remedies; 16.5% reported no intake of medication, and 1% reported the intake of other medication.
The final set of questions referred to diabetes self-management, based on the DSMQ. 39 Four subscales, “glucose management” (GM), “dietary control” (DC), “physical activity” (PA), and “healthcare use” (HU), as well as a “sum scale” (SS) as a global measure of self-care were derived. One item requests an overall rating of self-care and is included in the “sum scale” only. All items were formulated as behavioral descriptions taking the first person view.
Results
First, we measured the overall scale of reliability. Cronbach’s alpha for the overall scale (12 items) was 0.967, which indicates a high level of reliability for our sample (n = 293). Cronbach’s alpha was 0.925 for GM (3 items), 0.919 for DC (4 items), 0.882 for HU (2 items), and 0.970 for PA (2 items). Before trying to answer our first research question, we calculated the correlations between the subscales of our scale. There was a strong and positive correlation between the five subscales, statistically significant at the level 0.01, which were strongly positively correlated, with Spearman’s correlation coefficients ranging from 0.581 to 0.922.
To analyze whether belonging to a diabetes OSG is correlated to mean DSMQ score (RQ1) we performed an independent sample t-test. We found that people not belonging to OSGs (32% of the sample) related to diabetes had a statistically significantly higher score for healthcare and self-management of diabetes (M = 4.22; SD = 0.59; n = 97) compared to those belonging to OSGs (68% of the sample) (M = 2.98; SD = 1.07; n = 207), t(302) = 10.701, P = .000. The same is observed for each of the subscales, as shown in Table 1.
T-test for Subscales of the Healthcare and Self-Management of Diabetes Scale and Diabetes Care (N = 304).
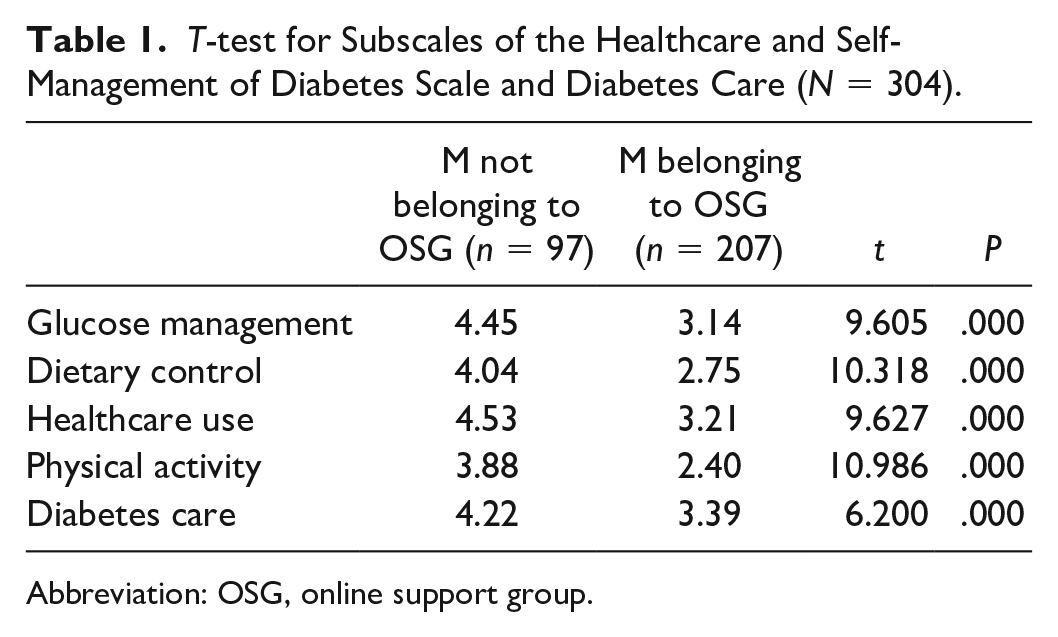
Abbreviation: OSG, online support group.
Our second research question related to the association between the individual’s type of diabetes (type 1 or type 2), belonging to diabetes OSGs and its effect on their healthcare and self-management of diabetes. For type 1 diabetes, we found that the differences were not statistically significant at all. Means for the overall scale (healthcare and self-management of diabetes) were almost equal (M = 4.33, SD = 0.47, n = 28, for not belonging to OSGs; and M = 4.29, SD = 0.48, n = 52, for belonging to OSGs), t(78) = 0.365, P = .716. The same was also observed for each of the subscales, as shown in Table 2.
T-test for Subscales of the Healthcare and Self-Management of Diabetes Scale and Diabetes Care for Type 1 Diabetes (N = 80).
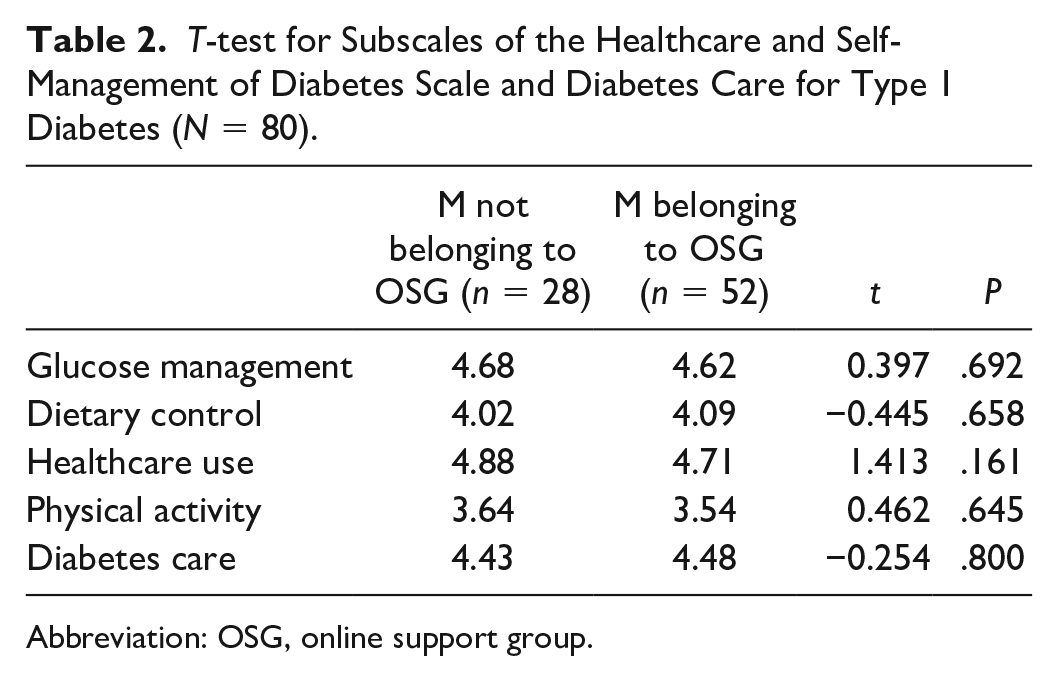
Abbreviation: OSG, online support group.
We performed the same assessment for T2D individuals. However, in this case, we found that the differences were particularly statistically significant. Means for the overall scale (healthcare and self-management of diabetes) were almost equal (M = 4.14, SD = 0.64, n = 61, for not belonging to OSGs, while M = 2.41, SD = .68, n = 144, for belonging to OSGs), t(203) = 16.904, P = .000. See Figure 1 for differences between both types of diabetes.
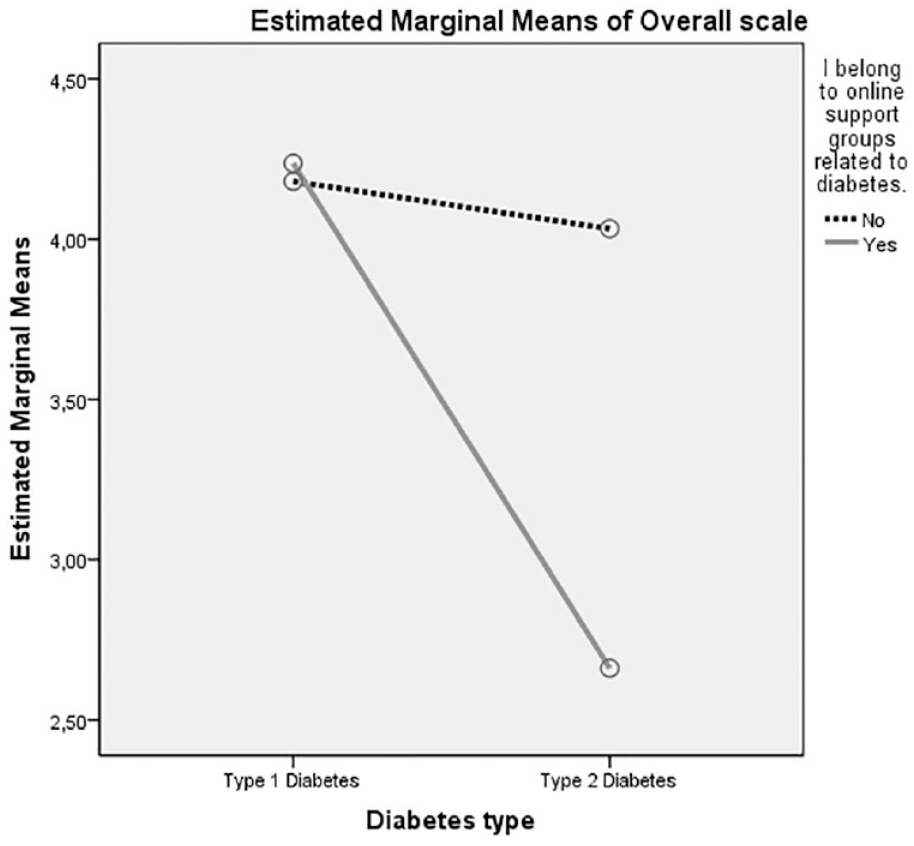
Plot of the mean healthcare and self-management of diabetes score for each combination of groups belonging to OSGs and diabetes type.
The same was also observed for each of the subscales, as shown in Table 3. All healthcare and self-management items score over 4 (with the exception of physical activity, 3.91)—with glucose management (4.34) and healthcare use (4.35) being the highest for patients not belonging to OSGs; whereas these items score under 3 for patients belonging to OSGs (2.90 for diabetes care, and the rest under 2.60, being dietary control and physical activity the lowest, 2.17 and 1.89 respectively).
T-test for Subscales of the Healthcare and Self-Management of Diabetes Scale and Diabetes Care for Type 2 Diabetes (N = 205).
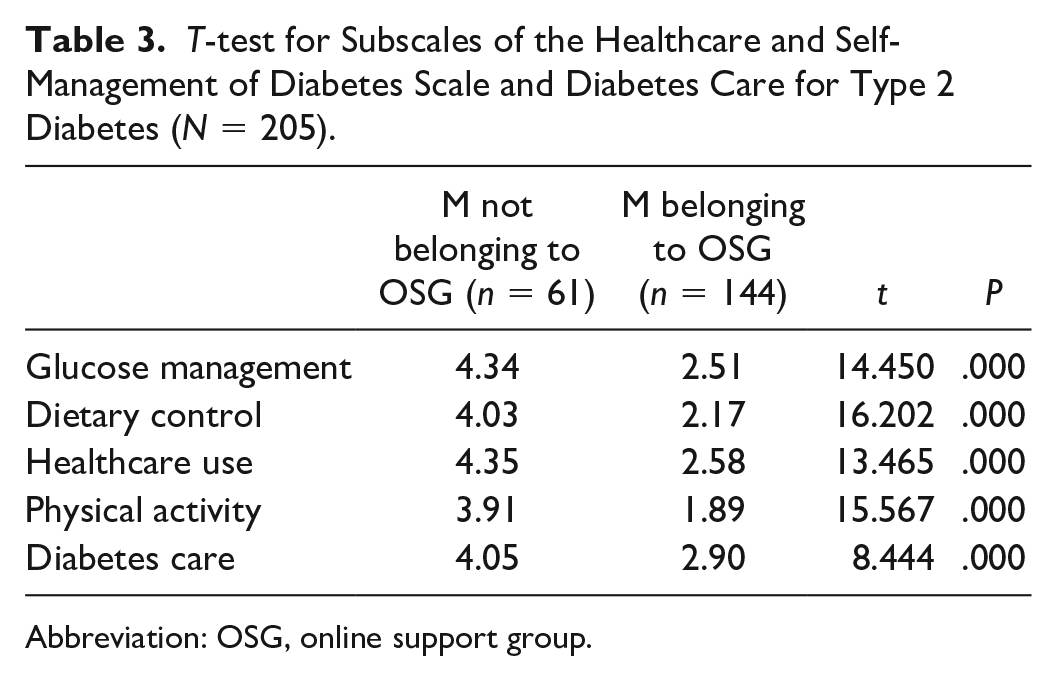
Abbreviation: OSG, online support group.
Finally, we did the same for the variable I have suffered complications derived from my diabetes (which includes hypoglycemia, hyperglycemia, retinopathy, nephropathy, or diabetic foot, among others). Results show the differences between groups (M = 1.46, SD = 0.88, for type 1 patients not belonging to OSGs, and M = 2.60, SD = 1.55, for those belonging to OSGs; while M = 1.95, SD = 1.28, for type 2 patients not belonging to OSGs and M = 4.77, SD = 0.72, for those belonging to OSGs).
Discussion
This study has found a strong relationship between the use of diabetes OSGs and the reporting of poor healthcare and diabetes self-management. This finding is particularly conclusive for patients with T2D given their dominance in the sample as well as much greater significance of the variables’ correlation if applied to the T2D sample. These findings may raise issues on how the healthcare and self-management practices influence or are influenced by those groups.
Type 1 diabetes users tend to be diagnosed when they are children or adolescents with no long-term consolidated dietary and social habits, whereas patients with T2D are diagnosed as adults that have developed the disease because of (rather than despite) dietary and social habits. Admittedly, self-care management attitudes such as glucose management, diabetes care, or healthcare usage would not be part of habits of patients with T2D before being diagnosed with type 2, but they are closely related to dietary control and physical activity, which were established as positive or negative habits before the diagnosis.
Given the dominance of T2D in the sample, and the strong significance between those that use OSGs and those that do not, we can extract a connection between the use of OSGs and a poor self-management of the diabetes disease by T2D. As a limitation of the analysis, we cannot predict the direction of effects between using OSGs and the disease’s self-management, that is, we do not know whether the self-management complications are the cause or the consequence of such a type of OSG use. However, the connection itself is an outcome that adds to the literature on online communities use by T2D. Specifically, these findings put the focus on the need to further research how the buffering model may be applied to the case of OSGs used by T2D. In other words, the use of OSGs to empower T2D—by informally granting them agency and autonomy to make key decisions and improve the day-to-day of the disease—does not seem straightforward. More research is required on this topic.
Having admitted this limitation, it is likely that intervention or assistance is required for those patients to select and critically analyze the information they encounter in OSGs, especially given the great accessibility of those OSGs through applications in smartphones, tablets, or laptops. Recent media-use theorizations 27 have emphasized that media and users act as dynamic reinforcers that mutually affect each other. Following this rationale, the social media user takes an active role and selects both the format and the content of information as a result of his/her established beliefs and attitudes. The way he/she uses these media in turn reinforces his/her beliefs and attitudes in a spiral manner. 27
Results may assist both patients with diabetes and medical professionals in managing online communication and resources more effectively, particularly when patients seek informational support from others who are more experienced in the field of diabetes.
This study is not without limitations. First, the quantitative nature of the study has significant limitations, specifically the use of self-reported scales and selection biases because of the online recruitment. Some qualitative approaches may help gain insight into the impact of online social groups. Second, the sample of type 1 and 2 diabetes participants is unequal (27% of the sample was type 1), probably because OSGs are heterogeneous and type 1 represents fewer than 10% of people with diabetes, 34 thus conclusions are mainly drawn for people with T2D.
Conclusion
This study examines the correlations between participating in health-related OSGs and forums, and the healthcare and self-management of diabetes. Results show that belonging to these forums is connected with lower levels of diabetes self-care management as well as health complications related to the disease. This connection is not statistically significant for type 1 diabetes users, but it is very strong for T2D users.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.