
Abstract
Type 1 diabetes is a unique disorder, requiring constant and vigilant assessment of glucose levels, food/snacks consumed, activities and exercise, emotions and stress, hormonal influence, and illness. No other diagnosis is as intensive in terms of the “burden” of care that impacts the patient/family physiologically, cognitively, and psychologically. Several Do-It-Yourself (DIY) closed-loop systems currently exist and can provide options for patients and families looking to reduce the burden of type 1 diabetes. However, as the systems are not Food and Drug Administration approved, healthcare providers are faced with the decision of whether to support patients using DIY systems. This manuscript discusses the ethics of choice and patient autonomy from the perspective of patient/family and healthcare provider. A set of proposed guidelines for healthcare providers are also presented for consideration when interacting with a patient or family who desires to use a DIY system to help manage type 1 diabetes.
Keywords
The Family
Parenting a Child With Type 1 Diabetes
Being responsible for a child with type 1 diabetes requires constant vigilance and a significant learning curve to ensure the immediate safety and best long-term outcomes for your child. It is a daunting and potentially life-threatening task. The amount of considerations and influencing factors are endless and overwhelming. As the parents of a child with type 1 diabetes, we can speak to the struggle because our son was diagnosed at age 3, and we live this very existence every day.
Managing diabetes did not come naturally for us. However, we knew that we needed to learn as much as possible to ensure our son’s health and safety. The thirst for knowledge was accompanied with a better understanding of the very real risks and worry about the possible complications associated with suboptimal control. We take the responsibility for his care very seriously and it is our top priority.
Selecting Diabetes Management Tools
In the years since diagnosis, we have learned so much. Sources of information are everywhere, including from our care team and our own research and experience. We have learned many things including the important lesson that not all diabetes devices are created equal and what works best for others may not work best for us (and vice versa). Being given the autonomy to decide which devices can help us best manage diabetes is a critical component to successfully reaching our goals for glycemic control and easing the burden of the diabetes on our family. Moreover, we have learned that your provider is the gate-keeper to the ability to obtain the management tools that work best and an open, honest, and supportive relationship between patient and provider is critical.
Arguably, the most important tool for our family has been the adoption of a continuous glucose monitor (CGM). This helps us to mitigate the very real risk of an undetected hypoglycemic event. We routinely rely on the CGM to alert us of high and low blood sugars, both when our son is nearby and away (such as at school). Using the CGM, we started to see how poorly we were handling high blood sugars. We were so scared of stacking insulin using multiple daily injections that our son frequently had sustained high blood sugars. Research showed us that an insulin pump could provide us the flexibility to dose meals in the real-world life of a three-year-old little boy. We started a pump four months after his diagnosis, thinking we might finally obtain some control; however, we still had a difficult time keeping blood sugars steady and in target range. It seemed like we had all the tools, but just could not manage our settings properly to have better results. We knew we had to do better; there must be a better way.
Do-It-Yourself (DIY) Hybrid Closed-Loop Systems
Despite the tools made available to us, we were lacking the glycemic control and failing to meet the goals that we had set for ourselves. We knew we needed to make a change. Like many others, we were struggling to meet our goals and our son’s HbA1C (A1C) was well above American Diabetes Association’s (ADA) stated goal of 7.5%. 1 We knew we wanted to do better, so we did what any 21st century parent does—we scoured the internet.
Through our search, we found the OpenAPS 2 (and eventually Loop 3 ) documentation on how to build our very own Do-It-Yourself (DIY) hybrid closed-loop system. Our frustration and guilt had grown so intense that we knew we had to do something different and give the DIY systems a try. It seemed logical to us that an algorithm could take the data from the CGM and the pump and adjust insulin delivery accordingly and objectively. This was something our human brains were desperately trying to do but were failing miserably. We spent several weeks reading to make sure we understood how this system would work, and more importantly, how to make it stop if necessary. The documentation was very thorough, organized, and clear. We finally acquired all the necessary hardware, only needing an updated prescription for pump supplies, as the DIY system required a different supply. We approached our provider and were denied. There was no room for discussion, our decision to use DIY was not supported. Instead of taking that denial as an end to our journey, we decided to find another provider.
The Results Speak for Themselves
The DIY system has never been a set it and forget it system for us. It does require setting adjustments, which can sometimes be quite challenging to get just right. It requires a desire and willingness to understand the system and understanding of the associated risks. The results, however, speak for themselves. We have learned that DIY hybrid closed-loop systems are unequivocally the best option for our son and the ability to use these systems has changed our lives. Our son’s A1C dropped from 8.1% to 6.3% within four months and has remained stable. Our family is more rested and more balanced since we are finally able to think about something other than diabetes. Rarely now, are we awakened by a glucose alert overnight, and when we are, the severity is typically much less due to the DIY system already attempting to mitigate (ie, setting a lower temporary basal rate to reduce insulin delivery in advance of the dropping blood sugar levels). Of important note, to date, we have not experienced any adverse events.
We are even able to select DIY tools to adapt to various situations and enhance our diabetes management user experience. In the continuing spirit of the #wearenotwaiting movement, we can use a DIY hybrid closed-loop system with the Omnipod (Insulet Corporation, Acton, MA, United States) insulin pump now, alleviating the worry of a nonwater proof, older pump. We also can use a Nightscout 4 site to collate CGM and pump information from our DIY loop system, to observe and monitor basal adjustments, predicted blood glucose levels, carbs entered into the system, bolus units received, set remote targets, and for louder alarms that continue to alarm until manually silenced.
At this point in time, there are no commercial systems that can match the features of the DIY systems, however, as all systems are on the brink of new discoveries, as early adapters, we would always be open to new emerging technologies (either DIY or commercial).
Patient/Provider Relationship
The relationship between patient/family and provider is most effective when there is a mutual understanding of goals, abilities, and open and honest communication to form a trusted bond. The provider is the gate-keeper to all decisions regarding prescription management tools; however, the patient is responsible for using the management tools daily and maximizing their benefit. Benefit should be measured most obviously in glycemic control but easing the burden of care and improving quality of life should also be a consideration. Without patient/caregiver input, it must be nearly impossible for a provider to determine which tools will work best for every unique family and circumstance.
For us, finding the right provider took some trial and error. We have found that certain practices/institutions were rigid, which we perceived as unsupportive, possibly due to fear of legal ramifications and/or lack of familiarity with these systems. Certainly, there was no intentional maleficence, but the mutual trusted bond was not present, and our results reflected that. When we found the right provider and institution, our entire experience has been different. We feel more empowered from the support of a provider, and the results have proven this partnership is truly working.
The diagnosis of type 1 diabetes was not a choice our son or family made. But with the diagnosis, came the reality that most of the care and decisions were ours. Therefore, the decisions of how we care for our son should be ours as well, in collaboration with our provider. Do-It-Yourself solutions should be considered as viable options for families who seek to improve their ability to manage diabetes and ease the burden of care. It is our hope that more providers become open to discussions with patients about DIY systems.
The Provider
An Intensive, Self-Managed Disease
Type 1 diabetes is a unique disorder, requiring constant and vigilant assessment of glucose levels, food/snacks consumed, activities and exercise, emotions and stress, hormonal influence (ie, growth hormone, pubertal, or menstrual cycle), and illness. No other diagnosis is as intensive in terms of the “burden” of care that impacts the patient/family physiologically, cognitively, and psychologically. No matter how well-controlled (or not) one day, the next day holds the same challenges. It is a condition that, at the present time, cannot be cured. At best, with an almost inhumane degree of attention, families strive for best possible control in hopes of protecting their child from the well-known long-term complications of uncontrolled diabetes and most worrisome, the short-term complication of severe overnight hypoglycemia leading to death.
In today’s world, from the earliest time after diagnosis, most families become aware of the need to learn as much about the process of diabetes and ways to start self-management for their child. Many families are quite content to have all adjustments done by the provider, but some families energetically embrace the ability to learn about trends and adjustments to insulin therapies to keep blood glucoses maximally in the target zone. One of the definitive manuals to assist families in their educational process, Understanding diabetes: A handbook for people who are living with diabetes, states “We encourage patients and families to be actively involved in making insulin dose adjustments. 5 ” In today’s typical outpatient visit, a significant portion of time is not only dedicated to making needed adjustments to insulin therapy, but also teaching families how and why, assisting the family to improve skills in self-management for their child. The relationship formed between provider and family is crucial in forming a positive and trusting bond, where the best control possible (as evidenced by greatest time in range, with minimal hypoglycemic events) for their child is the upmost shared goal.
The current focus in the partnership of care for the patient with diabetes has shifted to acknowledge 99% of self-care vs 1% time spent in the office in face-to-face care by the provider. 6 The families that eventually consider DIY systems are the same families that quickly embrace CGMs and continuous subcutaneous insulin infusion, and are often part of diabetes online communities, essentially searching for the “best possible” for their child. They are the same families that embrace the self-care model and seek a relationship with their provider of education, engagement, and support. These same families become comfortable with self-care management for their child, and feel empowered to make decisions, but can be overwhelmed with the enormity of necessary decision-making times. As Food and Drug Administration (FDA)-approved CGMs produce data every five minutes, families quickly realize that it is impossible to make 288 decisions per day. This pressure is almost inhuman as prompt decisions are necessary not on a daily or hourly basis, but moment-to-moment. These same families often live in the technology world of computers and software, and easily embrace the premise of software tools or algorithms that can assist with decision making. For example, patients and providers are comfortable with a bolus calculator on an insulin pump, and do not routinely double check the calculations. Thus, the attraction for a subset of families to embrace DIY technology to help them achieve their personal goals, and because the current FDA-approved systems are not meeting these needs, families are choosing another path.
The community-built automated insulin delivery systems were built prior to FDA-approved commercial systems (MiniMed 670G 7 [Medtronic USA Inc., Minneapolis, MN, United States] and Tandem Control-IQ 8 [Tandem Diabetes Care Inc, San Diego. CA, United States]) becoming available. These community-built systems continue to provide advantages such as individualized targets, remote monitoring, and even tools 9 to recommend changes adjustments in standard insulin pump settings (basal rates, insulin sensitivity factor [ISF], and carb ratio) which is of utmost important to families of younger children.
The ADA recognized the need to include technology in their 2019 Standards of Medical Care which not only acknowledges the value of increased technology of pump and CGM usage, but it also makes comment regarding the use of DIY systems, “although these systems are not FDA approved or recommended. 10 ”
The Ethics
The commonly used principles of healthcare ethics—justice, autonomy, nonmaleficence, and beneficence—can and should be applied in this discussion. All these principles may be open to interpretation, but they can be a foundation for decision making in this evolving and complex technology world we live. Providers certainly live by the dictum of “first do no harm, benefit only” yet, even this is unclear in today’s world when many approved therapies are painful, expensive, and include possibility of disability or not working. Protocols developed within institutions help to guide providers and protect patients from harm. However, using the principle of autonomy, persons own their own (or their children’s) lives. The parents who are interested in DIY systems must have educated themselves, be competent to make decisions for their family, and be free from coercion from outside or provider influence. This principle recognizes and supports a family’s ability to choose what is right for their child, understanding the risks and benefits. The final principle of justice targets not only resource allocations but also procedural processes. So, the questions in this setting are related to access to the required supplies needed in order to use DIY systems and whether there were guidelines that allow for fair treatment as any other patient/child.
As most providers are immersed in “do no harm,” which harm is greater: (1) the support of a family willing to take the risk of an unregulated, unapproved system that has been programmed to make the same decisions that they would or (2) nonsupport of a family using a system that has improved their child’s time in range, decreased their child’s hypoglycemic time, and improved the family’s quality of life? Although some of the “parts” of the DIY systems are approved and regulated (CGM and pump), it is the risk of the algorithm itself and the potential communication difficulties of this nonregulated system that lead some providers to refuse support and, in some cases, refuse to continue care. So, despite our professional community’s role in the promotion of self-care and self-management decision making, the line is drawn in using nonregulated systems. However, what assurance does any provider have that even a simple, approved device, such as an insulin pen, is used “as instructed”? If a family member is instructed to dose insulin three to four times daily, but the family finds that giving insulin five times daily keeps the blood sugar in control better, would that decision be supported? This is certainly a simplistic example, but shows that diabetes care and management is complex, and many families are able to modify their child’s diabetes regimen to best serve the individual needs of their child and promote their family’s quality of life.
Similarly, patient/family “right to choose” should also be addressed. More commonly addressed in the Oncology arena, right-to-try laws for terminally ill patients that have exhausted other options have some interesting correlations. 11 Families or patients are similarly frustrated with the lengthy FDA review process and willing to bypass full drug testing. It is interesting that the healthcare provider for the patients may recommend an experimental treatment, but patients or families are required to give written informed consent. “Health-care systems are often paternalistic and may treat the disease rather than the patient. . . For patients to make a well-informed decision, they must be provided good, clear knowledge regarding the benefits and limitations of experimental treatments. 10 ” Although diabetes is not a terminal illness, it is a chronic illness that requires all available resources, knowledge, and attention. It is imperative that patients or families have made available any and all tools to enhance quality of life while diligently caring for their child or themselves.
The healthcare provider writes a prescription for pumps and sensors that are FDA approved. It is the choice of the patient and/or family to utilize an unregulated control system. While this commentary is not intended to imply a legal debate, it is possible to support families who desire to use these unregulated DIY systems within a framework that ensures both parties are well positioned for success (Figure 1).
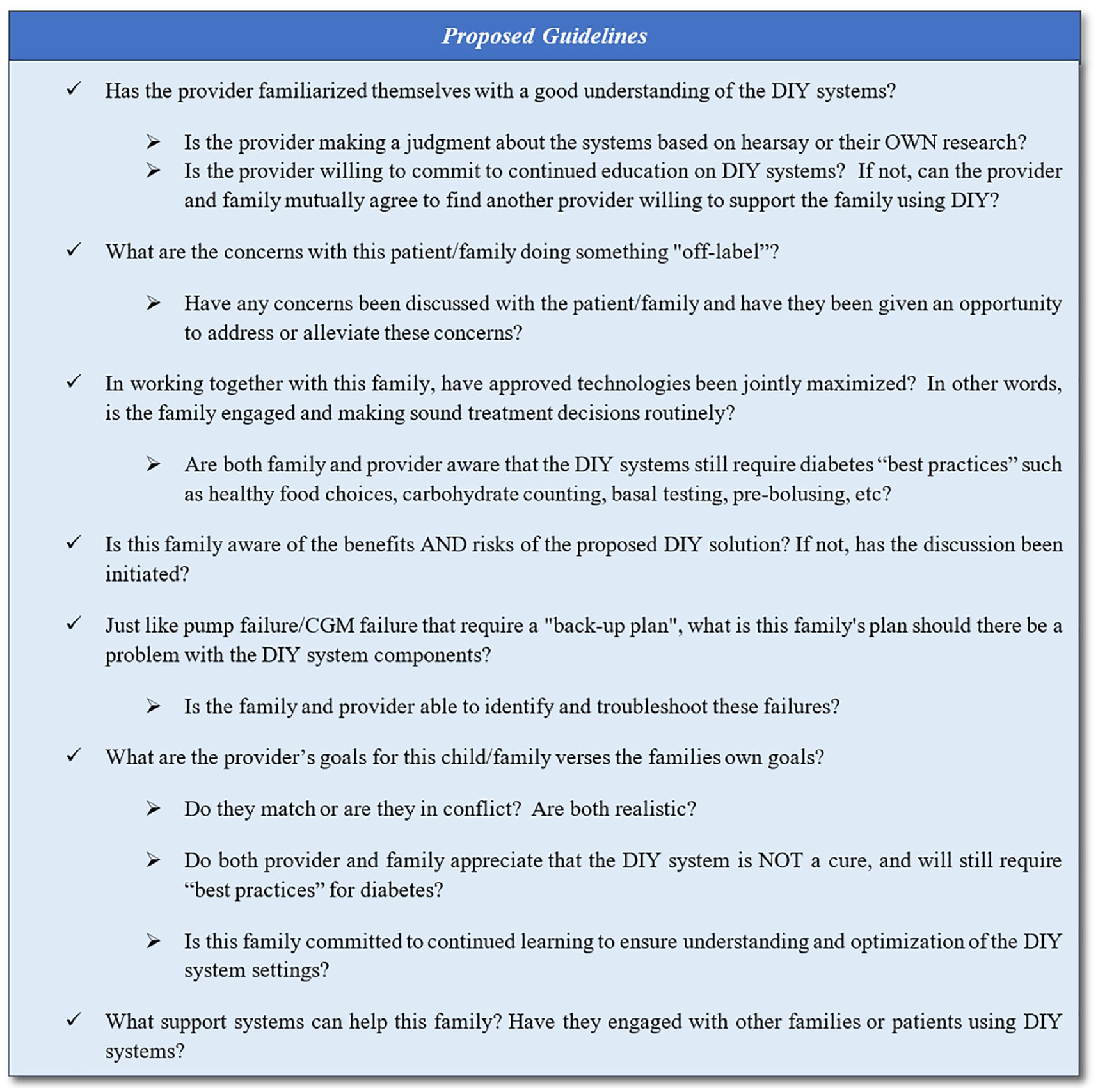
Proposed guidelines to support families using Do-It-Yourself hybrid closed-loop system (See Appendix A).
Conclusion
Nonregulated DIY systems may not be able to be “prescribed,” but if the above have been discussed with a family that is considering or already using a DIY system, and the concerns of the provider regarding the attention, engagement, knowledge, communication, decision-making skills, and back-up plans are met, it is appropriate to support the decision of the family and continue to interact with them.
Footnotes
Appendix A. Suggested Reading
Acknowledgements
The authors would like to thank Dana Lewis for her critical review and input.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.