
Abstract
In addition to the continuous use, the intermittent use of continuous glucose monitoring (CGM) is an application of CGM, expanding the typical medical use cases. There are a variety of reasons and occasions that speak in favor of using CGM only for a limited time. To date, these circumstances have not been sufficiently discussed. In this article, we define discontinuous or intermittent CGM use, provide reasons for using it, and expand on the benefits and possibilities of using CGM on a temporary basis. We aim to draw attention to this important topic in the discussion of CGM use and give examples for a different method of CGM use. As well, we would like to foster the allocation of CGM to the right patient groups and indications, especially in cases of limited resources. From a global point of view, intermittent CGM use is more likely to occur than continuous use, primarily for economic reasons.
Introduction
Usage of systems for continuous glucose monitoring (CGM) is increasing rapidly in various countries around the world, both in pediatric and adult patients with diabetes.1,2 There is increasing evidence showing beneficial effects of CGM on glucose control and other outcome parameters for people with type 1 diabetes (T1D) or type 2 diabetes (T2D), as well as in women with diabetes during pregnancy and their offspring.3-5 At the same time, there are also initial results indicating that CGM can be used successfully as part of interventions to prevent T2D, for lifestyle intervention or as a motivational device for people with poorly controlled diabetes.6,7
A range of different CGM systems exists. Some systems require calibration at more or less regular intervals and others do not need calibration anymore (so-called factory calibrated systems); some display glucose values automatically (real-time CGM [rtCGM]) on a handheld/smartphone or after an active scan (intermittent scan CGM [isCGM]). Most CGM systems provide alarms when glucose levels show trends head toward or reach specific preprogrammed thresholds. New systems can be used for insulin dosing in a nonadjuvant manner, meaning that no fingerstick blood glucose test is needed. It can also be distinguished between the personal CGM, where glucose values are displayed in real time, and the professional CGM (proCGM), which is worn by the patient in a blinded mode over a short period (eg, intermitted use for 6-14 days). 8 The data are retrospectively assessed by health-care professionals (HCPs) to detect glucose patterns and to adjust therapy. The efficacy of proCGM could be shown for children 9 and people with T2D. 10 Nearly all systems have glucose sensors that must be inserted under the skin into the subcutaneous tissue in order to measure glucose levels in the interstitial fluid and remain inserted for a duration from 6 to 14 days. A different rtCGM system has a sensor that is implanted under the skin for up to 180 days. CGM systems can be used in combination with multiple daily insulin injections with a syringe/insulin pen and most rtCGM systems can be used in combination with an insulin pump. This type of combination enables sensor-augmented pump therapy where insulin infusion is delivered according to the current glucose levels. In the next step, the so-called (hybrid) automated insulin dosing systems are established, that is, the basal insulin infusion rate is not only decreased in case of low glucose values but also automatically increased in case of high glucose values.
Use of CGM Systems in Daily Practice
CGM provides much more information over time across the glucose profile. Self-monitoring of blood glucose (SMBG) only provides glucose information only in a static way (akin to taking a snapshot) and not in a dynamic way (similar to a movie). 11 In daily practice, patients use CGM as a kind of “monitoring tool”, that is, they adjust their antidiabetic medication (most often the insulin dose) according to the current glucose value, the curve of the glucose values over the last hours, and the trend arrow which indicates how the glucose values will change in the near future.12,13
Currently, CGM systems are used by patients with T1D or T2D most often on a day-to-day basis and the recommendation is to use the systems all the time in order to achieve the optimal glycemic outcome. This recommendation is in accordance with the results of many clinical studies and respective meta-analyses.14-20 In clinical trials, patients were instructed to use their devices continuously and wear time of 80% appears to be the minimum lower limit required to see a clinical improvement.17,18,20,21 However, many of these studies also showed that it is difficult for a number of patients to wear the CGM system continuously. 22 In a study in France, the nonadherence rate (defined as a usage time of <70% of the time) was 13.9% in months 1-3, and 31.1% in months 4-6. 23 It appears as if many patients in daily practice use their rtCGM system “intermittently” and not constantly, and up to 40% of patients either stop using rtCGM altogether or at minimum reduce wear time considerably. Among new users, the early discontinuation rate was reported to be 25.4% during the observation period and the mean time to discontinuation was 339 days. 20 T1D Exchange Registry data show that in the United States the early discontinuation rate was 41% over the first year. 17 Many patients use rtCGM only during certain periods of time, although this probably varies depending on the systems used.17,19,20,24 One has to admit though, that most studies have been performed with today’s outdated models of sensors and devices, which might bias the results in view of modern CGM systems. Recently reported randomized controlled trials of traditional CGM, such as DIAMOND, 16 HypoDE (%), 25 and GOLD, 15 have required high levels of adherence for inclusion. On the other hand, Yu et al 26 presented studies, showing that despite the advances in CGM technology, better patient education, and support programs, the real-world adherence of CGM remains suboptimal with a considerable health-care resource waste.
Subsequently, the different aspects of intermittent use of CGM systems will be described, pointing out that CGM usage “in intervals” might be a common useful way of using CGM in cases or situations when the recommended, preferred method of constant use is not followed. One should therefore discuss if intermittent use of CGM systems might be of benefit for certain patient groups and/or situations/times. Intermittent use of CGM systems is probably not only reasonable but also an efficient and safe alternative to using it every day or never.
Up until now, only the Guideline of the Endocrine Society has recommended short-term, intermittent rtCGM use (but without providing a definition of intermittent use) in adult patients with T2D (not being on prandial insulin) who have glycated hemoglobin (HbA1c) levels ≥7% and are willing and able to use the device. 27 It appears that in no other guideline, to our knowledge, the intermittent use of rtCGM/isCGM is recommended or discussed.
Definition
So far, we have not found a definition of intermittent use of CGM in the literature. Therefore, we propose the following definition: intermittent use of CGM systems is any planned and agreed use that is intended not to be continuous all-the-time use for predefined periods of time or situations. The characteristic of “intention” or “planning” delimits this definition from a wearing behavior, which for various reasons deviates from the original agreement between physician and patient. To make the point clear, purely “forgetting” to scan regularly in isCGM or not replacing the glucose sensor at regular intervals with rtCGM is equivalent to nonadherence and is not in line with this definition. The proposed definition of intermittent use includes quantitative as well as qualitative aspects, which may overlap sometimes. The quantitative aspect includes, on the one hand, the duration of CGM use (eg, three days, one week, two weeks) and, on the other hand, the duration of the intervals until the next use (eg, monthly, every two months, twice a year, and annually). For example, a patient can use CGM for two weeks quarterly and in the time between these intervals use the SMBG system. The qualitative aspect includes specific events, situations, or occasions for the use of intermittent CGM. This may be diagnostic use at diabetes manifestation or for therapy intensification, use in special clinical situations, for example, during pregnancy, during hospitalization, but also in certain life events.
Reasons for Non-Continuous or Discontinuing Use of CGM
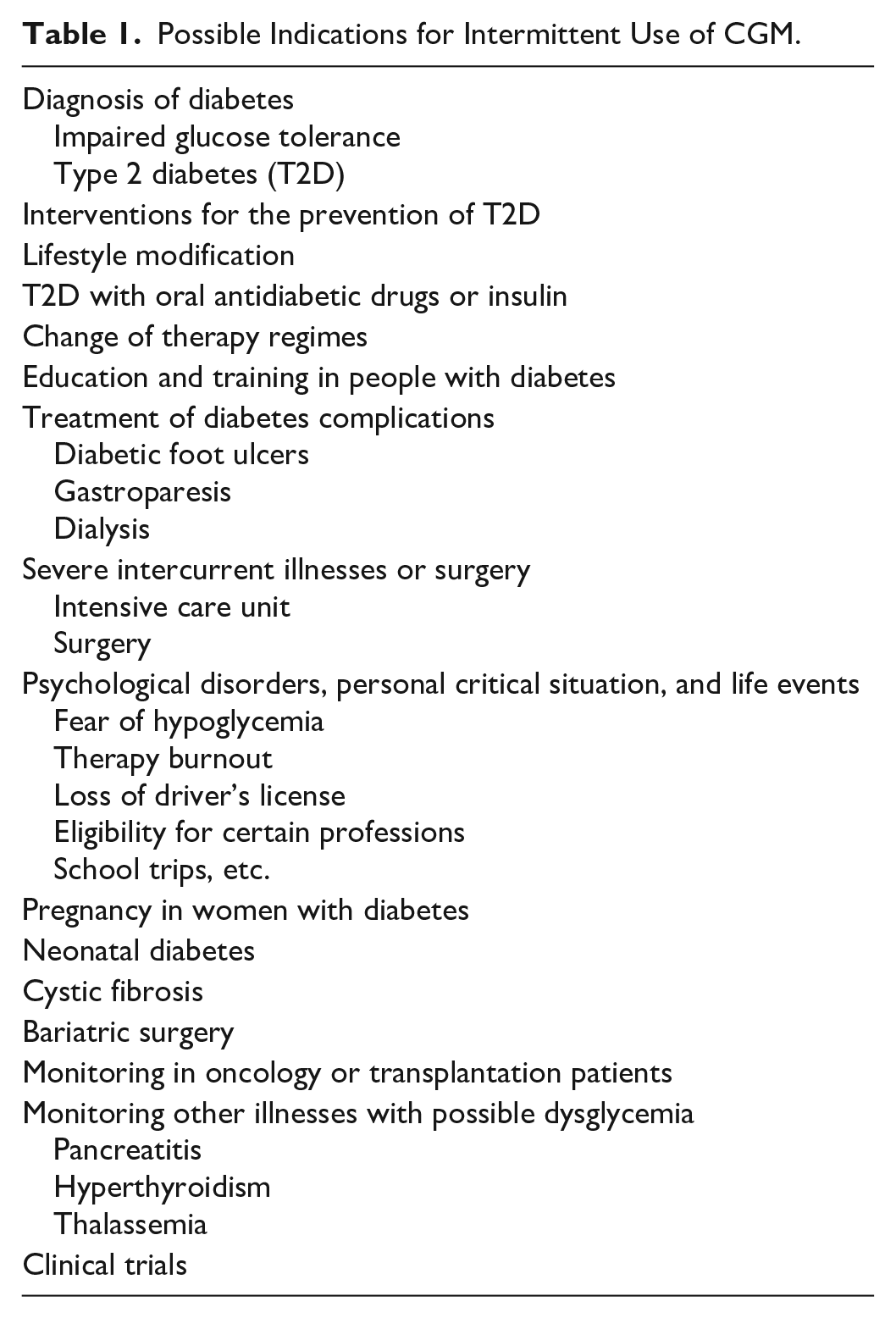
In general, there can be different situations and reasons for noncontinuous or discontinuing CGM use and one must distinguish between continuous monitoring using CGM and continuous use of CGM. CGM can be used with a clear intention for a relatively short period of time as a diagnostic tool before surgery or treatment escalation in a planned manner. Such usage can also be useful during different stages of the disease (eg, prediabetes), during complications or concurrent conditions, or in diseases not directly connected with diabetes (see below and Table 1).
Possible Indications for Intermittent Use of CGM.
Patient’s Perspective
An important reason for intermittent use of CGM systems might be that the patient may have false or unrealistic expectations of CGM, especially if the perceived disadvantages of the use of CGM outweigh the benefits.28-30 Some patients feel disappointment resulting from the fact that CGM use, in particular the alarms used on a daily basis, is experienced as disturbing or stressful.29,31 In addition, some patients experience themselves overwhelmed by the constant inflow of new information by the CGM system and the sheer amount of information provided (= data overload).30,31 They experience constant preoccupation with the values and perceive the frequent confrontation with diabetes as stressful. This occurs especially when there are, in addition, technical problems with the glucose sensors or skin irritations or in situations where CGM use is perceived as impractical.
Another reason for the intermittent use of CGM can be that the (cumbersome) usage of this diagnostic tool does not lead to the desired outcome, for example, an improvement in glycemic control.31,32 When the results of the therapy are not satisfying, constant feedback about the poor outcomes may be associated not as a spur to improvement but with negative feelings. 32 Also, negative reactions from the social environment, refuse to wear permanently technical devices on the body, skepticism of technology, or potential issues of data transparency can be reasons for the intermittent use of CGM.31,33 Likewise, patients may be convinced that they will receive sufficient information for their therapy with intermittent use. 34 Of course, cost also plays an important role in the decision of patients not to use CGM continuously. 35 One must accept that such issues are of high importance to many patients and greatly influence their decision about how often to use CGM.
Perspective of HCPs, Diabetes Teams
In order to use CGM correctly, patients must be motivated, trained, and supported in the evaluation and interpretation of the collected data. 11 Many factors play an important role in whether patients use CGM continuously, ranging from the attitude and expectations of the HCPs and diabetes teams to the experience in dealing with the technology and different devices. 36
Getting relevant, consolidated information from collected data and making appropriate therapeutic decisions within a short time frame can be a crucial barrier against the continuous use of CGM. In some cases, it can make sense to agree with the reasons patients have for not using CGM regularly, for example, if this is the patient’s wish or CGM is used for specific diagnostic or therapeutic decisions (eg, change of therapeutic regimes). Even for reasons of efficiency, it might often be useful to use CGM only at certain intervals if the results are sufficient for the assessment and adaptation of the therapy or the patient does not benefit from the alarms. There is also the possibility of using the so-called proCGM systems, where the patient cannot see the glucose data during the use of the device. The data are downloaded after a certain wear time. The proCGM systems can be used for multiple patients consecutively. One also must accept that patients and HCPs have different requirements and needs of CGM which might call for different types of CGM systems and ways of using them depending on the specific and individual problems, expectations, and requirements; this is also of relevance from the perspective of shared decision-making.
Perspective of Health Systems
CGM is still most often more expensive than SMBG making it a key reason why CGM has, to date, been used by relatively few patients in comparison to the total number of potential users worldwide. In a recently published Health Technology Assessment report, the authors stated that the high cost of CGM systems was seen as the greatest barrier to their widespread use. 37 To date, compelling cost-effectiveness studies for different groups of people with diabetes with various problems or health statuses are lacking. 35 Budget impact analyses are an important prerequisite for the assumption of cost calculations from the perspective of the healthcare payer. It is obvious that intermittent CGM use has a cost advantage and for countries with a tight budget for diabetes, it can be a very sensible strategy. 26 The relevance of this aspect differs massively depending on the individual situation of the patient and the resources that must be taken into account (reimbursement, self-payer). A study of medical resource usage while employing CGM systems showed that the group of patients using CGM demanded less often medical consultation (eg, by phone) in comparison to patients not using CGM.38,39 It remains to be studied if repetitive intermittent or noncontinuous use of CGM leads to the sustainable improvement of medical, psychosocial, or patient-reported outcomes and whether it is cost-effective.
Possible Situations/Indications for Intermittent CGM Usage
Categorization of possible indications and clinical situations for intermittent CGM usage is challenging. The section below lists diabetes-related causes in prediabetes, T1D or T2D, or other illnesses affecting glucose metabolism. If deemed helpful, sensible, and meaningful, we have included the reasons behind it, its advantages, and the existing evidence. Although we have not done a systematic literature search, often there is no clear evidence one way or the other. This list is by no means complete. It should merely serve as a proposition for discussion.
Diagnosis of Diabetes
Intermittent CGM could be used to diagnose diabetes or to define new criteria for the diagnosis of impaired glucose tolerance (IGT) or T2D besides using standard diagnostic criteria like fasting plasma glucose (FPG) or HbA1c. Recently, the working group of Colas et al showed that CGM allows for a better T2D risk prediction than FPG and HbA1c in a high-risk population. 40 Interestingly, the authors found that CGM-derived phenotyping reveals clinical differences which were not revealed by conventional diagnostic criteria. Also, Rodriguez-Segade et al have shown that the use of CGM can better detect dysglycemia in persons without diabetes. 41 In one study, CGM was used to identify children at risk for T1D as well. 42 In these cases, short-term use or intermittent use of CGM can be meaningful and makes a good diagnostic tool.
Interventions for the Prevention of T2D
Short-term use of CGM has also been used for improving exercise adherence in a group of subjects with IGT. In addition, and although there are very few published results so far, initial studies show that CGM can be used successfully for behavior modification in prediabetes to overt T2D.6,43 It may be useful to provide continuous and immediate feedback about the consequences of food and activity choices on glucose levels for people with a high risk for T2D. Intermittent use of CGM has the potential to enhance behavior change and problem-solving by providing physiological feedback. However, the future importance of intermittent use of CGM in the prevention of T2D and the potential role as an adjunct to lifestyle changes calls for further evaluation.
Lifestyle Modification
Initial results are very promising on the intermittent use of CGM for lifestyle modification and behavioral counseling for patients with T2D not requiring insulin. In a systematic review with 11 studies and a total 5542 patients, Taylor et al reported that, compared with SMBG, intermittent use of CGM promoted greater reductions in HbA1c, body weight, and caloric intake. 7 They also observed a higher adherence to a personal eating plan, increase in physical activity, and high adherence to CGM wear time and device calibration. The intermittent use of CGM enables an individual to observe what kinds of foods elevate his glucose level and to understand better the interactions and impact between diet, physical activity, and medication choices with greater qualitative and quantitative feedback. The intermittent use of CGM in lifestyle modification interventions in people without diabetes is also conceivable.
T2D with Oral Antidiabetic Drugs or Insulin
Intermittent use of CGM can also be recommended for poorly controlled patients with T2D treated with oral antidiabetic drugs (OAD) or insulin. Yoh et al demonstrated that intermittent use of CGM was beneficial in modifying a patient’s diet and exercise habits and thereby significantly reducing body weight, body mass index, postprandial glucose level, and HbA1c after three months. 44 Erhard also reported reduced HbA1c levels in patients stopping CGM use prematurely. 45 In a randomized controlled study, Vigersky et al came to the conclusion that patients with T2D not on prandial insulin who used rtCGM intermittently for 12 weeks significantly improved glycemic control at 12 weeks and sustained the improvement without rtCGM during the 40-week follow-up period, compared with those who used only SMBG. 46 The Endocrine Society Clinical Practice Guideline also recommends intermittent rtCGM use in adult patients with T2D (not on prandial insulin) who have HbA1c levels ≥7% and are willing and able to use the device. 27
Change of Therapy Regimes
CGM can be used short term or intermittently to adjust or change diabetes therapy as is routinely done in all patients with continuous CGM. This can either involve a change of doses or a change to the therapy regime, for example, change from oral medication to insulin use. One could argue that with the different quality of glucose data available, a decision regarding the change in treatment would be more evidence based and the effect could be rechecked at a later time using CGM. This could avoid clinical inertia, meaning the lack of initiating necessary treatment changes.
Education and Training in People with Diabetes
The influence of different types of meals, exercise, or daily routine on glycemic variability is often difficult to assess for people with diabetes, T1D and T2D alike. Intermittent use of CGM combined with a structured education program could increase understanding, knowledge, and problem-solving of glycemic fluctuations in different situations and therefore improve the glycemic outcome. Different studies already show possible scenarios and uses in this regard, and further studies should be initiated, especially in patient groups, with difficulties achieving treatment goals, such as adolescents.43,47,48
The special situation of hypoglycemia unawareness would benefit significantly from the use of CGM for a certain time as it could improve the perception of hypoglycemia in persons who do not want to wear CGM continuously as a safeguard.49-51
Treatment of Diabetes Complications
The rate of wound healing has been shown to be linked to the height of the glycemic level as measured by HbA1c52-54 as hyperglycemia is associated with impaired wound healing. 55 Because HbA1c levels are always a retrospective marker for the glucose concentration, one could derive from this that establishing a tighter glycemic control by using CGM data during treatment of diabetic foot ulcers could be of great advantage.
People with diabetes undergoing dialysis experience both pronounced glycemic variability and hypoglycemic events depending on the days on/off dialysis. Using intermittent CGM, glucose levels of these patients could be monitored more intensively, and therapeutic strategies and appropriate medication dosing could be established to reduce these incidences, as has already been shown.56-58
The diagnosis and treatment of gastroparesis as a common complication of diabetes with high fluctuation of glucose values (especially postprandially) can also be improved with the use of intermittent CGM. Patients and diabetes teams can learn from the trends and course of the glucose profiles over time as provided by the CGM systems to adjust their eating habits and adaption of their medication.59,60
Severe Intercurrent Illnesses or Any Medical Therapies Aggravating Glucose Control, For Example, Surgery or Critically Ill Patients in the Intensive Care Unit
For any person with diabetes, T1D or T2D alike, intercurrent illnesses, especially serious ones, and surgery represent are a serious challenge when it comes to keeping glucose under control. This holds also true for HCPs, diabetes teams, and nursing staff in hospital settings. The care of patients with diabetes during and after surgery with the right adaption of medication therapy is demanding and the fluctuations of glucose values can be immense. It has been shown that close-to-normal glucose levels are beneficial to the course of recovery, the surgical result, and wound healing. Among patients in the intensive care unit, pre/postsurgery or critically-ill patients (eg, acute stroke or ischemic stroke), dysglycemia is common and associated with increased complications; this also applies to patients without diabetes. Therefore, it seems obvious that in these conditions, intermittent CGM before, during, and after surgery or serious illnesses could improve both the outcome and the treatment of diabetes.61-67
Psychological Disorders, Personal Critical Situation, and Life Events
Fear of hypoglycemia is a strong driver for not achieving glycemic goals.30,33 Although continuous use of CGM would be the right choice, in this case, to avoid such events as much as possible, not all people with diabetes are capable of making the right choice. Here, intermittent CGM could be of help in identifying times and situations of possible hypoglycemia, giving the advice to manage such situations, assuring the patients and using CGM as a teaching tool. Also, in periods of therapy burnout and the overwhelming burden of glycemic control, intermittent use of CGM for a limited time period or repeatedly can be an alternative.16,23,68 Loss of the driver’s license due to recurrent hypoglycemia is a serious life event for any person with diabetes. Using CGM for a certain time to improve glucose control, reduce the risk of hypoglycemic events, and then to document the achievement can be of great benefit and sometimes the only way to regain the driver’s license if continuous use of CGM is not possible for any reason. Similarly, it could be helpful using CGM intermittently to demonstrate the ability or eligibility for certain professions or jobs (here again, the avoidance of recurrent or severe hypoglycemia). A multitude of circumstances come to mind where good glycemic control would be essential but SMBG is not adequate or sufficient, for example, exams, special training sessions, school trips, or summer camps for children where remote monitoring by the parents would be favorable.
Pregnancy in Women with Diabetes
Growing evidence shows the positive effects of CGM usage in pregnant women with existing diabetes.5,69-76 CGM provides more detailed information about glycemic variability and stability throughout pregnancy and is also helpful for adjusting diabetes therapy, especially because insulin requirements can sometimes change dramatically during pregnancy and then labor CGM usage also improves the neonatal outcome of pregnancy complicated by diabetes, like reducing macrosomia in the newborn. 5 Even use of CGM for short, repeated periods of time during pregnancy showed a positive effect.70,77
A similar situation, although with different relevance and characteristics, is gestational diabetes (GDM). CGM usage helps to detect a higher proportion of women with GDM needing antihyperglycemic medication compared with SMBG, reduces gestational weight gain, and can help to educate women with GDM.78-81 Therefore, using CGM during pregnancy in women with diabetes is an important indication, which might be, regarding the life of the woman with diabetes, intermittent use only during her pregnancy.
Neonatal Diabetes
Another group of patients benefiting from intermittent CGM usage are neonates or preterm infants, with or without (neonatal) diabetes, as CGM is a safe and suitable method to monitor glucose levels in neonates.82,83 Especially in neonatal diabetes with high glucose fluctuations and high insulin sensitivity, the need for minimally invasive glucose measurements is obvious. This also helps in finding the best therapeutic modalities. 84 In (critically-ill) preterm babies, the high variability of glucose levels and an increased risk of hypoglycemic events are a known complication which can be detected earlier and more often with CGM compared with the use of episodic glucose measurements.85-87 Although these advantages exist and glucose therapy and feeding can be better adjusted during the first weeks of life, studies or results on improved clinical outcome are still pending. 86
Cystic Fibrosis
Other specific types of diabetes, for example, in cystic fibrosis (CF) or other diseases of the exocrine pancreas, endocrinopathies or drug-induced or chemical-induced diabetes can also be indications for intermittent use of CGM. Here the question is to find the optimal point in time during routine screening to initiate or escalate diabetes-specific therapy. For example, clinical symptoms of diabetes, which is present in 20%-50% of youths/adults with CF, typically progress slowly and sometimes insidious, and glucose abnormalities cannot be detected sufficiently with diagnostic measures like an oral glucose tolerance test.88-92 It has also been shown in youth that high glycemic excursions correlate with a decline of lung function. 93 CGM-guided insulin therapy is associated with improved clinical outcomes as weight gain and pulmonary parameters. 94 The intermittent use of CGM has therefore potential to be meaningful and beneficial in improving the treatment of patients with CF.
Bariatric Surgery
One common negative outcome after bariatric surgery is late postprandial hypoglycemia. To evaluate this condition, educating patients and to adjusting diet and treatment postsurgery intermittent CGM use has been shown to be effective.95-98 Another reason for intermittent use of CGM after bariatric surgery can be the prediction of diabetes remission. 99
Monitoring Oncology or Transplantation Patients
In patients (with or without pre-existing diabetes) with different malignant diseases or on oncologic therapies, for example, in prostate carcinoma during androgen-deprivation therapy, insulin resistance and hyperglycemia increase, dumping syndrome after gastrectomy for gastric cancer, hypoglycemia, or hyperglycemia can be threatening complications.100-106 This could be monitored well with intermittent CGM after tumor resection or at the start of specific therapy, transplantation, or during follow-up care. Other cases have been described which show the benefit of intermittent CGM use, for example, for a patient with a neuroendocrine tumor suffering from high glycemic fluctuations and recurrent hypoglycemia. 107
Monitoring Other Illnesses with Possible Dysglycemia
During chronic pancreatitis, or after pancreatectomy in the immediate postoperative follow-up period, and screening during the long-term care monitoring, using CGM for the screening of hyperglycemia can be useful.108,109 Pancreatogenic diabetes is characterized by recurrent severe hypoglycemia due to changes in or loss of endocrine functions, resulting in “brittle” diabetes and often severe hypoglycemia. 110
Hyperthyroidism (Graves’ disease) can also be accompanied by IGT which results in a disbalance of glucose metabolism for reasons which are not always clear. Intermittent CGM use could be helpful in evaluating the glucose fluctuations.
CGM has also been suggested to be useful for the diagnosis of glycemic abnormalities in adolescents with thalassemia. 111
Clinical Trials
An excellent application for using intermittent CGM are clinical trials, as CGM and its parameters are now regarded as mandatory to document clinical results, for example, time in range, hypoglycemia, coefficient of variation, and the interpretation of such parameters.112-114
Conclusions or What Is the Rationale for Intermittent CGM Use?
Due to the characteristics of CGM, in the discussion about its application, it was usually tacitly assumed that it would also be applied continuously. What has been missing so far is a definition of intermittent use of CGM and a discussion about different fields of application or special situations, causes and reasons, and where and why this could be deemed appropriate. From our point of view, the discussion about this type of use of CGM should be conducted not only under the perspective of nonadherence but more about patient wishes, different medical conditions, economic constraints, etc. There are many serious reasons and occasions that speak for discontinuous CGM use. Nevertheless, of course, the patient’s wish must be respected if he or she does not want to wear a CGM device continuously. Whenever CGM is planned to be used only for a limited period of time for diagnostics, therapy monitoring, or as a basis for a therapy decision, the intermittent application is already considered the standard today. In addition, many new applications for CGM, such as the prevention of T2D, are conceivable where the intermittent use of CGM as an adjunctive therapy certainly makes sense. The use of CGM for a limited time is also conceivable outside the indication of diabetes, such as for lifestyle intervention measures.
Up to now, to our knowledge, there are too few studies being conducted to evaluate the efficacy and efficiency of intermittent vs continuous use of CGM and to evaluate what the minimal optimal time of use should be to result in an improved outcome.
Given the financial burden on health-care systems and the patients themselves in certain countries, we regard intermittent use of CGM over a long period of time to be more the norm than the exception. In weighing the costs and benefits the CGM’s balance sheet seems to be particularly good if CGM is used temporarily in patients with a particularly high risk of diabetes acute complications (eg, severe hypoglycemia, diabetic ketoacidosis, surgery), in special risk populations (eg, neonatal diabetes, cystic fibrosis), or as a support for important therapy decisions and to monitor glycemic control in situations where diabetes is only a secondary diagnosis.
Intermittent use of CGM should be discussed openly and in a wider manner and this option for glucose monitoring holds promise for a broad spectrum of situations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RZ has received speaker’s honoraria and/or served on advisory boards from/of Abbott, Ascensia, AstraZeneca, Berlin Chemie, Dexcom, Lilly, Novo Nordisk, and Roche Diabetes Care.
LH is a consultant for a number of companies that develop novel diagnostic and therapeutic options for diabetes treatment; for example, Roche Diabetes Care, Becton Dickinson, Lifecare, Berlin-Chemie. LH is shareholder of the Profil Institut für Stoffwechselforschung, Neuss, Germany and ProSciento, San Diego, United States.
GF is general manager of the IDT (Institut für Diabetes-Technologie Forschungs- und Entwicklungsgesellschaft mbH an der Universität Ulm, Ulm, Germany), which carries out clinical studies on the evaluation of BG meters and medical devices for diabetes therapy on its own initiative and on behalf of various companies. GF/IDT have received speakers’ honoraria or consulting fees from Abbott, Ascensia, Dexcom, LifeScan, Menarini Diagnostics, Metronom Health, Novo Nordisk, PharmaSense, Roche, Sanofi, Sensile, and Ypsomed.
RH is an employee of Roche Diabetes Care.
BK has received speaker’s honoraria and/or research grants from Roche Diabetes Care, Abbott, Ascencia, Berlin Chemie, Novo Nordisk, MSD, Lilly Deutschland, Sanofi.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funds were made available by Roche Diabetes Care.