
Abstract
Background:
Wearables (= wearable computer) enable continuous and noninvasive monitoring of a range of vital signs. Mobile and cost-effective devices, combined with powerful data analysis tools, open new dimensions in assessing body functions (“digital biomarkers”).
Methods:
To answer the question whether wearables are ready for use in the medical context, a PubMed literature search and analysis for their clinical-scientific use using publications from the years 2008 to 2018 was performed.
Results:
A total of 79 out of 314 search hits were publications on clinical trials with wearables, of which 16 were randomized controlled trials. Motion sensors were most frequently used to measure defined movements, movement disorders, or general physical activity. Approximately 20% of the studies used sensors to detect cardiovascular parameters. As for the sensor location, the wrist was chosen in most studies (22.8%).
Conclusion:
Wearables can be used in a precisely defined medical context, when taking into account complex influencing factors.
Introduction
Vital parameters such as heart rate, blood pressure, oxygen saturation, and temperature are essential for the clinical evaluation of patients. With new technological developments, such vital parameters can be recorded wirelessly and continuously, noninvasively and cost-effectively using the so-called wearables. The combination of wearables with powerful data analysis tools opens up new dimensions in the assessability of body functions (“digital biomarkers”), with the possibility of remote monitoring further enhancing the relevance of such approaches. Although many of the technologies used in wearables are not really innovative, technological advances mean that they can now be integrated into portable battery-operated devices in a compact and cost-effective form. They make it possible to use them in patients’ everyday lives and allow important functional aspects to be quantified and qualified, such as physical activity and sleep behavior.
The aim of this review is to present the status quo of the application of wearables for the measurement of vital parameters in the medical context. Additionally, the results of a PubMed search about clinical trials with wearables will be presented.
Background
Nowadays, many healthy people also monitor their vital parameters independently and regularly, but no published data on the number of vital parameters in Germany are yet available. In relation to the total population, it can be assumed that this proportion is relatively small. However, the proportion of those who collect information about their body functions under everyday conditions through wearables, driven by the “Quantified Self” movement, is increasing significantly. 1 Smartphones now routinely record a number of parameters and provide the user with suitable evaluations.
To date, vital parameters have primarily been recorded analogously in the medical context, eg, by blood pressure protocols or movement protocols for Parkinson’s patients. These are used by the attending physicians as “orientation” and usually not systematically evaluated. The keeping of such protocols means a high additional effort for patients, which often results in only inconsistent protocol keeping.
At the outpatient care level, vital parameters are usually randomly collected because of the limitations of analog measurement methods and the lack of data storage. The established methods for continuous recording of vital parameters under everyday conditions (eg, long-term ECG or blood pressure measurements) are carried out over a comparatively short period of a maximum of a few days.
On an inpatient level, a set of vital parameters is routinely recorded by hospital staff at several points in time per day; this is a manual serial measurement with different recording frequencies. There are no published data available on the regularity and measurement quality of vital parameters in hospitals, although there are corresponding guidelines from the specialist societies. 2 Although various vital parameters are continuously recorded on monitoring stations, they are usually only analyzed as “snapshots” or in simple trend tables. In addition, many of the parameters need to be measured invasively and are associated with considerable restrictions on patient mobility. A transferability of the vital parameters measured under inpatient conditions to the everyday situation of the patients is only possible to a limited extent.
Overall, the recording of vital parameters currently requires considerable personnel and economic effort; it is often unclear to what extent the information obtained is reliable and what actual medical added value it offers.
Monitoring of Vital Signs With Wearables in the Medical Field
The rapidly increasing number of different wearables is primarily based on their use in the private sector (eg, fitness tracking); for medical use, there is only a limited number of systems. 3 The recording of various vital parameters measurable with wearables should enable a clinically relevant assessment of intra- and interindividual physiological and pathophysiological processes over time. They are to be used for monitoring vital parameters in outpatient, inpatient, institutionalized (eg, nursing home), and scientific settings.
Medical interventions based on vital parameters recorded with wearables require high data reliability, ie, the measured parameters must be validated in a precisely defined context of use (eg, age and pre-existing conditions). 4 Despite the rapid technical development, this validation still turns out to be a complex requirement; a number of influencing factors have to be considered systematically and structured before the use of wearables (Figure 1):
Environmental factors: Ambient light, temperature, humidity, height above sea level, and the exact location of the patient must be taken into account. 5
Legal framework conditions: The medical purpose (diagnostic or therapeutic) of wearables crosses the line from lifestyle/fitness to medical devices, so that manufacturers and users in Europe are subject to the Medical Devices Act (MPG) and the (medical) product used must be CE-certified. In Europe, the regulatory authorities have so far not made any recommendations for the use of wearables in the medical context; in the United States, on the other hand, they have done so for clinical application, albeit not for use in clinical research. There are only a few initial statements on this subject.6,7
Body: The target population should be clearly defined and has to be carefully considered which parameters are relevant in the given disease-related context. The majority of the clinical studies identified with the PubMed research mentioned above were conducted with a young and healthy study population. Such volunteers differ considerably from the patients in the medical use of wearables and represent an inadequate starting point. Even when wearables are used in an adequate target population, pronounced interindividual differences must be taken into account: Thus, factors of body constitution such as skin color, fluid status, and body fat content can vary significantly between patients in a target population. Especially in photometric procedures (eg, photoplethysmography [PPG]), body temperature has a negative influence on the measurement quality via local skin perfusion or substances applied or applied to the skin (eg, creams and tattoos). 5
Movements cause artifacts in many measurement methods and are one of the biggest problems in data evaluation. For example, heart rate analysis has shown that measurement accuracy decreases with increasing movement intensity. 8 Furthermore, the heart rhythm can influence the accuracy of the measurement, so that the heart rate can be determined more reliably in patients with sinus rhythm than in patients with atrial fibrillation. 9 Therefore, influential disturbances such as movements should be addressed and compensated for as well as possible.
Sensors: The sensors built into wearables usually convert a physiological signal into an electrical signal, which is then usually digitized and stored or transmitted in this form. In most wearables, combinations of different sensors are used. Many of the measurement methods are not based on traceable measurement quantities in the metrological sense, they are measured with arbitrary methods (ie, without calibration). This means, for example, in the case of PPG that the light measured by the photon detector is usually not specified with an SI unit. However, since the absolute measured values are in most cases not clinically relevant, but relative changes, interindividually comparable values only result after further processing (eg, determination of the heart rate from pulse wave analysis).
The attachment of the sensors to the body can have a negative influence on the quality of the measurement of some parameters, eg, the accuracy of the pulse measurement at the wrist is inferior to that at other locations. 10 The ear, for example, represents a low artifact measuring point for many parameters. The reasons for this are the lack of ambient light in photometric measurements in the auditory canal and comparatively few movement artifacts. 11 It nonetheless remains to be seen how compliance with in-ear wearables will be in clinical studies.
Depending on the body localization at which the wearable is to be measured, different fixation techniques are considered, eg, with a plaster or an elastic band. The contact pressure can influence the local blood flow in such a way that the quality of the measurement is negatively affected. 12 If the wearable is worn in the same place for a longer period of time, skin reactions may occur which may even lead to the development of relevant inflammations. Such side effects can massively impair the use of wearables by patients.
Processor: The wearables in themselves often represent a “black box,” ie, the raw signal detected by the sensors is processed by proprietary algorithms of the manufacturers; artifacts created shall be eliminated, the signal-to-noise ratio shall be improved, etc. The algorithms are usually permanently further developed, since an improvement in the performance of the wearables is possible without major technical effort (in terms of hardware). Therefore, the most current algorithm version should always be used for practical application and the version used should be documented.
In everyday use, user-friendliness and intuitive handling of wearables are decisive factors for long-term use by patients. Factors such as battery life, capacity of the data memory, and easy attachment to the body are of great importance in this context. Such characteristics vary significantly between the available wearables which means the spectrum of battery life goes from a few hours up to 18 months (Spire Health Tag, Spire Inc., United States).
Data transfer: The processed data are not only stored in different formats (ISHNE, CSV, etc.), but depending on the underlying operating system, relevant differences may arise for further data transmission and processing. If the data from wearables are to be merged with data from other signal sources, the necessary interoperability is often not given. The integration of wearable data into the existing clinical information systems (CIS) or practice systems can thus be made considerably more difficult. There are individual technical solutions in which vital parameters are automatically transferred into such information systems (Connex Spot Monitor, Welch Allyn Inc., United States; No Wearable), but as a rule this possibility does not exist for vital parameters recorded with wearables.
Vital sign data can be transferred from the given wearable to a device via Bluetooth or similar methods using different transmission techniques. In practice, the transmission technique used has a considerable effect on the reliability of the transmission per se and on the transmission speed. In many cases, the wearables are linked to a smartphone and the data are automatically stored in cloud databases. There are studies that have shown that the data transmission of medical devices using such techniques is not sufficiently secure. 13 Even the act of data transmission as such must be covered by the express consent of the patient previously informed of his rights. In the European Union, this is controlled by the General Data Protection Regulation and in Germany by the Federal Data Protection Act.
Devices: These devices receive the data and represent the interface to the user. The vital parameters are visualized on the display of the devices: this ranges from the representation of a numerical value to complex graphics, eg, for glucose day profiles. It is crucial for the user to be able to get a comprehensive picture of the data immediately. Furthermore, key figures can be calculated and displayed in the terminal device: for example, the average glucose concentration, sleep duration, or heart rate.
Analysis and interpretation: The progress made in data processing and analysis in recent years as well as over the past decades due to the broad availability of smartphones has made a decisive contribution to the pronounced use of wearables in the private sphere. The amount of data to be analyzed is considerable, if, for example, a range of vital parameters with a frequency of, eg, 1 Hz (per parameter 86 400 data records/day) is recorded, several million values result over weeks, months, and years. In most clinical studies with wearables, data processing was “manual”, ie, with the help of suitable software (such as Matlab). With methods from the field of artificial intelligence and “deep learning,” a considerably faster and “automated” processing is possible. An increasing use of such approaches in data processing in connection with vital parameters can be observed, however, these methods have so far only been used in smaller experimental investigations.
The potential of new evaluation methods for large amounts of data (ie, “Big Data”) can hardly be overestimated. 14 It is, however, important to consider the benefits in a differentiated way, as it is possible, with the help of artificial intelligence, to differentiate images of the fundus of the eye according to gender without it being comprehensible on the basis of which criteria the algorithm used makes this allocation. 15 As a result, this circumstance is per se goal-oriented, but unsatisfactory in terms of knowledge gain; similar problematic results are also conceivable in the area of vital parameters.
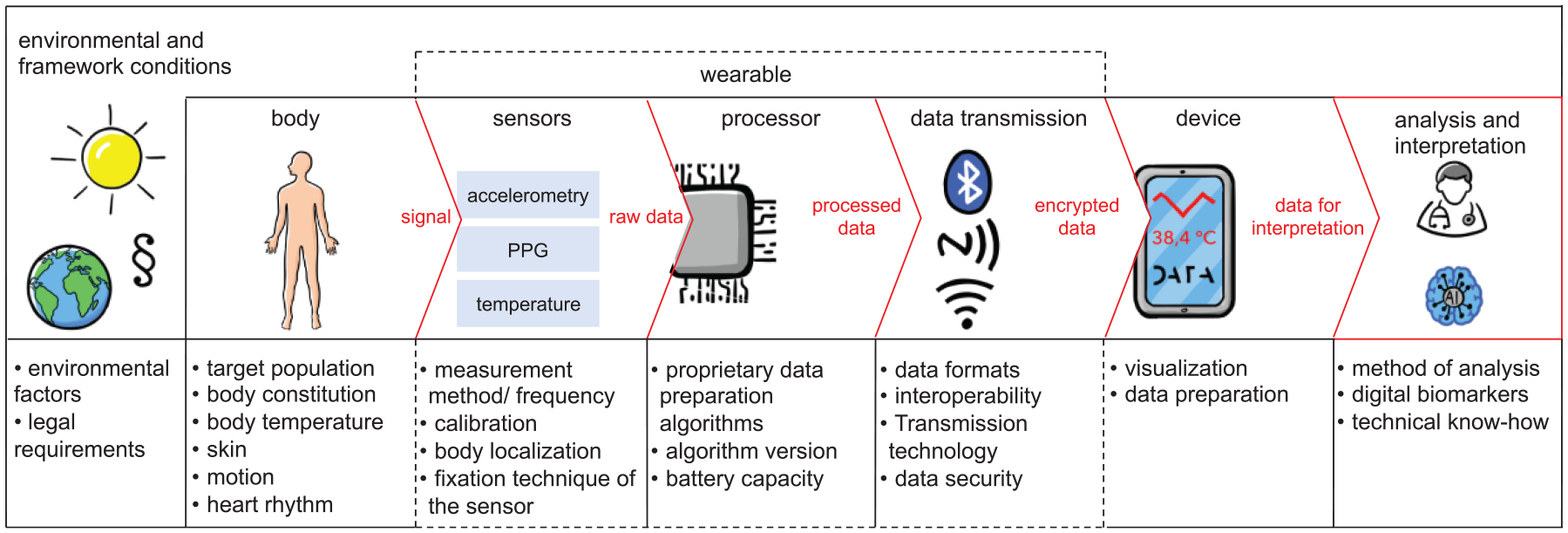
Noninvasive continuous measurement of vital parameters with wearables. Steps from the signals to the analysis and interpretation of the measured values. PPG, photoplethysmography. Source: Graphs from www.visionom.de.
This list of factors makes it clear that there are no wearables that can be used ubiquitously (“one fits all”), but that the specific selection of a suitable wearable must be made for the respective question.
Self-Monitoring by the Patients
The measurement of vital parameters can support patients especially in dealing with diseases of civilization such as obesity-related, neurodegenerative, and cardiovascular diseases. Self-monitoring enables patients to continuously track their own physical condition based on objective data in everyday life at any time. Such vital parameters recorded under everyday conditions support approaches to individualized medicine. Defined key figures (ie, digital biomarkers) can be determined through the evaluation of longitudinally recorded “vital parameter profiles”; their value can be further increased through the use of further information (eg, genomics). 16
A possible negative consequence of self-monitoring is that hypochondriasis may worsen and patients are constantly concerned with their vital parameters and the possible significance of these parameters on their health. The American “mobile health” expert Eric Topol sees the predominant benefit of digital medicine in the larger context, but also points to the problem of such “side effects. 17 ”
Usage of Wearables in Research and Clinic
The clinical studies to date provide indications of the potential of the use of wearables for clinical research. Thus, wearables provide important additional information for the interpretation of the questions posed by the studies (“surrogate parameters”). The combination of noninvasively recorded vital parameters with subjective patient experiences (electronic patient reported outcomes, ePRO) under real conditions represents a further option for clinical research. Such correlated data could be used ubiquitously in healthcare: From clinical research to outpatient care to inpatient monitoring, practitioners are de facto “live” informed about serious incidents and changes in the monitored patients.
In the Apple Heart Study, data from approximately 420 000 study participants were analyzed for cardiac arrhythmias using Apple Watch (a photoplethysmographic method) and immediate automated analysis. Recruitment for the study was via an app (“ResearchKit”), with the first >10 000 study participants enrolling within 24 hours. 18 Whether clinical studies with wearables with large study cohorts (ie, “virtual studies”) will be conducted more frequently in the future and how principles of Good Clinical Practice will be implemented in such studies remains to be seen.
The “dynamic” life cycle of wearables and their software represents a considerable obstacle to the use of wearables in research: Software updates come in monthly intervals and new device generations in annual intervals. A context-related validation for a vital parameter only applies to a defined wearable generation with a given software version. With regard to a study duration that regularly takes years, this problem must be adequately considered: A wearable that was selected during study planning may differ significantly in its properties from the wearable that is used at the start of the study and, above all, at the end of the study.
The use of wearables in hospitals enables a completely new monitoring option, the diverse application potential of which has not yet been fully exploited.
Possible use cases are the following:
New procedures for the collection of vital signs. After appropriate validation, wearables can be used to replace the previously used methods for vital signs collection. For a broad use of wearables in the medical environment, it would be supportive if they could measure two additional vital signs: - Noninvasive and cuff-less real-time blood pressure measurement: In various approaches, PPG is mostly used in combination with ECG recording.
19
A clinical trial from 2016 showed that such a measurement of systolic blood pressure is possible; it even meets the requirements of the Society for Measurement Accuracy for new blood pressure monitors.
20
Since the end of 2018, the first wristwatch wearable for measuring blood pressure has had FDA approval, which measures blood pressure noninvasively several times a day.
21
- Noninvasive continuous blood glucose measurement as a replacement for conventional capillary blood glucose measurement and continuous interstitial glucose monitoring, which is still a burdening factor for millions of patients with diabetes. Although various approaches have been researched in recent decades, no marketable product is yet available.22,23
Outpatient/inpatient monitoring of patients during critical treatment phases: The automated analysis of vital signs for the collection of clinical scores is an important application example, eg, the “Early Warning Score” or the “quick Sepsis-related organ failure assessment” (qSOFA) score. Such scores are clinical tools that take vital parameters and state of consciousness into account and allow early detection of disease worsening or sepsis. 24 Through consistent further development of such scores, clinically relevant events can be automatically detected by wearables.
Treatment support for chronic diseases or for therapies involving a high risk that lead to frequent hospitalization: An example is the assessment of volume status on the basis of vital signs in patients with heart failure. In addition, the potential of novel therapies can be better detected by wearables, eg, by the option of monitoring for specific undesired side effects, such as those occurring with CAR-T cell or antibody therapies in the form of cytokine release syndrome. 25
Secondary prevention: One example is the early detection of heart rhythm disorders in large collectives of previously healthy patients. As with all screening examinations, a careful balance must be struck between the expected incidence and the false-positive rates.
Health-Economic Aspects
The direct costs or acquisition costs for wearables are comparatively low compared to other medical equipment. If, however, clinical validation studies are required for the use of wearables in accordance with the MPG, it can be assumed that the manufacturers will pass on the costs incurred to users in the form of higher acquisition costs.
Due to the abnormalities in the vital parameters of patients detected by wearables, there may initially be increased use of medical services, ie, the health systems have to bear higher costs. 26 In the long run, costs can be reduced by avoiding hospitalization and achieving a better state of health. 27 Overall, it is not yet possible to estimate whether wearables have a positive cost-benefit ratio.
Methods
To describe the status quo, a PubMed literature search was carried out and publications on clinical studies with wearables in the last 10 years were sought. The search terms “wearable” and “clinical trial” or “clinical study” were used in the years 2008 to 2018 (accessed February 20, 2019).
Results
The search yielded 314 hits, with the number of hits increasing from n = 4 in 2008 to n = 84 in 2017 and n = 49 in 2018. The identified articles were then analyzed to determine whether they described the results of clinical studies with wearables for the noninvasive measurement of vital parameters. This applied to n = 79 (of which n = 16 were randomized controlled trials) of the 314 publications. Relevant data from these 79 publications were collected and evaluated (Table 1; the respective references are given in the last column of the table).
In PubMed Literature Research Identified Clinical Studies Published in the Years 2008-2018 in Which a Noninvasive Continuous Measurement of Vital Parameters With Wearables Was Performed.
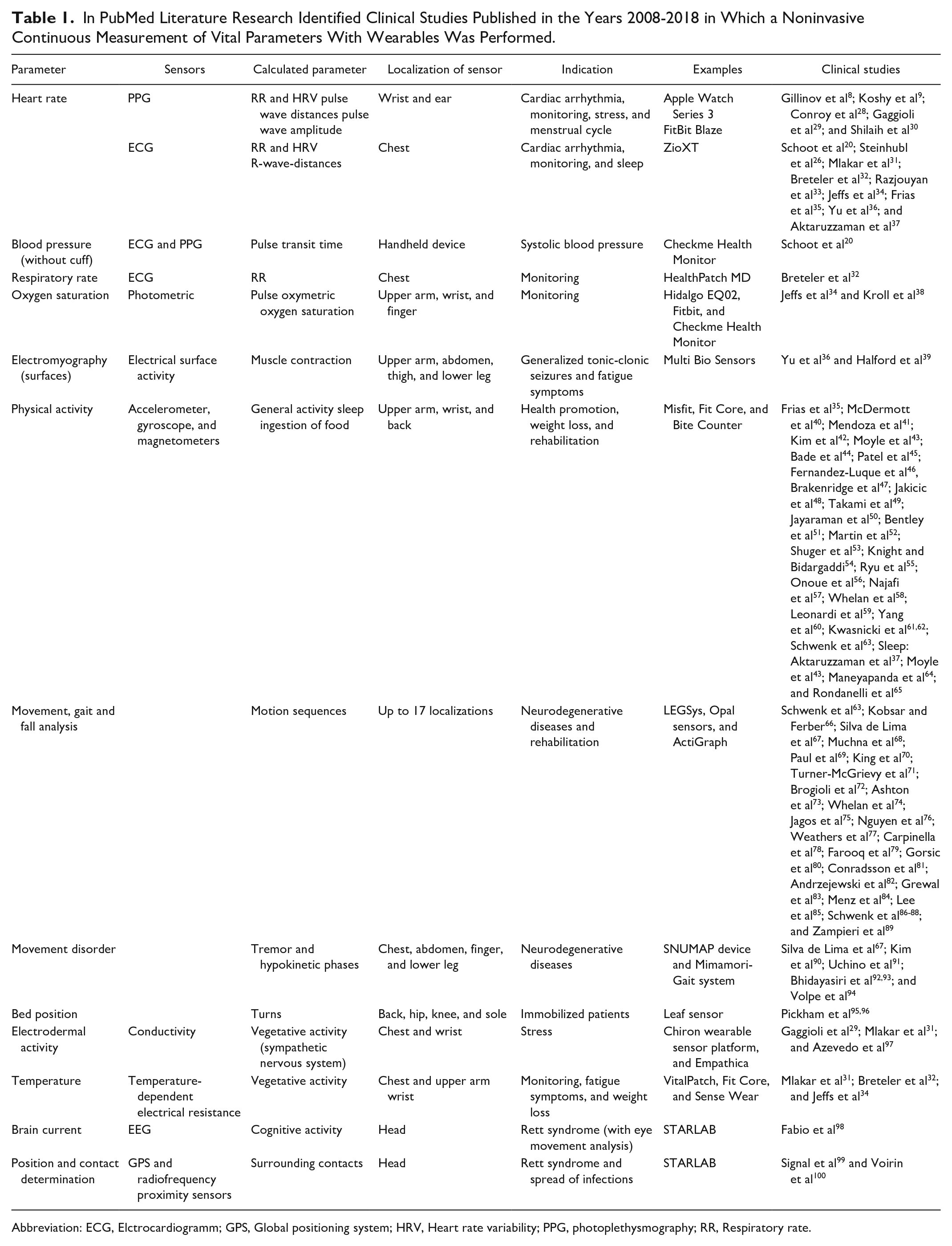
Abbreviation: ECG, Elctrocardiogramm; GPS, Global positioning system; HRV, Heart rate variability; PPG, photoplethysmography; RR, Respiratory rate.
Parameter and Sensors
In 60% of the studies, sensors were used that can measure linear (accelerometer/magnetometer) or angular acceleration (gyrometer) motion to record.40,41 Motion sensors were used for various applications:
In 31 studies, defined motion sequences (eg, rehabilitation exercises) or disorders (eg, neurodegenerative diseases) were examined with the aid of motion sensors.66,70
In 20 other studies, the focus was on general physical activity (eg, weight loss, sleep, or health promotion).40,41,42-53
In 20% of the identified studies, wearables were used to measure cardiovascular parameters (eg, heart rate, heart rate variability, and respiratory rate).8,9,20,26,31-38 A smaller number of sensors were used to measure (surface) skin temperature, electrodermal activity, oxygen saturation, and muscle activity.31,32,34,35
Calculated Parameters
At least with some wearables, the measurement method used does not directly measure the parameters, but estimate these from other signals, eg, if the heart rate variability is derived from PPG. Telemonitoring of vital signs with conventional medical products is not appropriate for capturing real-world data continuously.
Sensor Location and Areas of Usage
In 22.8% of the study goods, the sensors were attached to the wrist, which was the most frequently chosen localization.
In 25% of the 79 studies, the included patients were healthy or had frequent diseases of civilization such as obesity or arterial hypertension, with wearable activities (eg, physical activity and food intake) as endpoints.35,42 Patients with neurodegenerative diseases were the second-most studied cohort with 17.7%. On average, the studies had 135 participants; 25 of the 79 studies had >100 participants. The largest number of participants with 2659 participants was the randomized controlled clinical study of Steinhubl et al for the detection of atrial fibrillation with a wearable (adhesive ECG patch) in a risk population. 26 The average age of the patients in the study cohorts was 54.5 years.
Additional Aspects
The evaluation of the publications regarding the sensors used shows a considerable problem, the nomenclature is used—at least partially—inconsistently. For example, the terms “electrodermal activity” and “galvanic skin reaction” are used synonymously.
In 81% of the studies, the authors assess the use of wearables technology as predominantly positive with regard to the specific question of the study and the authors’ prior considerations for wearable usage. While the other studies found the wearable not consistently beneficial due to, eg, optimizable wearable features for the studied question, lack of interpretation options because of poor reference method or technical issues.39,46,67,73
In two studies, the evaluation was based on machine learning approaches.
One general problem with wearables that occurred in the studies was false-negative or false-positive alarms. These can lead to a low acceptance by patients if, for example, a false-positive alarm rate of 2.5 in 24 hours occurs during the detection of generalized tonic-clonic seizures by a wearable. 39
Discussion
In view of the rapid technical developments and the procedures already used by many patients as “self-monitoring,” a discussion of this topic is necessary. Wearables have an enormous potential for medical care, both for the care of individual patients and for prevention in the sense of public health approaches. The analysis of recent studies conducted with wearables shows that they can be successfully used in the medical context; however, certain aspects have to be taken into consideration:
Adequate selection of wearables taking into account the influencing factors with a precisely defined application context.
(Pilot) testing of the selected wearable in a small cohort of the target population and comparison of the results with those from an established reference method.
Clear definition of the practical procedures for the use of wearables for complete data collection and handling.
Selection of a suitable evaluation model of the determined data in relation to the research question.
Use of validated digital biomarkers (their development has only just begun, see “real-world walking speed” of the MOBILISED-D collaboration).
Vital parameters can be measured reliably and routinely with wearables. Ethical questions and data protection aspects need to be discussed transparently.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.