
Abstract
Background:
Extensive past work showed that noninvasive continuous glucose monitoring with a wearable Multisensor device worn on the upper arm provides useful information about glucose trends to improve diabetes therapy in controlled and semicontrolled conditions.
Methods:
To test previous findings also in uncontrolled in-clinic and outpatient conditions, a long-term study has been conducted to collect Multisensor and reference glucose data in a population of 20 type 1 diabetes subjects. A total of 1072 study days were collected and a fully on-line compatible algorithmic routine linking Multisensor data to glucose applied to estimate glucose trends noninvasively. The operation of a digital log book, daily semiautomated data transfer and at least 10 daily SMBG values were requested from the patient.
Results:
Results showed that the Multisensor is capable of indicating glucose trends. It can do so in 9 out of 10 cases either correctly or with one level of discrepancy. This means that in 90% of all cases the Multisensor shows the glucose dynamic to rapidly increase or at least increase.
Conclusions:
The Multisensor and the algorithmic routine used in controlled conditions can track glucose trends in all patients, also in uncontrolled conditions. Training of the patient proved to be essential. The workload imposed on patients was significant and should be reduced in the next step with further automation. The feature of glucose trend indication was welcomed and very much appreciated by patients; this value creation makes a strong case for the justification of wearing a wearable.
In the past few decades diabetes has become a major global disease, and with more than 640 million expected cases estimated by 2040 it receives a lot of attention because of both its social and economic implications. 1 Glucose sensors and other wearable monitors play crucial roles in improving diabetes treatment. At the same time the topic of exercise and motion per se has received increasing attention. Particularly relevant for people with diabetes, exercise is a very important component to improve glycemic control. 2 We have seen wide spread availability of motion trackers, step counters and other devices generally termed as “wearables.” There is now an emerging wave of more complex and sophisticated wearables starting to reflect increasing consumer and patient demands, and an increasingly holistic view on health per se. The last 20 years have witnessed the accumulation of broad scientific evidence, a catalyst and powerful motivation to pursue the development of such multisensor-based systems.
For example, it is known that one’s activity behavior during the day co-dictates how we sleep.3,4 The quality and duration of sleep in turn drives body restoration and hence the sustainability of how the human body can operate again after recovery. Imbalances, inappropriate diet or a sedentary lifestyle over a longer period can lead to subtle deteriorations of general health, fueling the development of chronic conditions. For people with diabetes this is of particular importance since they are more prone to develop comorbidities.
Nearly 20 years back, in 1998 Hakim et al reported about the distance walked versus mortality, and essentially demonstrated the longer you walk the longer you live. 5 In 2011 Studenski et al then showed the link between gait speed and mortality in people above 65, concluding that faster walking leads to reduced mortality and hence an increase in median survival. 6
Taking things yet another step further and considering more complex data beyond motion, one can see that a reduction of heart rate variability (HRV), a loss of temperature curve complexity, 7 the reduction of respiratory complexity or alterations in gait dynamics are linked to aging per se but also to certain chronic conditions, such as obstructive sleep apnea or metabolic syndrome.3,4,8,9 These variability measures have shown to hold impressive prognostic power and for many secondary conditions often seen in diabetes, HR characterization is also a central parameter.7,10
In 2016, McCrory et al presented the results of a longitudinal cohort study with subjects aged ≥50 and 4475 subjects with a mean follow-up of 4.3 years. 11 Beat-to-beat heart rate responses to standing were measured during a 2-minute window. Heart rate recovery (HRR) was then modeled to the stand by age group, cardiovascular disease burden, and mortality status. Speed of HRR in the immediate 20 s after standing was a strong predictor of mortality. A 1-bpm slower HRR between 10 and 20 s after standing increased the hazard of mortality by 6% controlling for established risk factors. Participants in the slowest recovery quartile were 2.3 times more likely to die compared with those in the fastest recovery quartile.
Obviously a person with diabetes is particularly interested in glucose dynamics. However, as summarized here, other physiological parameters and activity tracking are playing crucial roles and are rightfully becoming an increasing part of today’s diabetes therapy.2,12
A highly relevant and preferable “wearable” should be based on multiple sensors, will track activity and health parameters day and night over a longer period and may also feature glucose dynamic tracking capabilities. Of course, it should do so noninvasively and with a measurement frequency that provides adequate data granularity to feed standard medical protocols or scores for the decentralized monitoring and management of health. Since this requires quasi inter beat interval resolution for HRV capabilities it leads de facto to an “always on” modus operandi and therefore a defined requirement for battery real estate. This is the reason that the device developed and presented here in this study has been optimized to feature such capabilities—always on, long-term wearability, large battery capacity, and the future capability to monitor multiple parameters, including HR and its derivatives. Today, users are requesting “wearables” that provide multiple features and preferably in a first step also the capability to follow glucose trends and if possible, calibration free. The analyses presented in this article are therefore focusing on the users’ view and the glucose trend capability of the Multisensor device.
Methods
Study Population
Eligibility for study participation included age 18-60 years, BMI < 32 kg/m2, HbA1c < 9.0%, technically interested, and computer literate subjects with home internet access. A total of 20 patients, 13 male and 7 female patients of Caucasian origin with type 1 diabetes mellitus (age 38 ± 13 years (mean ± SD), BMI 24.1 ± 3.0 kg m-2, duration of diabetes 17.0 ± 13.0 years, HbA1c 7.5 ± 0.9%), participated in this open study. The study was performed in accordance with Good Clinical Practice and the Declaration of Helsinki. All patients signed an informed consent agreement, performed the screening visit and were then enrolled in the study.
Study Design
The study was aimed at long-term data collection with the Multisensor in a home and clinical setting during different periods of the year to allow evaluation of long-term attachment and performance.
A total of 34 patients were screened to eventually include 23 patients that where compliant with the inclusion criteria and importantly, after being introduced to the study, understood and agreed to bring up the significant time needed to complete the entire study.
Figure 1 shows a graphical illustration of the study procedure and the respective numbers of approved study days resulting from each phase. After the screening visit, patients completed an in-clinic study day (block A) to be introduced to the device and get trained in the operation of the set up. Patients collected each a total of ten home-use days (block B). Collected data were digitally and securely submitted periodically (if possible daily) to the study server via a semiautomated procedure. Once available on the server, data quality was then screened for compliance with respect to number of blood glucose reference measurements, duration of time series, and attachment quality. Patients could see attachment quality of the device on their PDA as a simple green or red bar.
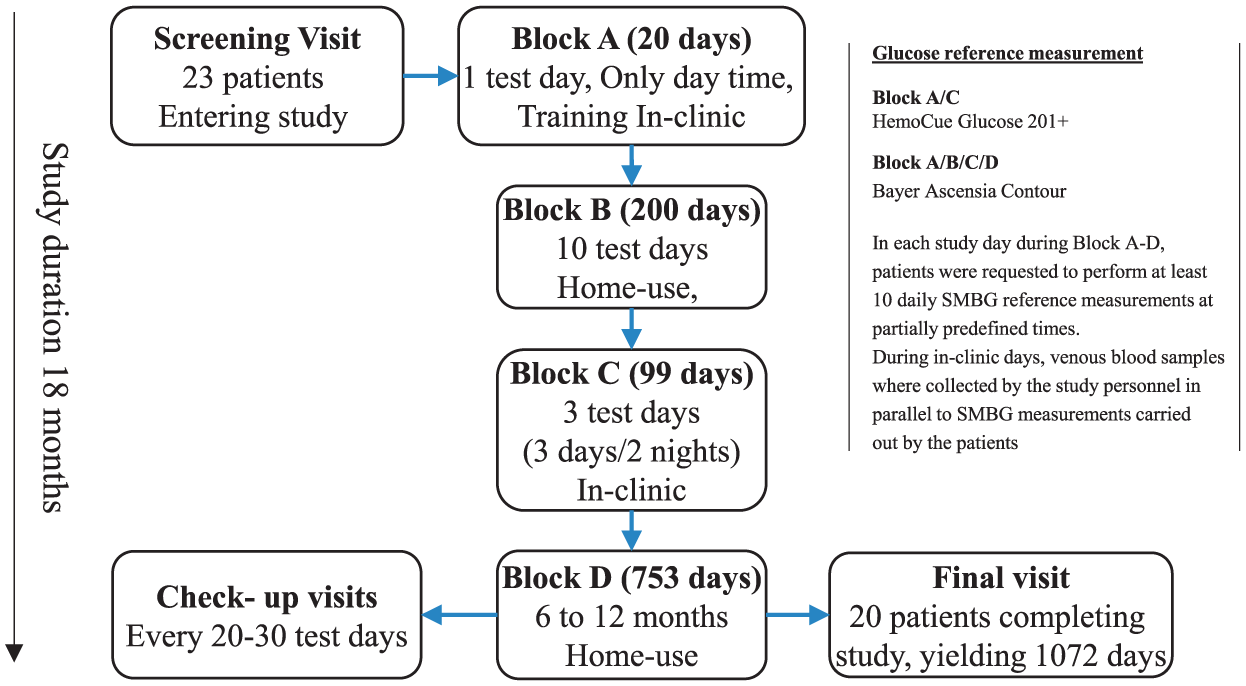
Illustration of study design. In block A approx. 10 hours’ worth of data were collected in each day (run). The study started in fall and lasted for approx. 18 months, hence covering all seasons with a wide spectrum of temperatures and weather conditions as normally experienced in Switzerland.
After block B, patients then returned for another three in-clinic days, including two nights to the study site. Blood samples were taken routinely (every 20 minutes during the days and every 60 minutes during the night) by the study personnel via an inserted venous catheter for blood glucose reference measurement using a HemoCue Glucose 201+ (HemoCue, Sweden). In parallel patients were performing regular SMBG via finger pricking (every 60 minutes during the day) and blood sampling, using an Ascensia Contour BMG (Bayer, Switzerland).
Moreover, during the entire study, patients were documenting insulin dosing, food intake, activity levels or special events using a dedicated log book tool installed on the PDA.
After completion of the three in-clinic days patients returned home to perform at least another 20 study days under regular home use conditions within a period of 6-12 months.
Over the entire study the following numbers of study days were excluded for one of the three reasons named above. In the end there were 1072 accepted and a total of 191 excluded study days (runs) respectively, which represent 15% of all runs. From these 191 study days, 49 (26%) were excluded due to a too low number of SMBG reference values, 65 (34%) due to inadequate attachment and 76 (40%) due to a too short duration of the run.
In the end 20 patients completed all blocks (A-C) with the minimum requirements fulfilled, three patients resigned from the study after block B due to personal time restrictions. Patients were contacted weekly to verify that there were no handling issues or other adverse events that needed investigation. Finally, a questionnaire was filled in by all patients at the end of the study to collect their views on the study structure, the wearability and handling of the device and what information they would want to have on the display.
Multisensor and Technical Infrastructure
One major difficulty met in developing NI-CGM sensors consists of dealing with intrinsic and extrinsic factors, being environmental and physiological processes. These can be blood perfusion changes, subcutaneous water migration, temperature variations or sweating, all very common sources of disturbance in daily-life conditions, acting as perturbing factors as they can significantly change the biophysical properties of skin and underlying tissue (SAUT) as well. If not properly controlled and taken into account, these non-glucose-related processes can greatly restrict the domain of applicability of NIGM sensors per se, making their accuracy acceptable only during specific conditions, such as in an in-clinic environment.13,14 A change in blood perfusion has profound biophysical effects over nearly the entire frequency spectrum with different underlying mechanistic manifestation. 15
For this reason, the proposed approach for NI-CGM aims at combining different sensors within the same device, creating a Multisensor concept, to detect and compensate for those disturbances leading for decreased accuracy.
We have reported extensively along the development path building on the theoretical, in vitro and in vivo bases.16 -20 It has been shown that glucose variations induce significant changes in the electrical properties of SAUT that can be followed by respective sensors. Several clinical studies have been performed in the past using the Multisensor within a controlled or semicontrolled environment. To utilize the developed data evaluation routines and to further collect a substantial body of data from a nearly unrestricted environment this outpatient study has been performed. The article here provides a first report to disseminate these findings. Due to the substantial amount of information collected during this study we will need to separate general basic findings from very detailed and extensive data analyses. Furthermore, we will also separate the investigators view and the patients view. It must be emphasized that the main goal of this outpatient study was to collect a substantial body of information, such as data for further development, get basic patient/user feedback on the fundamental handling and wearability of the device, apply developed routines and simply understand to which extend it is possible to collect reliable sensor readings per se over a longer period by the patient in an uncontrolled environment. Figure 2a shows a schematic illustration of the device used and its attachment on the upper arm.
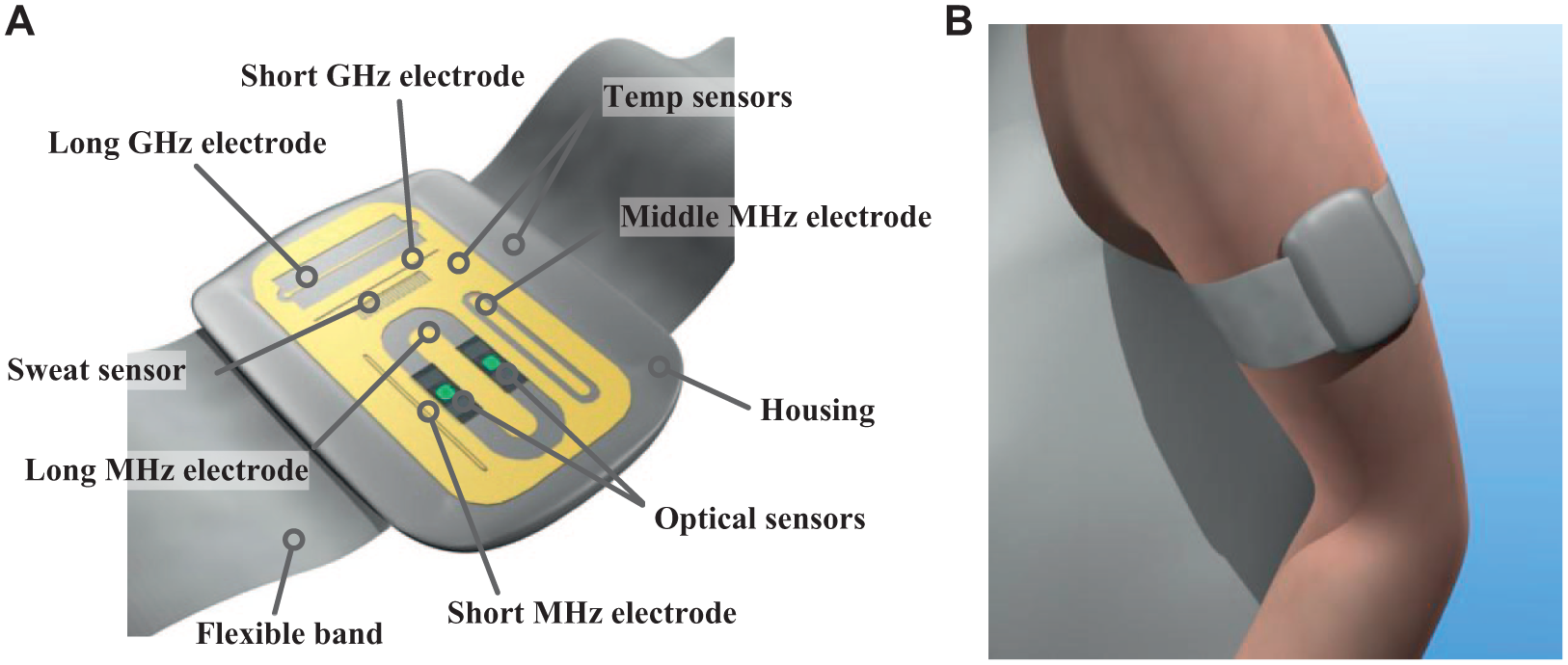
(a) Schematic illustration of the combination of the optical diffuse reflectance sensors and electrodes of the dielectric sensor on the substrate of the Multisensor system. (b) Attachment of the Multisensor to the upper arm with a flexible band.
The Multisensor device features 19 different sensor signals, including optical and dielectric sensors to perform biophysical characterization of SAUT as well as accelerometer, two temperature and one humidity sensors. Dielectric SAUT properties are collected in three frequency regions: 1-200 kHz to monitor sudomotor activity, 0.1-100 MHz with 3 different electrodes to monitor the effect of glucose variations and 1 and 2 GHz with two different electrodes to monitor the effect of water migration. Last but not least, optical properties of the skin are monitored with diffuse reflectance sensors to monitor hemodynamic changes. The Multisensor measures all sensor signals every 20 seconds and was connected via Bluetooth with a HTC PDA, running Windows Mobile 6.1, continuously collecting the sensor readings from the Multisensor. After completion of the study day, the device was taken off by the patient for charging and the data collection stopped automatically. The PDA was then connected with a Laptop computer using a USB cable. Upon connection a program started automatically, downloading the sensor data from the PDA as well as the log book entries. The same was done with the Bayer Ascensia Contour BMG. All collected data (sensor readings, log book entries, SMBG reference values and InsulinBolusSA, InsulinBolusLA, InsulinPump details) were then automatically and securely uploaded to the clinical study server for further processing by trained study personnel.
Results
The full sensor signal data analyses procedure is described in detail in Part II and includes model definition, estimation and application, calibration, novelty detection, output filtering, performance calculation, and clinical relevant statistical metrics. The results presented here are based on the analyses performed on the same procedures. Here we focus on the user experience, trend information, and patient observations.
Over the entire study there were 3431 HemoCue lab reference values collected, 13 338 SMBG measurement points taken, 4395 short-acting and 271 long-acting insulin bolus injections registered plus a total number of 4359 meals/snacks protocolled. Figure 3a shows a respective graphical illustration with the distribution over the individual blocks. Figure 3b shows sampling rhythmicity of the two reference methods over the study blocks. Finally, Figure 3c shows the overall distribution of study days for each patient over the entire study period. It covers all relevant seasons including winter, spring and summer to impose a wide spectrum of different climatic conditions.
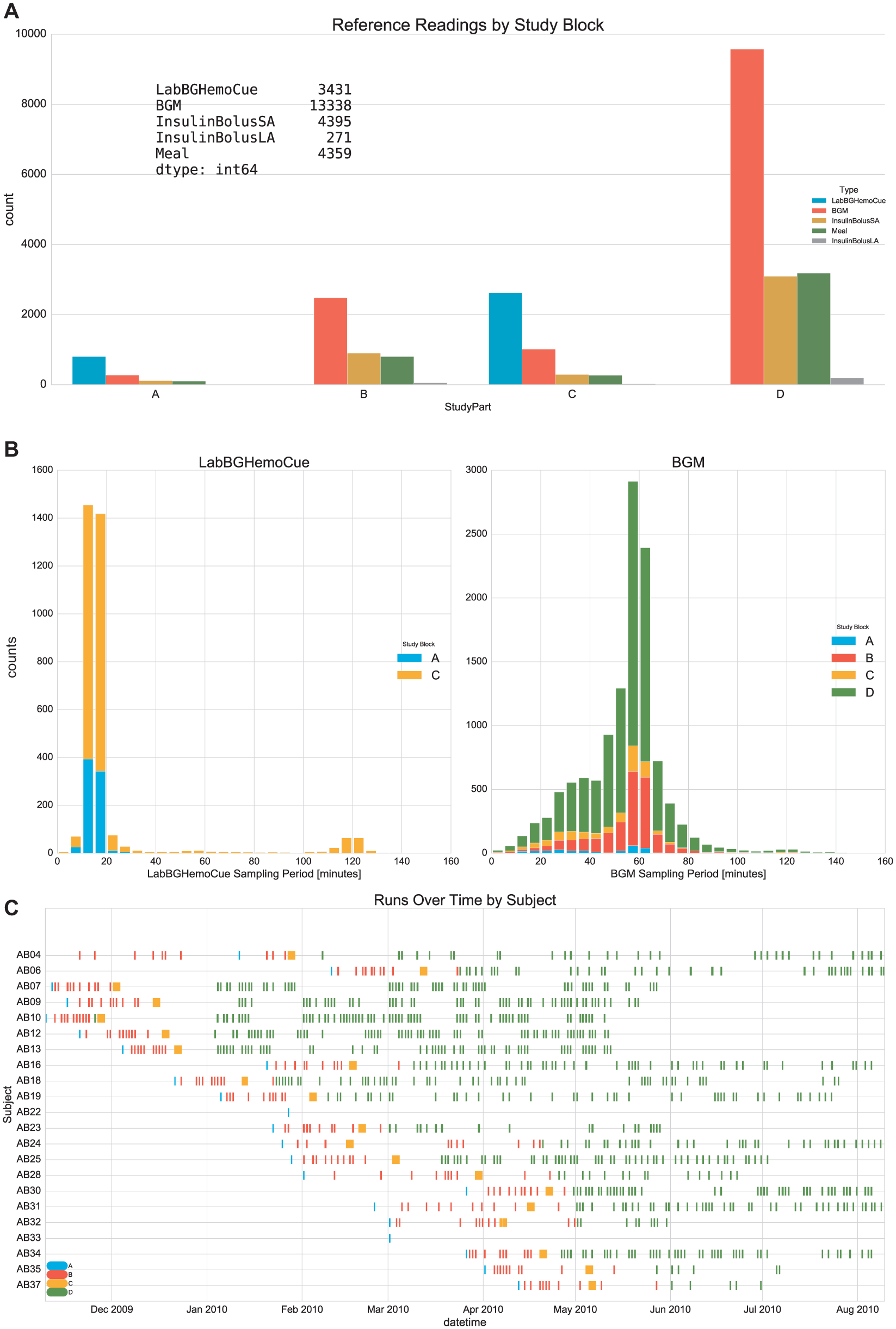
(a) Total reference readings and other recordings for all patients by study block. (b) LabBGHemoCue represents the gold standard reference method for blood glucose assessment. BGM represents blood glucose monitoring performed by the patients himself. InsulinBolusSA/LA represents short- and long-acting self-administration of individual insulin injections. (c) Distribution of study days over time for each patient. A sequenced patient onboarding over the months has taken place.
Not all patients completed the same numbers of study days in block D. Seven patients completed at least 50 runs in block D, eight patients completed between 30 and 50 runs and 5 patients completed less than 30 runs. The minimum runs defined were 20 study days, which was achieved by all 20 patients.
The results of the analyses presented here are focusing on the trend capabilities with respect to reference data.
Table 1 summarizes the distribution of glucose trend dynamics seen in patients per se, comparing SMBG versus reference blood glucose measurements taken by the study personnel in block C. Table 2 summarizes the effectively found trend indication by the Multisensor versus invasively measured reference blood glucose values. Glucose trends are calculated with the same rhythmicity of 20 seconds, and the output reported in mg/dl/min units.
Relative Number of Values in a Specified Glucose Trend Range.

Glucose trend is defined as average glucose rate between two consecutive readings. Readings compared between RBG and SMBG.
Relative Mismatch of Multisensor Trends Tabulated With Respect to the Specified “Number of Ranges Apart” From the Reference Trends.
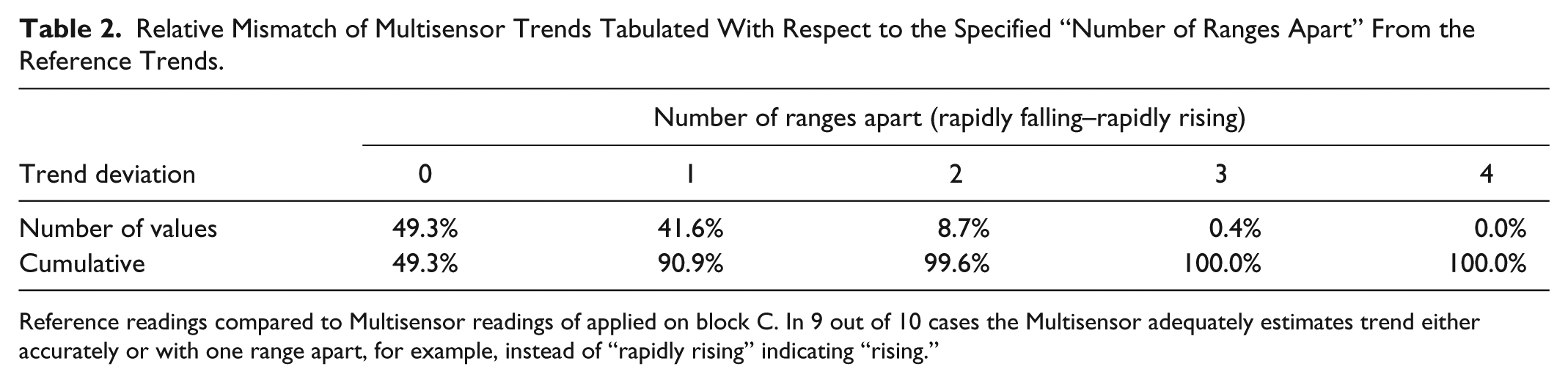
Reference readings compared to Multisensor readings of applied on block C. In 9 out of 10 cases the Multisensor adequately estimates trend either accurately or with one range apart, for example, instead of “rapidly rising” indicating “rising.”
SMBG performance by the user can lead every now and then to erroneous measurements due to mishandling or an unfavorable surrounding situation. We compared the in-clinic reference data from block A/C from HemoCue (measurement performed by the study personnel as reference blood glucose—RBG) and SMBG from Bayer Ascensia (measurement performed by patient). We obtained an MARD = 11.8%, Clarke AB = 97.3%, Clarke A = 82.3%, R2 = 0.9, RMSE = 26.6mg/dL. This can give an indication of what effect an initial baseline adjustment can have if erroneous sampling is then introduced to an NIGM system. Eliminating the need for reference sampling in an initial trend setup eliminates not only the need for invasive SMBG but also a possible source of error.21,22
Discussion and Conclusions
The upper arm attachment has shown to be very well tolerated and was reported to be a comfortable location to wear the device also for a longer period. Training was however needed to ensure a most comfortable placement. Selection of adequate band size has shown to be highly relevant. A too long band led to inappropriate attachment with reduction of data quality in the dielectric sensors. A too tight band to discomfort over time and in some cases to a situation where skin could unintentionally get stuck between the housing and band attachment site. If unnoticed this then caused in three cases tissue to become clamped, leading to a skin blister. In all cases the issue was solved and eliminated after a retraining.
Sweating was never reported to be an issue. However, devices that where showing small inconsistences in the sensor substrate homogeneity due to manufacturing imprecisions were reported to be less comfortable. As a rule of thumb what can tactually be felt on a surface as geometric inconsistency has the potential for skin sensitizations and needs to be avoided. In one case the device produced a skin lesion under the sensor substrate that needed recovery by pausing for 7 days. The investigation pointed toward a dermal sensitization to certain metals (such as copper) that are used as bonding agents to couple gold, used as the sensory structures, to the multilayer ceramic substrate.
All patients that withdrew from the study did so in the first part. Before block C and after being confronted with the significant daily workload to adhere to the study protocol. To adhere to the protocol a minimum of 10 daily SMBG values, daily data transfer, digital log book running and a total of 4 days in clinic time was required. This led to a daily workload of 60-90 minutes and also presented the main reason for those 11 patients that though passing the screening eventually did not enter the study due to the heavy workload.
Showing patients a traffic light on the PDA to display attachment quality and measurement progress for the day was very useful and together with the digital log book engaging. Doing this at a larger scale it is recommended to further evolve the user experience and interaction. A future set up that might permit other physiological parameters to be displayed and put that into an overall health context could be a very attractive step to continue collecting evidence in a larger study.
One of the most important elements was to understand the capability of the Multisensor to track trends. It can do so in 9 out of 10 cases either correctly or with one level of discrepancy. This means that in 90% of all cases the Multisensor shows glucose dynamics to rapidly increase or at least increase. This feature has been very much appreciated by patients and seems to provide value to justify wearing a wearable.
Performing this study has proven to be an enormous opportunity to learn, discover procedural challenges, reveal technical issues or subtle errors in the experimental setting. The organization of the study via four blocks with regular check points has proven to be highly useful.
Patients were interviewed every four weeks. As indicated, the majority reported a high interest in glucose trend given as an arrow on a display as already a very meaningful piece of information to have. The analyses identifies such functionality could even be made without an initial baseline calibration, as it can be decoupled from the absolute value.
The requested sampling rhythmicity of at least 10 SMBG/day proved to be a challenge in some of the patients and as reported, led to the exclusion of 5% of study days due to under sampling or inappropriate rhythmicity. For a larger follow-up study it would however be very useful to reduce the overall burden of SMBG sampling and to provide additional value via the display to create an incentive for the less enthusiastic patients to also participate in such a broader study. This would warrant the inclusion of vital parameters for example to make a further step in the direction toward a more holistic view on health per se as presented in the introduction here. Moreover, supplementing or even replacing SMBG with less disruptive minimally invasive CGM as reference method should be considered.
To expand such a study and perform at a significantly larger scale it will be important to have as much automation and integration as possible to minimize the user workload. However, enrolled patients were highly motivated to contribute in an optimal way to the successful collection of data that could be used for further processing.
Last but not least, much attention was given to the automation and synchronization of the various data streams. With the likely occurrence of even more references and third party data streams and the necessary convergence thereof, it will be of great importance to fully leverage automatic data synchronization, data upload, and automatic verification of data integrity.
The next study along these lines should bring trend features combined with other physiological parameters investigated within a broader audience over a longer period. This will then also promote the collection and investigation of longitudinal data in combination with machine learning functionality. Ultimately leading toward the advancement of objective scores to better map health and derive actionable elements from a truly holistic view.
Footnotes
Acknowledgements
Thanks go to various people from former Solianis Monitoring AG and to dedicated international partners for their solid contributions that allowed expanding on the understanding of underlying mechanisms and characterization of phenomena related to noninvasive glucose monitoring.
Abbreviations
BG, blood glucose; CGM, continuous glucose monitoring; HRR, heart rate recovery; HRV, heart rate variability; NI-CGM, noninvasive CGM; PDA, personal digital assistant; RBG, reference blood glucose; SAUT, skin and underlying tissue; SMBG, self-monitoring blood glucose.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Solianis Monitoring AG.