
Abstract
Islet transplantation is a promising curative treatment option for type 1 diabetes (T1D) as it can provide physiological blood glucose control. The widespread utilization of islet transplantation is limited due to systemic immunosuppression requirements, persisting graft immunodestruction, and poor islet engraftment. Traditional macro- and micropolymeric encapsulation strategies can alleviate the need for antirejection immunosuppression, yet the increased graft volume and diffusional distances imparted by these coatings can be detrimental to graft viability and glucose control. Additionally, systemic administration of pro-engraftment and antirejection therapeutics leaves patients vulnerable to adverse off-target side effects. Nanoscale engineering techniques can be used to immunocamouflage islets, modulate the transplant microenvironment, and provide localized pro-engraftment cues. In this review, we discuss the applications of nanotechnology to advance the clinical potential of islet transplantation, with a focus on cell surface engineering, bioactive functionalization, and use of nanoparticles in T1D cell-based treatments.
Introduction
Type 1 diabetes (T1D) is a chronic autoimmune disease characterized by the selective destruction of insulin-producing beta-cells in the pancreatic islets of Langerhans. 1 In the United States, an estimated 1.25 million people have been diagnosed with T1D, with conventional treatment methods relying on frequent blood glucose monitoring and exogenous insulin administration. 2 This current standard fails to provide optimal, physiological glycemic regulation, which instigates life-threatening complications such as retinopathy, neuropathy, nephropathy and, in a cohort of patients, potentially fatal hypoglycemic unawareness.3-5
Beta-cell transplantation exhibits a promising treatment option that can deliver endogenous and physiological insulin release. In one approach, termed clinical islet transplantation (CIT), cadaveric human islets are infused into the hepatic portal vein. In 2000, the clinical potential of CIT was revitalized with the adoption of the Edmonton Protocol, which utilizes a steroid-free immunosuppression regimen and strives for an islet graft mass of 10 000 islet equivalents (IEQ) per kilogram of body weight.6,7 Despite the demonstrated success of CIT in severely labile patients with T1D, 8 the widespread application of islet transplantation remains restricted due to multiple limitations. Specifically, pancreatic islet donor scarcity requires the development of beta-cells from more abundant sources, such as stem cells or porcine tissues.9,10 Further, the compulsory life-long immunosuppression regimen required to prevent graft rejection leaves recipients vulnerable to opportunistic infections and oncogenesis; this elevated risk prevents its use in patients with T1D exhibiting moderate glycemic control. 8 Finally, CIT is limited by poor cell engraftment and recurring autoimmunity, which hinders the durability of the treatment.11,12
Seeking to address these challenges, researchers are exploring multiple avenues for improving cellular engraftment and immunoprotection. Applying nanoscale engineering techniques to the islet transplant system can facilitate improved therapeutic localization, elegant control of spatial and temporal distribution, and increased therapeutic power.13,14 In this paper, we review the applications of nanotechnology in immunoisolation, bioactive functionalization, and therapeutic nanoparticle delivery for islet transplantation.
Nanoscale Immunoisolation
Despite enrollment in a systemic immunosuppression regimen, a major obstacle in successful islet engraftment is the host’s immune response to the foreign graft. In the first week following intraportal transplantation, up to 60% of the islet mass is lost due to general surgical trauma. 12 Additionally, an instant blood mediated inflammatory reaction (IBMIR) is instigated by both the inherent inflammatory nature of the donor islets’ surface as well as protein adsorption to the cellular graft upon blood contact. 15 This activation triggers complement and coagulation cascades, which, in turn, recruits innate immune cells, namely neutrophils, monocytes, and macrophages, to the transplant site. 15 Innate immune cells further propagate this inflammatory microenvironment by secreting pro-inflammatory factors, such as cytokines, chemokines, and reactive oxygen species (ROS), to activate and recruit adaptive T and B cells.16,17 Antigen-specific cytotoxic T cells recruited to the site recognize and kill islets through direct T cell-graft cell contact. Conversely, the interactions between antigen presenting cells (APC) presenting donor and beta-cell antigens to host T and B cells result in their activation via indirect allorejection.18,19 Activated T helper cells accelerate graft rejection, while activated B cells generate antibodies to both donor antigens and beta-cell antigens to assist in flagging these cells for phagocytic clearance.18,19
A popular strategy to prevent the immune-mediated reaction of allogeneic islets is the encapsulation of these cell spheroids within a semipermeable, immunoisolating material or device. With the ultimate goal of eliminating the need for immunosuppressive drugs, polymeric encapsulation devices provide a physical barrier to block direct interactions with host effector T cells, while permitting nutrient exchange and glucose-responsive insulin secretion.20-22 By limiting host-graft interaction, permselective membranes can also overcome limitations in donor availability by expanding the feasibility and safety of xenotransplantation and stem cell derived cell sources. The most common formats for encapsulation are macroencapsulation sheet devices or microcapsules.23,24
Despite considerable efforts to translate encapsulation approaches to patients, strong clinical efficacy of any encapsulation-based platform has yet to be shown.25-27 The failure points of these implants have yet to be fully elucidated, but there are likely multiple factors contributing to their insufficient glycemic control. A significant concern regarding encapsulation platforms is the high metabolic demand of islets.28,29 As islet encapsulation creates diffusional barriers in the delivery of nutrients, even micron-scale barriers can lead to significant impairment in sufficient oxygen delivery to meet the metabolic demands of these cells, resulting in decreased insulin responsiveness and hypoxia-induced necrosis.30,31 To further compound this impact, accessible implant sites for capsules, such as the peritoneal cavity, are poorly oxygenated. 32 While decreasing cell loading density within these encapsulation platforms can reduce overall metabolic demand and elevate graft viability, the clinical scalability of these devices typically results in unrealistic graft volumes.20,33 While innovative microfluidic techniques are decreasing this micron scale from 1000 to 10 µm, 34 these approaches tend to generate many cell-free capsules that require purification to remove empty polymer beads prior to implantation. 35
The application of advancements in nanotechnology and polymer chemistry can aid in resolving some of these issues. Specifically, the development of ultra-thin immunoprotective cell coatings can support adequate nutrient diffusion and efficient glucose-stimulated-insulin-release by substantially decreasing the diffusional barrier between the cellular transplant and the host microenvironment. Due to the relationship between diffusional length and time, decreasing the diffusional length scale by only tenfold results in a 100-fold reduction in diffusional time. 36 Thus, converting micrometer scale capsules to the nanoscale should virtually eliminate diffusional-imposed sensing and secreting delays.
To form nanoscale barriers, polymeric deposition typically takes the advantage of intrinsic chemical properties of the pancreatic islet. This can be the cell membrane itself or the outer extracellular matrix (ECM) coating left on the islet post-isolation and/or generated by the nonendocrine islet-resident cells during culture. 37 This cell surface engineering approach provides elegant nanoscale control over layer formation, with resulting layers serving to both mask instigating cell surface agents and accommodate the hepatic portal vein transplant site. To generate nanoscale immunoisolatory barriers, two major approaches have been explored: PEGylation and layer-by-layer (LbL) (Figure 1).
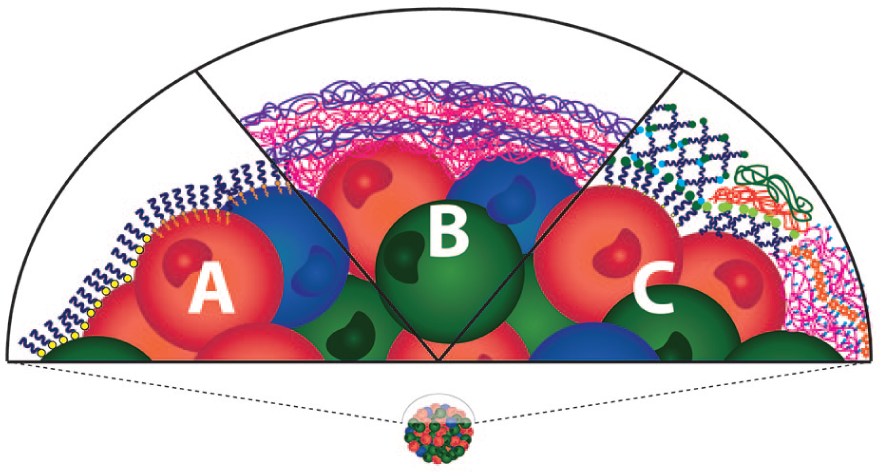
Surface engineering of the pancreatic islet via nanoscale PEGylation or layer-by-layer coatings can serve to mask the foreign cellular surface from host immune cell recognition. (a) The grafting of long-chain poly(ethylene glycol) can be achieved via covalent binding or lipid tail integration into the cellular membrane. (b) Electrostatic layer-by-layer coatings can be generated directly on to the islet surface. (c) To prevent cytotoxic responses to polycations, a base layer of poly(ethylene glycol) can be added prior to polyelectrolyte multilayer formation and/or layers can be fixed via covalent, hydrophobic, or biological recognition sites.
Islet PEGylation
Poly(ethylene glycol) (PEG) is a low-fouling, hydrophilic polymer that has been extensively explored in immunomodulatory surface modification due to its ease of functionalization and benign backbone. 38 Early work in exploring the immunocamouflaging capabilities of cell surface PEGylation illustrated the capacity of PEG cell grafting to mask cell surface foreign epitopes on red blood cells.39,40 This pioneering work exhibited the utility of simple long-chain PEG grafting in delaying cell-cell interactions with decreased recognition of immunogenic surface agents, such as major histocompatibility complexes (MHC). 39 For utilization in islet transplantation, cell surface PEGylation has the potential to prolong graft function by mitigating IBMIR, concealing surface antigens, and limiting cell-cell interactions. Islet-surface PEGylation has been studied using the following conjugation strategies: covalent bonding and hydrophobic interaction.
PEGylation via covalent bonding
Covalent cell surface modification can be achieved using functional groups that are naturally present in the cell membrane and/or in the protein-rich ECM surrounding the cell cluster (Figure 1(a)). These binding moieties include free amines or thiols present on cellular membranes and extracellular matrix proteins. 38 For islet PEGylation, the most utilized covalent bonding reaction is between a linear, long-chain (>2000 Da), bi-functional PEG terminated with an amine-reactive group and an inert methyl group. The amine reactive group, eg, N-hydroxysuccinimide (NHS ester), isocyanate, and succinimidyl-propionic acid (SPA), spontaneously binds to cell surface primary amino groups, resulting in the formation of a stable amide bond39,41-43; the benign methyl group on the other end of the PEG chain presents an inert group to the external environment. Several groups have shown uniform PEG binding using this covalent grafting approach with strong cytocompatibility and functional response to a glucose challenge.41-43 In vivo allogeneic kidney capsule transplant studies examining the immunoprotective effect of PEGylated pancreatic islets quantified extended graft function and mitigation of immune cell infiltration when fully MHC mismatched allogeneic islets were implanted within chemically induced diabetic mice 43 ; however, long-term graft viability was not durable or complete. With the hypothesis that elevating the PEG grafting would enhance immunoprotection, Lee et al explored additional PEG coatings using multiple incubations of PEG-SPA. 44 In an allograft rat model, a triple PEGylation procedure resulted in almost a twofold extension in graft function (eg, 12-19 days), when compared to their single PEGylation protocol. This hypothesis was further explored by Jeong et al, who incorporated a six-arm PEG to generate a dense, conformal coating. 45 In this approach, PEG was grafted via catechol, an amine-binding moiety derived from mussel adhesive protein. The resulting PEGylated islet grafts did not significantly extend graft protection, although the transplant model tested was a more aggressive mismatch (ie, rat islets into murine recipients). 45
PEGylation via hydrophobic interactions
The spontaneous incorporation of lipid alkyl tails within the cell membrane provides an alternative method for the homogeneous surface coverage of PEG chains (Figure 1(a)). Teramura and colleagues developed a PEG-conjugated phospholipid platform exploiting this approach, whereby the lipid tail was found to easily integrate into the cell membrane of peripheral islet cells. 46 The resulting coating had minimal impact on islet survival and glucose response profile. Additionally, xenotransplantation of PEG-lipid coated hamster islets into chemically induced diabetic mice not only illustrated the feasibility of intraportal infusion of these PEGylated islets, but also resulted in modest delays in graft rejection when compared to untreated islets (from 1.8 to 5.0 days) despite an aggressive xenograft model. 47 Compared to covalent surface modification, it is postulated that PEG grafting via hydrophobic interactions confers less damage to islet membrane protein structures and integrity38,47; however, due to membrane turnover, the viability of this platform as a long-term, steric immunoprotection barrier is likely short-lived. 48
While the impact of PEGylation on overall graft survival within murine models was modest, at best, multiple reports have illustrated a synergistic effect when PEG grafting of the islet is combined with low-dose and/or short-course immunosuppression. In allograft murine models, graft survival has been extended from short term (<20 days) to long term (>100 days) when PEGylated islets were combined with the systemic, but transient, delivery of immunosuppressive agents such as cyclosporine, anti-LFA-1, heme oxygenase-1, tacrolimus, or anti-CD154 mAb.42,43,45,49 Thus, while PEG grafting alone is not a particularly potent immunoisolation approach, this approach provides a drug-free method to boost the efficacy of many immunosuppressive agents. Further, PEGylation approaches can serve as base layers for additional LbL coating approaches.
Nanoscale LbL Encapsulation of Islets
The imperfect immunoprotection achieved by single-layer PEGylation can be fortified through LbL nanofilm polymer assembly. Exhibiting greater stability and homogeneity, the sequential cell surface deposition of polymers creates an immunoisolating, conformal coating with controllable thickness, permeability, and surface chemistry. 21 Furthermore, the utilization of multiple layers can impart multifunctionality. For example, the base or first layer can serve as the islet interface, while middle layers can be customized to control permeability and/or stability. Finally, the outer layer can serve as the interface with the host, which can be functionalized to direct desirable host responses (see “Bioactive Functionalization Strategies” section). Nano-thin LbL islet polymer coatings are more commonly generated through cell surface electrostatic interaction, although alternative approaches, including covalent bonding, hydrophobic interaction, and hydrogen bonding, have also been utilized.
Layer-by-layer coatings formed via electrostatic interactions
Islet LbL nanofilm assembly via electrostatic interaction is achieved by the alternate deposition of oppositely charged polymers. Using the relatively negatively charged cell surface as the electrostatic complexation substrate, cationic polymers can be directly assembled on to the islet surface (Figure 1(b)).
50
Numerous polycationic polymers have been screened as potential base layers for polyelectrolyte multilayer (PEM) cell coatings, including poly(
While PEM provides an efficient means to generate multiple layers, a major issue in PEM nanofilm assembly is the cytotoxicity of the polycation, which can induce plasma membrane pore formation and subsequent cell death.44,51,52 Several studies have reported the cytotoxic effect of direct contact between commonly employed synthetic polycations, such as PLL, PAH, PDADMAC, and PAAm, and cells.44,51,52,54 Seeking to mitigate this cytotoxicity, Lee et al first grafted long-chain PEG onto the islet surface (as described in “PEGylation via covalent bonding” section). 44 Despite the PEG barrier, the exposure of PEGylated islets to cationic PLL or PAAm resulted in significant cytotoxicity and functional impacts, with clear peripheral cell damage to the islet spheroid. 44 In another approach, Wilson et al grafted PEG onto PLL (termed PLL-g-PEG), postulating that PEG would mitigate cell membrane disruption while retaining the net positive charge of the polymer.54,55 Extensive characterization of the impact of PEG length and the degree of modification on cytocompatibility and layer formation was conducted to generate an optimized PLL-g-PEG composite. 50 While PLL alone resulted in significant cytotoxicity after only 15 minutes, the final optimized PLL-g-PEG polymer did not convey any observable negative effects, even after 12-hour exposure.50,54 To formulate multi-layers, alginate was then used as the polyanion, with the incubation of islets in alternating solutions of PLL-g-PEG and alginate resulting in uniform nanoscale encapsulation. To explore the impacts of this coating in vivo, eight-bilayer PLL-g-PEG/alginate nano-encapsulated C57BL/10J islets were intrahepatically transplanted into chemically diabetic C57BL/6J mice. As a concordant allograft, the immunoprotective nature of the coating was not fully evaluated; however, the PLL-g-PEG/alginate modified islets exhibited statistically comparable efficacy when compared to uncoated islets. 50
Moving away from the classic polycation solutions, others have leveraged phosphorylcholine-derived chitosan for the formation of PEM layers.56,57 In one approach, Zhi et al generated nanofilms using chitosan and alginate, with a final layer of chondroitin-4-sulfate to impart anticoagulant properties. 56 Islets coated with eight layers of chitosan/alginate exhibited no visual decline in viable cells and only a modest delay in dynamic glucose-responsive-insulin-secretion when compared to uncoated controls. 56 Upon transplantation, chitosan/alginate-coated islets demonstrated a modest delay in the reversion of hyperglycemia, when compared to untreated islets; however, the coating delayed allograft graft rejection, with the preservation of islet function in >70% of the mice during the 30-day observation period. 56 Additionally, Syed et al applied a nine-bilayer chitosan and PSS coating approach to murine and human islets. 57 Chitosan/PSS-coated islets exhibited decreased susceptibility to cytokine cytotoxicity in vitro when compared with uncoated islets. Transplantation of chitosan/PSS-coated human islets decreased blood glucose levels in diabetic murine recipients, albeit statistically equivalent to untreated controls. 57
In an alternative approach to mitigate polycation cytotoxicity, neutral polymers can be used as intermediates to initiate the electrostatic adsorption of polymers. Miura et al demonstrated this approach by using an amino group-terminated PEG-lipid as the primary anchor to then subsequently form sodium alginate and PLL bilayers. 46 In another approach, Kikravesh et al preconditioned beta-cell clusters with calcium chloride prior to PEM complexation. 58 Calcium preconditioning enabled the deposition of an anionic alginate layer, which is less cytotoxic, as the primary layer, with subsequent building using traditional PEM polymers. Encapsulated MIN-6 spheroids displayed unimpaired viability and functionality and were able to protect against antibody binding and inflammatory cytokine stimulation. 58
Overall, the generation of nanoscale coatings via polyelectrolyte LbL formation has been shown to be highly efficient, controllable, and uniform. While several innovative approaches are seeking to mitigate polycation cytotoxicity, polyelectrolyte layer formation can be unstable due to its dependency on electrostatic interactions. Over time, these layers can disassemble; a feature that is more accelerated within a physiological environment. In addition, polycations are known instigators of an aggressive foreign body response.59-61 The mobility of these electrostatic layers within the coating inevitability results in the exposure of the polycations to the external environment, even if the terminal coating layer is designed as a polyanion. 62 Due to these challenges, alternative LbL approaches are seeking to employ methods that result in enhanced stability and improved biocompatibility (Figure 1(c)).
Layer-by-Layer coatings stabilized via alternative interactions
To improve the stability and provide additional flexibility to coatings formed using charged polymers, Wilson et al further functionalized their PEG-grafted PLL with biotin (PLL-g-PEG(biotin)). 54 The biotin group provides a means to build layers via biotin-streptavidin binding interactions, a noncovalent biologically based interaction with high affinity (Kb = 1015 M−1). Multilayer nanofilms were generated onto the islet surface using PLL-g-PEG(biotin) and streptavidin, with no significant changes in islet viability or function when compared to control. 54 While resulting coatings are likely more stable, excess biotin can result in disassembly. To enhance stability, the biotin functional group can be replaced with an azide or hydrazide, which can form covalent bonds when exposed to polymers expressing aldehyde or cyclooctyne groups, respectively. 55
To further improve stability, polymers can be functionalized to promote covalent binding between layers during LbL formation.63-65 Applying to islet encapsulation, covalent stabilization of layers should result in improved coating stability with the inhibition of intralayer mobility. 66 In one approach, covalent layers were generated onto an islet surface by combining covalent PEGylation with chemoselective functionalized polymers. 67 Specifically, islets were first PEGylated with a long-chain PEG terminated with azide (N3). This functional group permitted subsequent layer formation via Staudinger ligation, a biorthogonal reaction where N3 spontaneously and chemoselectively reacts with a phosphine group to generate a stable amide bond. 68 Incubation of islets coated with PEG-N3 with a four-arm PEG terminated with a complementary phosphine group resulted in layer formation. 67 Resulting coatings did not alter viability or function and coated BALB/c islets exhibited immune-protective effects when transplanted into chemically induced diabetic C57BL/6J mice, with 57% of coated islet achieving long-term (>100 days) graft survival. 67 While promising, this layer approach is inefficient and nonuniform, due to the high flexibility of the PEG arms and the low density of reactive groups. To improve upon this approach, new polymers were developed, specifically poly(amidoamine) (PAMAM) dendrimers and hyperbranched alginate. The defined branched structure of dendrimers facilitates high functional density and predictable surface expression, while applying a hyperbranching feature to the alginate backbone elevates the number of functionalization groups and the rigidity of their presentation. 69 In a recent publication, PAMAM dendrimer and hyperbranched alginate were functionalized with complementary Staudinger ligation reactive groups and used for covalent LbL encapsulation of islets. 70 Similarly, Teramura et al built covalent LbL coatings using a primary maleimide-PEG-lipid (MAL-PEG-lipid) anchor. 71 Additional layers were generated through the covalent thiol-disulfide exchange of poly(vinyl alcohol) functionalized with thiol (SH) and pyridyl-disulfide. 71 Overall, these methods illustrated the efficient generation of uniform and stable coatings.
Alternative to electrostatic or covalent-based LbL encapsulation, Kharlampieva’s group has explored the use of noncationic compounds and hydrogen bonding to facilitate LbL deposition. Specifically, phenol-containing tannic acid was adsorbed onto the islet surface and retained in place via hydrogen bonding with poly(N-vinylpyrrolidone) (PVPON). 72 Multiple bi-layers, up to six, could be deposited onto the islets, with demonstrated stability up to a week in culture. Encapsulated islets retained cell viability and functionality and restored normoglycemia in a diabetic transplant model comparable to uncoated islets.72,73 These polymers can also impart additional beneficial functions, such as antioxidant capacities (as discussed in further detail in “Bioactive Functionalization Strategies” section).72-74
The use of additional interactions to deposit layers onto the viable islet cluster provides additional stability and reduced toxicity. Furthermore, the use of functional handles on polymers provides a platform for the presentation of additional agents that can further modulate the local microenvironment. With proof-of-principle coatings generated, future work should focus on the detailed evaluation of their stability, subsequent impacts of these coatings on the islet interface, and clear validation of their immunoprotective capacity.
Other Surface Engineering Strategies
As highlighted in the earlier sections, deposition of the first polymeric layer onto the islet spheroid can be one of the most challenging issues. Interactions of polycationic polymers with the cell surface lead to cytotoxicity. Lipid-based layers that integrate into the cell membrane lose their stability over time due to cell membrane recycling. Covalent-based islet PEGylation, while highly efficient, generally stable, and cytocompatible, is not ideal for subsequent layer deposition. Specifically, the subsequent deposition of polyelectrolyte polymers for PEM layer formation is difficult, as the PEG typically presents a net neutral charged surface. For covalent methods, the flexible nature of the PEG can lead to masking or delays in interactions of the functional groups for bond formation. Finally, the interactions of a synthetic polymer with the islet surface may further exacerbate islet anoikis (ie, programmed cell death due to the lack of matrix binding) at the periphery.
Alternative approaches to initiate conformal coatings directly onto the cell surfaces leverage natural or biomimetic polymers that present ECM-cell binding motifs. In one approach, fibronectin, a multifunctional glycoprotein, was used to bridge the cell surface to gelatin (hydrolyzed collagen). 75 While this approach is currently used to form multicellular layers or spheroids,75,76 it is conceivable that this method could be translated to LbL encapsulation. A challenge with this approach is its obvious degradability; however, ECM-based films could serve as base layers to present important biological cues to the cells and facilitate the additional deposition of other more permanent layers.
To leverage biological recognition sites but improve stability, one group incorporated a cholesterol anchor and an acrylate group within a pullulan nanogel system to generate coatings stabilized by both hydrophobic and covalent interactions. 77 Applying to beta-cell spheroids, this approach created stable coatings while conserving cell viability. Finally, in an approach that converges functional handles used in covalent LbL with cell surface labeling, Tomás et al integrated azido groups onto the cell surface using Bertozzi’s method of metabolic labeling.78,79 In this elegant approach, polymers expressing complementary functional handles “clicked” onto azido-labeled cells. While some loss of the polymer was observed over time, this approach can be combined with traditional covalent LbL methods to create durable coatings.
Bioactive Functionalization Strategies
A major limitation to CIT’s widespread adoption is the need for systemic immunosuppression to prevent allograft rejection. Further, despite aggressive antirejection regimens, islet grafts remain vulnerable to immunodestruction. The incorporation of immunomodulatory agents via islet surface engineering or linkage to nanoscale coatings can improve the distribution, bioavailability, and therapeutic power of immunomodulatory agents without impacting the graft volume or transplant site. Within the example of CIT, both the innate and adaptive immune responses play critical roles in poor islet engraftment and survival following intraportal transplantation and provide opportunities for therapeutic invention. 80
Anti-inflammatory Nanoscale Coatings
As highlighted earlier, IBMIR results in substantial islet loss.81,82 In order to reduce the deleterious effects of inflammation following blood-graft contact, bioactive moieties can be incorporated into nanoencapsulation strategies to not only provide steric hindrance and mask surface epitopes, but also alter the transplant microenvironment (Figure 2(a)). In one approach mimicking classic anticoagulant coatings, the islet surface can be heparinized. For example, Cabric et al exploited avidin’s affinity to both surface-bound biotin and macromolecular heparin. 83 Specifically, the islet surface was first biotinylated via sulfo-NHS-LC-biotin, followed by avidin, and then heparin. Using a porcine allotransplant coagulation model, heparinized islets displayed decreased intraluminal clotting compared to untreated control islets; however, murine syngeneic studies revealed no difference in blood glucose normalization from untreated islets. 83 In other approaches, islet surface heparinization has also been achieved by linking heparin to multi-branched PEG chains presented on the islet surface84,85 or 3,4-dihyrdoxyphenylalanine (DOPA), a mussel-derived cell-adhesive protein. 86 Heparin-coated islets exhibited decreased thrombogenicity 85 ; however, the impact of surface-bound heparin on delaying islet rejection in allo- and xenotransplantation studies was modest (eg, three days), if at all.84,86 Combining islet heparinization with low dose systemic immunosuppression (eg, FK506 or anti-CD154) extended this impact when compared to untreated islets, indicating a synergistic effect.84,86 Incorporating a different anti-inflammatory agent, Luan et al sought to inhibit complement activation through surface functionalization of soluble complement receptor 1 (sCR1). 87 Thiolated sCR1 was bound to the islet surface via MAL-PEG-lipid, with the verification of bioactivity in vitro. The co-immobilization of both sCR1 and heparin resulted in enhanced benefits, with the prevention of blood clot formation and fibrin deposition following intrahepatic infusion and improvements in graft efficacy within syngeneic C57BL/6J diabetic mice when compared to untreated islets. 88 Thrombomodulin, a transmembrane protein that binds and inactivates thrombin, is another potent anticoagulant applied to islet surface engineering. Using a recombinant thrombomodulin, Chaikof’s group linked this agent to the islet surface via azido and biotin-based approaches, with the retention of agent bioactivity.89,90 Alternatively, Chang et al covalently modified the islet surface using TAK-242, a toll-like receptor 4 (TLR4) antagonist pro-drug, that elutes drug upon linker hydrolysis. 91 Syngeneic kidney capsule transplant studies using a marginal IEQ demonstrated 100% graft survival compared to 0% survival of uncoated islets at four weeks. Overall, these anti-inflammatory islet surface modification approaches highlight the potential of ex vivo modification to protect the infused cells and reduce islet mass requirements.
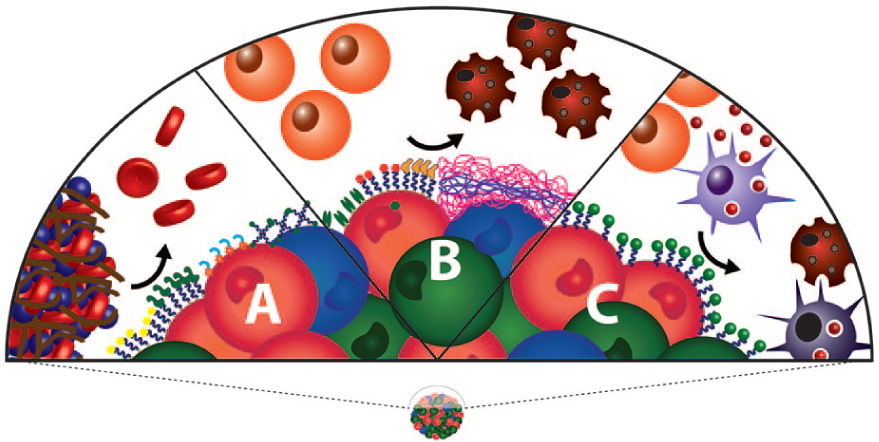
Functionalization of bioactive nanoscale agents to the islet surface can modulate undesirable host responses. (a) Anti-inflammatory coatings can inhibit clot formation and dampen IBMIR. (b) Presentation of adaptive immunomodulatory agents can inhibit T cell proliferation and/or induce cell death. (c) Nanoparticles, delivered freely or bound to the islet surface, can modulate innate and adaptive immune responses toward suppressive or tolerogenic pathways.
Immunomodulatory Nanoscale Coatings
Another major consideration with islet transplantation for treatment of T1D is reoccurrence of autoimmunity and targeted allorejection. In order to mitigate effector T cell graft destruction and promote long-term survival, surface engineering strategies have been explored to create a tolerogenic transplant microenvironment (Figure 2(b)). Yolcu et al surface engineered islets with a chimeric streptavidin-Fas ligand (SA-FasL) to instruct local immune cells.92,93 Fas/FasL-mediated apoptosis plays an important role in control of the T cell response to self-antigens, for Fas is expressed on T cells following activation. Subsequent to islet biotinylation and SA-FasL surface modification, murine allogeneic kidney capsule studies demonstrated localized tolerance, with the homing of regulatory T cells (Tregs) to the graft site and improved graft survival; this tolerogenic effect was greatly enhanced with the addition of short-course rapamycin. 93 In a similar approach, jagged-1 (JAG-1), a cell surface ligand that activates the Notch signaling pathway, was immobilized on the islet surface to tune the transplant microenvironment through Treg induction. 94 Islets expressing JAG-1 via surface PEGylation increased the generation of T regulatory cells when compared to untreated islets, albeit modestly (5% vs 1% T regulatory cells for JAG-1 coated vs uncoated islets, respectively). Implantation of modified rat islets into diabetic mice indicated function, but the pilot study needs to be expanded past six days post-transplant. 94 Cells can also be immobilized on the islet surface to promote graft tolerance. For example, peripheral blood-derived Tregs can be immobilized onto the islet surface to provide localized immunomodulation without impairing islet viability or functionality.95,96 Sertoli cells, which create an immunoprivileged environment in the testis, have also been conjugated onto the surface islets using a single stranded oligonucleotide-PEG-lipid liker. Islet functionality was maintained and, when transfused into liver of a mouse model, the Sertoli cells remained colocalized to the islets. 97
In addition to cell surface engineering, polymers used to generate nanoscale coatings have also been leveraged to modulate immune responses. As described earlier, LbL coatings generated using tannic acid and PVPON can not only impart a polymeric barrier, but also scavenge oxidants. With tannic acid as a natural antioxidant, several recent publications have illustrated the capacity of these coatings to modulate both APC activation as well as T cell recruitment and cytokine release.73,74 While the validation of several of these approaches is needed in vivo, these approaches clearly illustrate the capacity of immunomodulatory surfaces to locally direct host responses toward suppressive phenotypes.
Nanoparticle-based Approaches in T1D
Nanoparticles have significant potential in biomedical applications. With nanoscale control of physical and chemical properties, the pharmacokinetic features of nanoparticles, such as solubility, avidity, blood circulation half-life, and cellular targeting and trafficking, can be distinctly manipulated. For controlled drug delivery, nanoparticles serve as ideal carriers for poorly soluble drugs and can be tailored for extracellular or intracellular drug release. Their high surface area-to-volume ratio results in elevated potency, when compared to micro- or macrocarriers. Finally, the nanoscale format permits unique in vivo delivery, with the feasibility of both intravenous delivery and subcutaneous delivery with draining to local lymph nodes via interstitial flow.98,99
Nanoparticles can be synthesized from various materials, including inorganic metals, polymers, lipids, and ceramics, with variable compositions imparting distinct bioactive properties. The translation of nanoparticle-based approaches in the clinic has been widespread with applications in cancer, anemia, imaging, vaccinations, anesthetics, and immunotherapy. 100 For T1D, the clinical application of nanoparticles has traditionally been in exogenous insulin delivery, with nanoformulations serving to extend release or to facilitate oral delivery.101-104 Beyond exogenous insulin therapy, nanoparticles can serve as useful tools for bioactive modulation of the islet transplant environment.
Immunomodulatory Nanoparticles
As noted in earlier sections, innate and adaptive immune responses to the foreign cellular graft quickly result in the rejection of the islet transplant. While immunoisolation and bioactive surface functionalization provide important tools to mitigate this impact, coupling these approaches with immunomodulatory nanoparticles may provide further protection or tolerance induction (Figure 2(c)). Nanoparticle-based immunomodulatory approaches typically serve as drug-delivery depots, although they can also be surface functionalized for targeting or cellular instruction.
Nanoparticles can be used to deliver immunosuppressive cargo to immune cells to dampen effector cell function or induce a more tolerogenic phenotype. Due to their scale, nanoparticles are easily phagocytosed by professional APC, 105 although particles can be coated with targeting agents, such as anti-CD11c, for targeting specific phagocytic immune cells, such as dendritic cells. 106 For binding to nonphagocytic immune cells, nanoparticles can be decorated with specific binding agents. 107 Once the particle locates the targeted immune cell, their immunomodulatory cargo can be released. In one approach, poly(lactic-co-glycolic) acid (PLGA) nanoparticles were loaded with immunomodulatory cytokines, TGF-beta and IL-2, and coated with anti-CD4 for targeting CD4+ helper T cells. 107 The local delivery of these cytokines to CD4+ T cells resulted in the induction of a T regulatory phenotype. In another approach, a tolerogenic ligand, 2-(1′H-indole-3′-carbonyl)-thiazole-4-carboxylic acid methyl ester, was copresented with a beta-cell antigen, proinsulin, on the surface of gold nanoparticles in an effort to prevent beta-cell immune attack. 108 Testing in prediabetic mouse models of autoimmune diabetes, ie, nonobese diabetic, resulted in significant prevention of diabetes in treated animals when compared to untreated controls. 109 This approach could be useful in islet or stem-cell derived beta-cell transplantation as a means to prevent autoimmune attack of the new graft; however, additional studies are needed to evaluate targeting and toxicity in larger animal models. 110 In another approach, poly (lactide-co-glycolide) (PLG) nanoparticles were used as carriers for allo-antigens to promote tolerance to specific allogenic islets. 111 The immunization of diabetic mice with PLG nanoparticles containing allogeneic antigens from one mouse strain (Balb/c) before the allogeneic transplantation of Balb/c islets into another mouse strain (C57BL/6J) resulted in prolonged survival of the graft. While this approach may be difficult to translate to the current human islet transplant protocols due to the unpredictability of the donor HLA, the emergence of functional stem-cell derived beta-cells would permit for the immunization of the recipient to the donor HLA antigens prior to the delivery of the beta-cell graft.
Combining drug delivering nanoparticles with encapsulation should further elevate protection, as coatings prevent direct cell attack and the local release of immunosuppressive or tolerogenic agents dampen indirectly activated immune cells. In one approach, tacrolimus-loaded PLGA nanoparticles were coated with DOPA and self-assembled onto the islet surface. 112 While the efficacy of immunosuppression in a xenograft islet transplant mouse model was not durable (only ten-day delayed rejection), the approach could be scaled up to expand to other drugs or the dosage of the nanoparticles could be increased. In a similar approach, leukemia inhibitory factor (LIF)-loaded PLGA nanoparticles were linked to PEGylated islets. 113 Resulting LIF-coated islets were significantly protected from allograft rejection in a murine model. 113 These results highlight the potential to combine nanoparticles and nanoscale coatings to further elevate protection without introducing significant volume to the transplant.
Antioxidant Nanoparticles
Reactive oxygen species is a natural by-product of glucose metabolism. Under hyperglycemia, however, ROS is overproduced. 114 When cell-derived antioxidants are unable to accommodate these elevated ROS levels, oxidative stress arises. Oxidative stress damages cellular components and activates immunological pathways, resulting in broad tissue damage114,115 and the initiation of inflammation in various innate/adaptive immune cells.116,117 As it relates to T1D cell therapy, ROS impacts multiple areas, from cell procurement to transplant engraftment and immune responses. 118 During pancreatic organ transport, islet isolation, and cell culture, ROS-mediated damage is evident.119-121 As outlined previously, inflammatory responses following islet infusion, such as IBMIR, result in elevated ROS, which contributes to significant beta-cell damage and exacerbated immune responses to the graft.
Antioxidant nanoparticles provide a useful platform to locally mitigate ROS, during both isolation and transplantation. Antioxidant activity in these particles can be generated by the material itself, eg, cerium, yttrium, and zinc, 122 and/or by the incorporation of antioxidant agents onto the nanoparticle. 123 Antioxidant nanoparticles are particularly potent, when compared to other geometrical formats, as their surface redox properties per unit volume are exceptionally high. To add further utility to these particles, the nanoparticle surface can be functionalized to enhance targeting and/or provide additional bioactive features.
Cerium oxide, a rare-earth metal oxide, is a broadly used catalyst material. In nanoparticle form (CONP), surface oxygen vacancies impart redox properties, while the capacity of cerium to fluctuate within a +3 and +4 oxidative state provides a unique self-renewing property. CONP is a useful therapeutic for various biomedical applications, as it can be injected intravenously and target specific organs, tissues, and even cell compartments. 124 For islet transplantation, the addition of CONP to islet cultures resulted in the protection of beta-cells from ROS-mediated damage, with the addition of yttrium oxide nanoparticles boosting this effect125,126; however, cellular internalization of CONP can impart beta-cell toxicity.127,128 As an alternative, CONP can be integrated within encapsulating biomaterials to serve as a local antioxidant.127,129 In one approach, CONP was coated with dextran and immobilized within alginate microbeads, where the embedded CONP protected beta-cells from ambient ROS. 127 In another approach, nanoscale coatings of CONP and alginate were generated in a LbL manner. 129 The resulting ultrathin coatings scavenged externally generated ROS, providing protection from ROS-mediated insults to the underlying cells. 129 Overall, the high potential of this material to impart durable and ubiquitous antioxidant protection in cell culture studies supports the translation of these materials to preclinical models.
Zinc has long been known to inhibit free radical reactions 130 ; however, the translation of zinc oxide nanoparticles (ZON) to living cells is challenged by reports of ZON treatment increasing oxidative stress and cytotoxicity.131-133 Applications to pancreatic rat islets indicate a dose-dependent mechanism, with low-dose treatment resulting in improved metabolic activity and elevated basal and stimulatory insulin release. 134 Furthermore, the systemic delivery of ZON in rodents resulted in protection from chemically induced diabetes 135 ; boosting ZON with silver nanoparticles elevated this protection. 136 In addition to an antioxidant effect, ZON may also play a role in resolving impaired insulin signaling in diabetes via the deactivation of phosphorylation protein tyrosine phosphatase 1B, an inhibitor of insulin signaling, and the activation of protein kinase B, an essential mediator of insulin signaling. 135 Modification of ZON synthesis using biogenic approaches may also elevate their inherent antioxidant capacity.137,138
Gold nanoparticles (AuNPs) are widely used in biomedical diagnostics and therapy, owing to their malleable optical and electronic features and ease of surface functionalization. 139 They have been used as inert carriers of antioxidant materials, such as vitamin E analogs, 140 catechin, 141 and curcumin. 142 Biogenic approaches for generating AuNP can also be leveraged to introduce antioxidant features. Specifically, antioxidant plant extracts or microbes can be used as reducing agents to generate AuNP, with the resulting particles exhibiting unique antioxidant properties.143-146 While in early stages, treatment of diabetic rodents with biogenic AuNP resulted in decreased blood glucose and decreased serum levels of proinflammatory cytokines TNF-α and IL-6. 143 Another study using a different biogenic AuNP formulation measured increased antioxidant defense mechanisms and saw decreased oxidative organ injury for AuNP-treated diabetic rats compared to untreated controls. 144 With promising results in modulating systemic ROS to mitigate chemically induced diabetes in rodents, translation of AuNP to islet cell therapy is well supported.
In addition to metal-based nanoparticles, polymer materials can be leveraged to deliver an antioxidant payload at a targeted site. In one approach, chitosan nanoparticles were loaded with an antioxidant agent, stevia rebaudiana. 147 Systemic delivery of these particles into streptozotocin (STZ)-diabetic mice alleviated oxidative stress, resulting in decreased hyperglycemia and STZ-induced organ toxicity. 147 In another approach, bilirubin, an effective antioxidant and anti-inflammatory agent, was formulated using PEG-facilitated self-assembly. 148 Treatment of islets with PEG-bilirubin decreased oxidative stress in pancreatic islets and inflammation in lipopolysaccharide (LPS)-activated macrophages. Furthermore, PEG-bilirubin extended the efficacy of a xenograft transplant (rat islets into STZ-diabetic mice) by over ten days. 148 This approach highlights the importance of mitigating oxidative stress, not only to preserve islet viability, but also to modulate immune signaling.
Conclusion
Innovative approaches that address islet donor scarcity, requisite systemic immunosuppression, and the poor engraftment associated with clinical islet transplantation would result in a profound impact in T1D therapy. With a focus on mitigating immune-mediated destruction through both direct and indirect pathways, nanotechnology approaches seek to modulate immune responses with unique features of therapeutic localization, elegant fabrication control, and increased therapeutic power without generating large transplant volumes or diffusional barriers.
Nanoencapsulation via cell surface modification provides immunoprotection and conceals surface antigens without increasing graft volume. Islet PEGylation is able to mitigate IBMIR through reduced protein adsorption and can be achieved through either covalent bonding or hydrophobic interactions with moieties innately present on the cell surface. The challenge presented with islet PEGylation is to develop a nanoencapsulation platform that both maintains membrane integrity and is durable despite membrane turnover. Layer-by-layer assembled nanofilms offer a more tunable and stable coating platform, with polycation cytotoxicity as a major constraint. To date, passive immunoprotection alone has been unable to support durable cell protection, but rather the synergistic effect of nanoencapsulation and short-course immunotherapy is able to achieve long-term graft survival. Moreover, steric immunoprotection is a promising strategy to expand the feasibility of alternative beta-cell sources, such as xenografts and stem cell-derived beta-cells. Moving forward, the host response to cell surface engineering strategies needs to be comprehensively characterized. Both in vivo monitoring and postretrieval assessment of the surface-engineered graft and infiltrating cell phenotypes will lead to insight into immune recognition of these unique transplants. This will guide the generation of more stable and protective coatings capable of promoting long-term graft survival. Additionally, larger animal studies are needed to fully evaluate the potential of nanoscale encapsulation as a primary or adjunct immunomodulatory agent.
Immunomodulation can also be accomplished through bioactive functionalization of the islet surface. By intelligently instructing a suppressive transplant microenvironment through innate and/or adaptive immune response mitigation, adverse off-target side effects can be avoided. Further examination of the in vivo efficacy and durability of cell surface immobilized bioactive moieties needs to be conducted.
Additionally, the incorporation of nanoparticles into the transplant system can prevent graft immunodestruction through bioactive modulation. Antioxidant and therapeutic-loaded nanoparticles have the ability to dampen the immune response and create a tolerogenic microenvironment, respectively, and can easily be integrated into nanoscale coatings to enhance graft protection without increasing graft volume. A potential problem with nanoparticle-incorporated nanoencapsulation platforms is long-term particle localization. If the polymeric coating was to dissociate, nanoparticles may enter the circulation and accumulate in the unwanted sites.
Footnotes
Acknowledgements
The authors are grateful for funding from the US National Institutes of Health grants DK104208, DK100654, and DK108736, as well as from JDRF grants 3-SRA-2017-347-M-B and 3-SRA-2018-683-S-B.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the US National Institutes of Health grants DK104208, DK100654, and DK108736, as well as from JDRF grants 3-SRA-2017-347-M-B and 3-SRA-2018-683-S-B.