
Abstract
Introduction:
Pancreas transplantation is currently one of the best treatments proposed in highly selected patients with unstable and brittle type 1 diabetes. The objective of pancreas transplantation is to restore normoglycemia and avoid the occurrence of complications associated with diabetes. Graft pancreatitis and thrombosis, arising from ischemia reperfusion injuries, are major causes of graft loss in the postoperative period. Ex situ perfusion, in hypothermic or normothermic settings, allowed to improve ischemic reperfusion injury in other organ transplantations (kidney, liver, or lung). The development of pancreatic graft perfusion techniques would limit these ischemic reperfusion injuries.
Objective:
Evaluation of the safety and feasibility of ex situ perfusion of pancreas for whole-organ transplantation.
Methods:
English literature about pancreas perfusion was analyzed using electronic database Medline via PubMed (1950-2018). Exclusion criteria were studies that did not specify the technical aspects of machine perfusion and studies focused only on pancreas perfusion for islet isolation.
Results:
Hypothermic machine perfusion for pancreas preservation has been evaluated in nine studies and normothermic machine perfusion in ten studies. We evaluated machine perfusion model, types of experimental model, anatomy, perfusion parameters, flushing and perfusion solution, length of perfusion, and comparison between static cold storage and perfusion.
Conclusions:
This review compared ex vivo machine perfusion of experimental pancreas for whole-organ transplantation. Pancreas perfusion is feasible and could be a helpful tool to evaluate pancreas prior to transplantation. Pancreas perfusion (in hypothermic or normothermic settings) could reduce ischemic reperfusion injuries, and maybe could avoid pancreas thrombosis and reduce morbidity of pancreas transplantation.
Keywords
Introduction
Pancreas transplantation is currently one of the best treatments proposed in highly selected patients with unstable and brittle type 1 diabetes. In 2015, 30.3 million Americans (9.4% of the population) presented diabetes and diabetes was the seventh leading cause of death in the United States, with 79 535 deaths. Approximately 1.25 million American children and adults suffer from type 1 diabetes. 1 The objective of pancreas transplantation is to restore insulin secretion, thus avoiding life-threatening hypoglycemia and limit the progression of macro- and micro-angiopathic complications. Simultaneous pancreas and kidney transplantations are commonly performed in selected patients with diabetic nephropathy and chronic renal dysfunction.
Improvement of surgical procedures and postoperative management has strongly reduced the morbidity and mortality of pancreas transplantation.2,3 Recent data from UNOS (2010-2014) showed three-year graft survival rates of 82.2% for pancreas graft among simultaneous pancreas and kidney transplant recipients, 75.4% for pancreas after kidney, and 73.3% for pancreas transplantation alone in the United States. 4 Whereas long-term outcomes have improved, graft losses during the first year (early graft failure) remained stable, between 10% and 15%. Graft pancreatitis and thrombosis are major causes of graft loss in the postoperative period, and these complications can occur in 25%-50% of cases.5,6 Despite strong evidence for the implication of ischemia reperfusion injury in the occurrence of these complications, there has been no major improvement of pancreas transplant preservation technique. Standard method for human pancreas preservation is hypothermic preservation by static cold storage (SCS) for a limited period of time, usually less than 20 hours. 7 Furthermore, there is no tool to evaluate pancreas viability before transplantation, except visual macroscopic evaluation.
Moreover, organ shortage and the growing demand for organs prompt clinicians to expand the donor pool by including extended criteria donors (ECD).8,9 In kidney transplantation, the use of machine perfusion, in hypothermic or normothermic settings, has beneficial effects in term of delayed graft function and primary nonfunction, for transplant from ECD and/or donation from cardiac death (DCD). 10 These techniques to preserve and perfuse organs in hypothermic and normothermic settings have been developed in liver, heart, and lung models also.
Improvement of early graft survival is a major issue in pancreas transplantation. Pancreas preservation appears to be critical to prevent thrombosis and reperfusion pancreatitis. Similarly to other organs, pancreas perfusion before transplantation may improve graft survival and could be useful to evaluate the organ. The development of pancreas transplantation is linked to the improvement of pancreatic graft perfusion techniques. Very few studies have focused on hypothermic pulsatile perfusion for pancreas preservation. The main objective of these experiments was not to transplant the organ but to isolate Langerhans islets.11-13
The objective of this literature review is to evaluate the safety and feasibility of ex situ pancreas perfusion for whole-organ transplantation.
Methods
English literature about perfusion of pancreas was realized using electronic database Medline via PubMed (1950-2018).
Key terms used included “pancreas perfusion,” “pancreas preservation,” “normothermic pancreas perfusion,” “hypothermic pancreas perfusion,” and “ex vivo pancreas perfusion.”
Exclusion criteria were studies that did not specify the technical aspects of machine perfusion and studies focused only on pancreas perfusion for islet isolation. Review articles were screened for their references for further relevant studies. References in the identified articles were used to identify more relevant studies. The literature search was performed independently by two authors (TP, JB) and results were crosschecked. Data from included studies were extracted by the primary author (TP) (Figure 1).
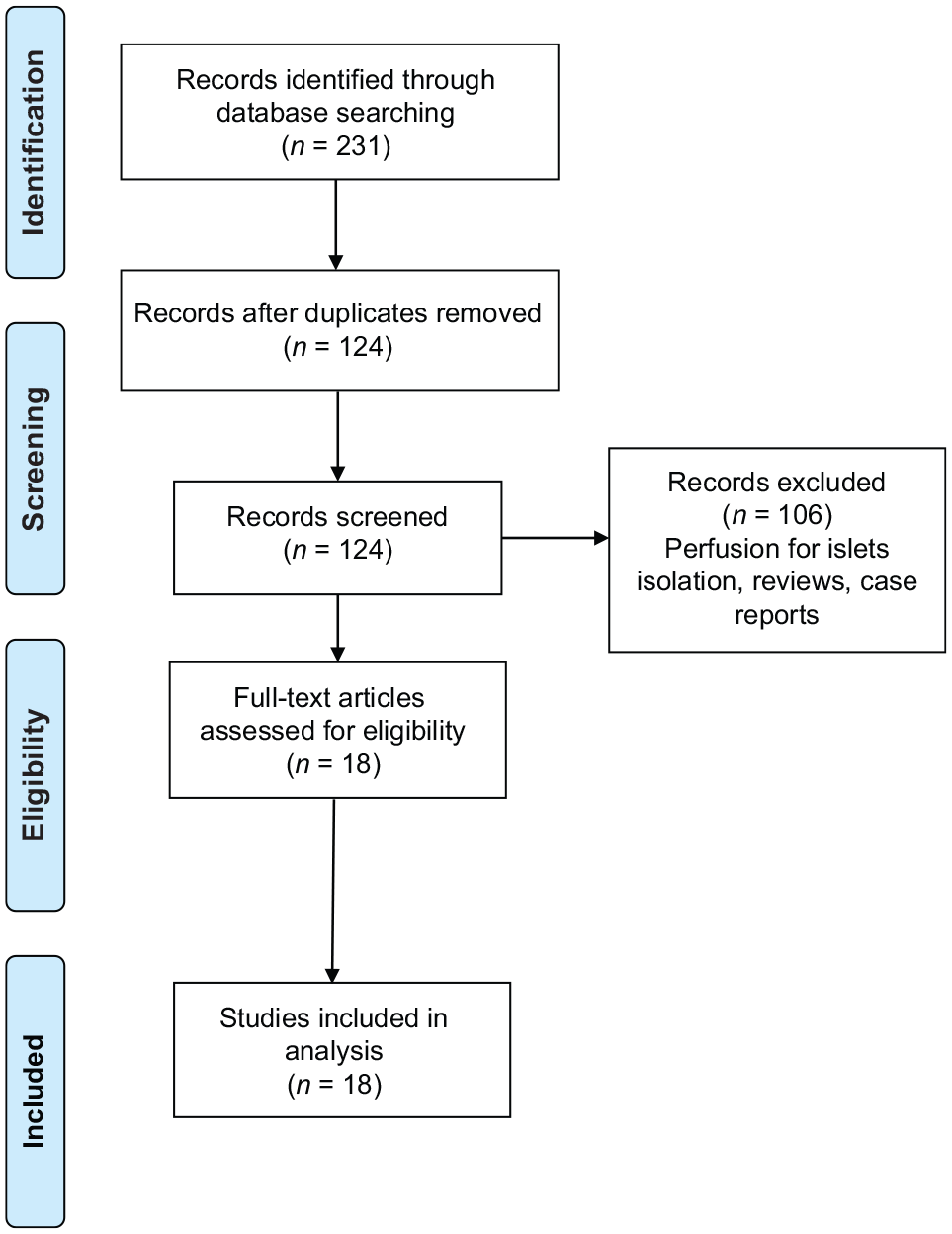
PRISMA flow diagram.
Results
Hypothermic machine perfusion for pancreas preservation was evaluated in nine studies and normothermic machine perfusion in ten studies. Hamaoui et al 14 evaluated both hypothermic and normothermic perfusion.
Hypothermic Pancreas Perfusion
The summary of the experimental hypothermic perfusion of human and animals’ pancreas studies is summarized in Tables 1 and 2.
Experimental Hypothermic Perfusion of Human Pancreas Studies.
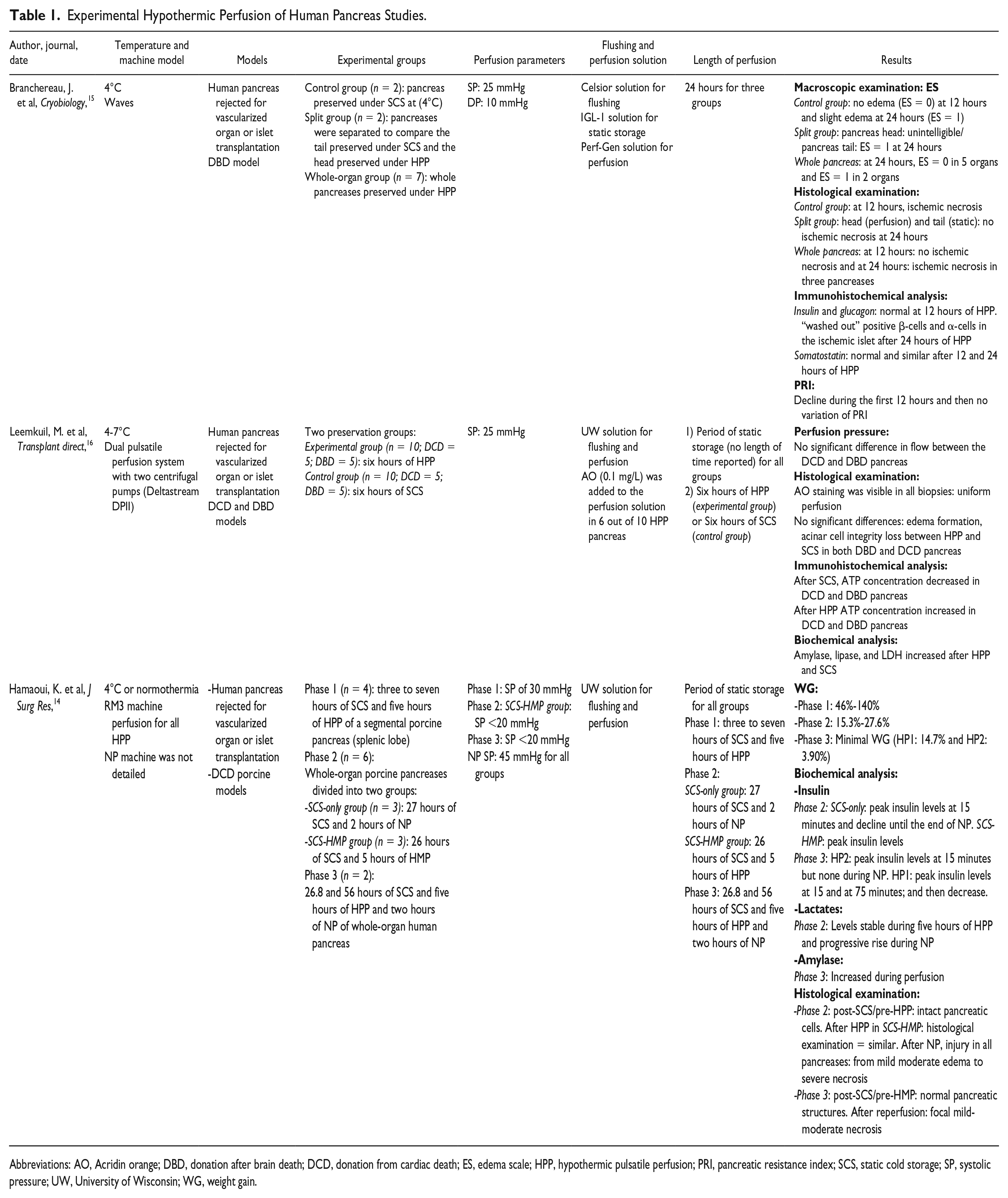
Abbreviations: AO, Acridin orange; DBD, donation after brain death; DCD, donation from cardiac death; ES, edema scale; HPP, hypothermic pulsatile perfusion; PRI, pancreatic resistance index; SCS, static cold storage; SP, systolic pressure; UW, University of Wisconsin; WG, weight gain.
Experimental Hypothermic Perfusion of Animals’ Pancreas Studies.
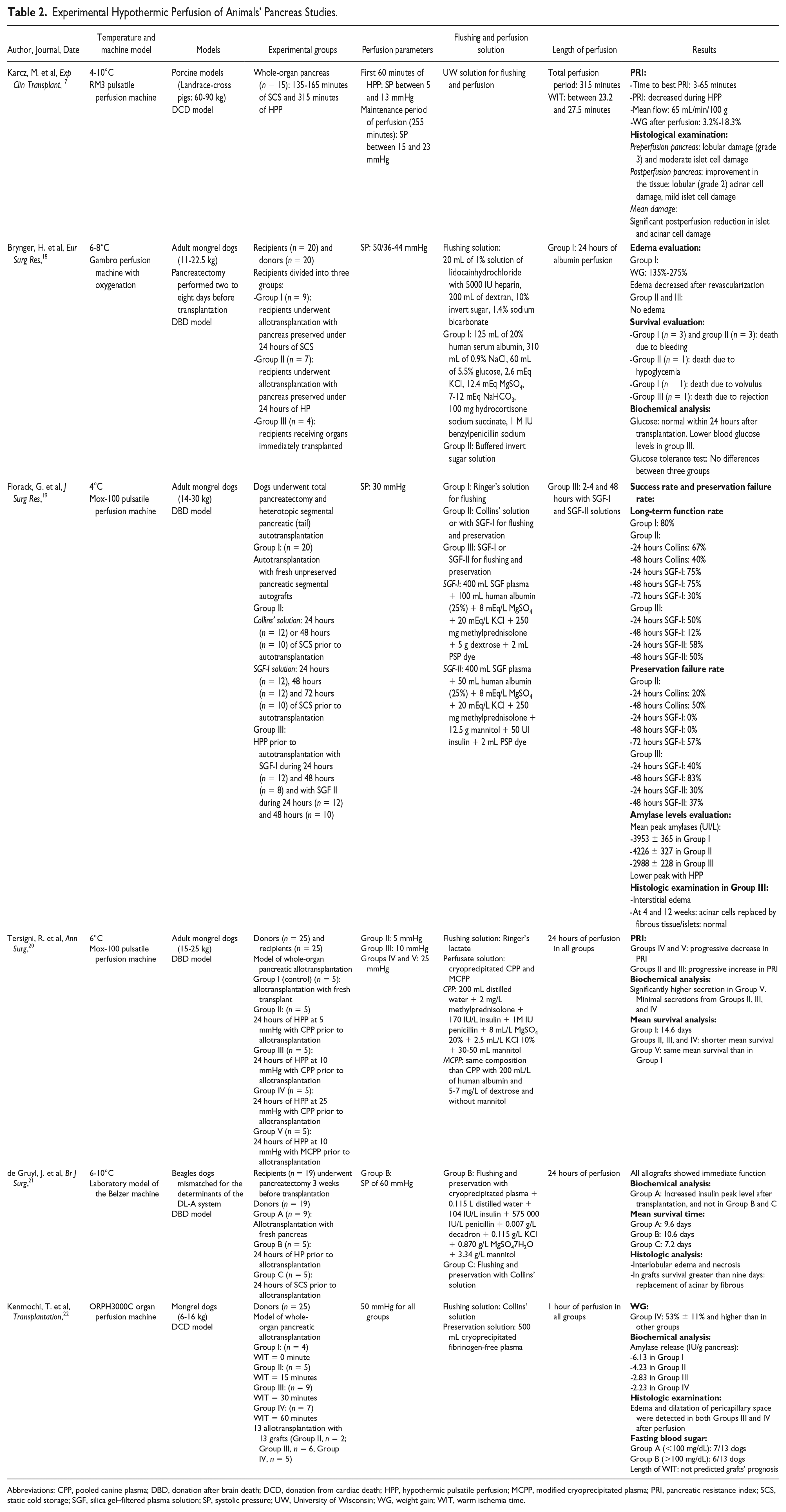
Abbreviations: CPP, pooled canine plasma; DBD, donation after brain death; DCD, donation from cardiac death; HPP, hypothermic pulsatile perfusion; MCPP, modified cryoprecipitated plasma; PRI, pancreatic resistance index; SCS, static cold storage; SGF, silica gel–filtered plasma solution; SP, systolic pressure; UW, University of Wisconsin; WG, weight gain; WIT, warm ischemia time.
Human experimental hypothermic pancreas perfusion studies
Branchereau et al, 15 Leemkuil et al, 16 and Hamaoui et al 14 reported human experimental hypothermic perfusion studies.
Branchereau et al 15 used human pancreas rejected for vascularized organ or islet transplantation. They compared three groups: control group (n = 3) with whole-organ pancreases preserved under conventional SCS during 24 hours; split group (n = 2) with pancreases separated in order to compare the tail, preserved under SCS during 24 hours, and the head, preserved under hypothermic pulsatile perfusion (HPP) during 24 hours and the whole-organ group (n = 7) with whole-organ pancreases preserved under HPP during 24 hours. The HPP machine was a Waves machine perfusion. The systolic pressure (SP) was 25 mmHg in all groups. The SCS solution was IGL-1 and the HP solution was Perfgen. Concerning macroscopic examination, with edema scale, they reported no edema at 12 hours and slight edema at 24 hours in the control group. In the split group, slight edema occurred at the head of the pancreas after 24 hours. In the whole pancreas group, after 24 hours of HP, no edema occurred in five pancreases and two transplants presented slight edema. Concerning histological examination, in the control group, after 12 hours, multiple ischemic necrosis occurred. In the split group, no ischemic necrosis occurred, after 24 hours, in the head and the tail of the pancreases. In the whole-organ group, after 12 hours, no ischemic necrosis occurred and after 24 hours, ischemic necrosis was present in three pancreases. Concerning immunohistochemical analysis, insulin and glucagon concentration was normal at 12 hours of HP. At 24 hours of HPP, a “washed out” positive β-cells and α-cells in the ischemic islet occurred. Somatostatin concentration was normal after 12 and 24 hours of HPP. Concerning pancreatic resistance index (PRI), during the first 12 hours, PRI declined and then no variation was reported.
Leemkuil et al 16 compared six hours of SCS (n = 10) and six hours of HPP (n = 10) of human pancreases rejected for vascularized organ or islet transplantation. They had both DCD and donation after brain death (DBD) pancreases. The HPP machine was a dual pulsatile perfusion system (Deltastream). The SP was 25 mmHg in all groups. The SCS and HPP solution was UW and they added Acridin orange, in the solution, to evaluate the perfusion. Concerning perfusion pressure, they reported no significant differences in flow between DCD and DBD pancreases. Concerning histological examination, they reported no significant differences in terms of edema formation, and acinar cell integrity loss between HPP and SCS in both DBD and DCD pancreases. Acridin orange staining was visible in all biopsies, confirming the uniform perfusion. Concerning immunohistochemical examination, after six hours of SCS, ATP concentration decreased in DCD and DBD pancreas, while, after six hours of HPP, ATP concentration increased in DCD and DBD pancreas. Concerning biochemical examination, amylase, lipase, and LDH increased after HPP and SCS.
Hamaoui et al 14 used both human pancreas rejected for vascularized organ or islet transplantation and DCD porcine pancreas. They compared three groups: phase 1 (n = 4) with segmental porcine pancreases (splenic lobe) preserved under HPP during five hours after a period of three to seven hours of SCS; phase 2 (n = 6): whole-organ porcine pancreases divided into two subgroups: SCS-only group (n = 3) with whole-organ porcine pancreases preserved under two hours of NP after 27 hours of SCS and SCS-HMP group (n = 3) with whole-organ porcine pancreases preserved under five hours of HPP after 26 hours of SCS; phase 3 (n = 2) with whole-organ human pancreas preserved under five hours of HPP and then two hours of NP after an initial period of 26.8 and 56 hours of SCS. The HPP machine was a RM3 and the NP machine was not detailed. The SP of HPP was 30 mmHg in phase 1, and <20 mmHg in SCS-HMP group (phase 2) and in phase 3. The SP of NP was 45 mmHg in all groups. The SCS and HPP solution was UW. The warm ischemia time (WIT) in phase 1 and 2 were 30-55 and 30 minutes. The WG was lower in phase 3 (HP1: 14.7% and HP2: 3.9% versus 46%-140% in phase 1 and 15.3%-27.6% in phase 2). Concerning biochemical analysis, both phase 2 and phase 3 pancreases presented peak insulin levels after the beginning of the HPP. In phase 2, lactates levels remained stable during HPP and raised during NP. In phase 3, amylase levels increased during HPP and NP. Concerning histological examination, in phase 2, after 27 and 26 hours of SCS, no pancreatic cell damages occurred. After HPP, no pancreatic cell damages were reported while after NP, moderate edema to severe necrosis was reported. In phase 3, after 26.8 and 56 hours of SCS, a normal pancreatic structure was reported. After HPP and NP, moderate necrosis occurred.
Animal experimental hypothermic pancreas perfusion studies
Machine perfusion system
Different types of machine perfusion were used: RM3 Machine Perfusion Unit (Waters Medical Systems, Rochester, MN, USA),14,17 Gambro perfusion system with oxygenator, 18 Mox-100 machine perfusion (Waters Medical System, Rochester, MN, USA),19,20 ORPH3000C organ perfusion machine (Senko Medical Mfg. Co., Tokyo, Japan), 22 and an experimental model of Belzer machine. 21
Experimental models
Experimental models were porcine in one study, 17 mongrel dog in four studies,18-20,22 and bagel dog in one study. 21 Five studies were conducted with DBD model, and four studies with DCD model.
Perfusion parameters
Karcz et al 17 perfused porcine pancreas at an SP between 15 and 23 mmHg. They reported minimal WG and an improvement in histologic islet and acinar cell damages after 315 minutes of perfusion. Higher SP (50/36-44 mmHg) was used by Brynger et al. WG was more important in these dogs’ pancreases (135%-275%). 18 Florack et al 19 reported that use of high SP (45 and 60 mmHg) of dogs’ pancreases resulted in severe edema. At 30 mmHg, all grafts developed interstitial edema during perfusion (at 24 hours and more important at 48 hours). Tersigni et al 20 compared SP of 5-10 and 25 mmHg in dogs’ pancreases. Pancreatic secretions increased in pancreases perfused at SP of 25 mmHg. de Gruyl et al and Kenmochi et al21,22 perfused dogs’ pancreases with high SP (60 and 50 mmHg). They reported an immediate function 21 and a minimal weight gain with edema. 22
Flushing and perfusion solution
Karcz et al 17 used University of Wisconsin solution for perfusion of porcine pancreases. Brynger et al 18 developed an experimental perfusion solution with albumin, NaCl, glucose, KCl, MgSO4, NaHCO3, hydrocortisone sodium succinate, and benzylpenicillin. Likewise, Florack et al 19 developed an experimental perfusion solution (Silica Gel-Filtered plasma solution: SGF-I and SGF-II). SGF-I contained plasma, human albumin, MgSO4, KCl, methylprednisolone, dextrose, and PSP dye. SGF-II had the same composition as SGF-I with adjunction of mannitol and insulin. Tersigni et al 20 used experimental pooled canine plasma (CPP) and modified cryoprecipitated plasma (MCPP) perfusion solution. CPP contained water, methylprednisolone, insulin, penicillin, MgSO4, KCl, and mannitol. MCPP had the same composition as CPP with human albumin and dextrose and without mannitol. Pancreatic secretions (amylase, trypsin, and lactic acid) were significantly higher in pancreases perfused with MCPP. These pancreases presented less edema. de Gruyl et al 21 used an experimental (plasma, water, insulin, penicillin, decadron, KCl, MgSO47H2O, and mannitol) solution in Beagles dog model. The mean survival of dogs’ recipients was longer with grafts preserved under hypothermic perfusion using experimental solution (10.6 days versus 7.2 days).
Length of perfusion
Florack et al 19 compared 24 and 48 hours of perfusion in a dog model. They reported a long-term function rate of 50%, 58%, 12%, and 50% in groups perfused during 24 hours with SGF-I, 24 hours with SGF-II, 48 hours with SGF-I, and 48 hours avec SGF-II, respectively. The preservation failure rate was 40%, 30%, 83%, and 37% in groups perfused during 24 hours with SGF-I, 24 hours with SGF-II, 48 hours with SGF-I, and 48 hours avec SGF-II, respectively. Kenmochi et al 22 compared different warm ischemia time (0, 15, 30, and 60 minutes) prior to 1 hour of HP in dog models. Long warm ischemia period was correlated with higher WG and more severe histologic lesions.
Pancreas transplantation
Brynger et al and Tersigni et al reported dogs pancreases allotransplantation experiences.18,20 Brynger et al compared dogs pancreases allotransplantation after 24 hours of perfusion with albumin or buffered sugar solution, in hypothermic conditions. 18 Tersigni et al compared pancreases allotransplantation after 24 hours of HP, at different SP values: 5, 10, and 25 mmHg, in dog models. Mean survival time was shorter for recipients transplanted with pancreases preserved in HP compared to recipients transplanted with fresh transplant without perfusion. 20 Florack et al published a model of dog’s pancreases autotransplantation. They compared pancreases autotransplantation, after 24 and 48 hours of HP or SCS of grafts. Long-term function rate was 75% after 24 hours of SCS and 50% after 24 hours of HP. After 48 hours of SCS, long-term function rate was 75%, and 12% after 48 hours of HP. 19 de Gruyl et al compared pancreas allotransplantation, in dog models, after 24 hours of HP or 24 hours of SCS. Mean survival time was longer for recipients transplanted with grafts preserved with HP (10.6 days versus 7.2 days). 21 Kenmochi et al compared pancreas allotransplantation, of grafts with different WIT (0, 15, 30, and 60 minutes), prior to one hour of HP. Grafts pancreases with long WIT (30 and 60 minutes) presented edema after one hour of perfusion. 22
Normothermic Pancreas Perfusion
The summary of the experimental normothermic perfusion of human and animals’ pancreas studies is presented in Tables 3 and 4.
Experimental Normothermic Perfusion of Human Pancreas Studies.
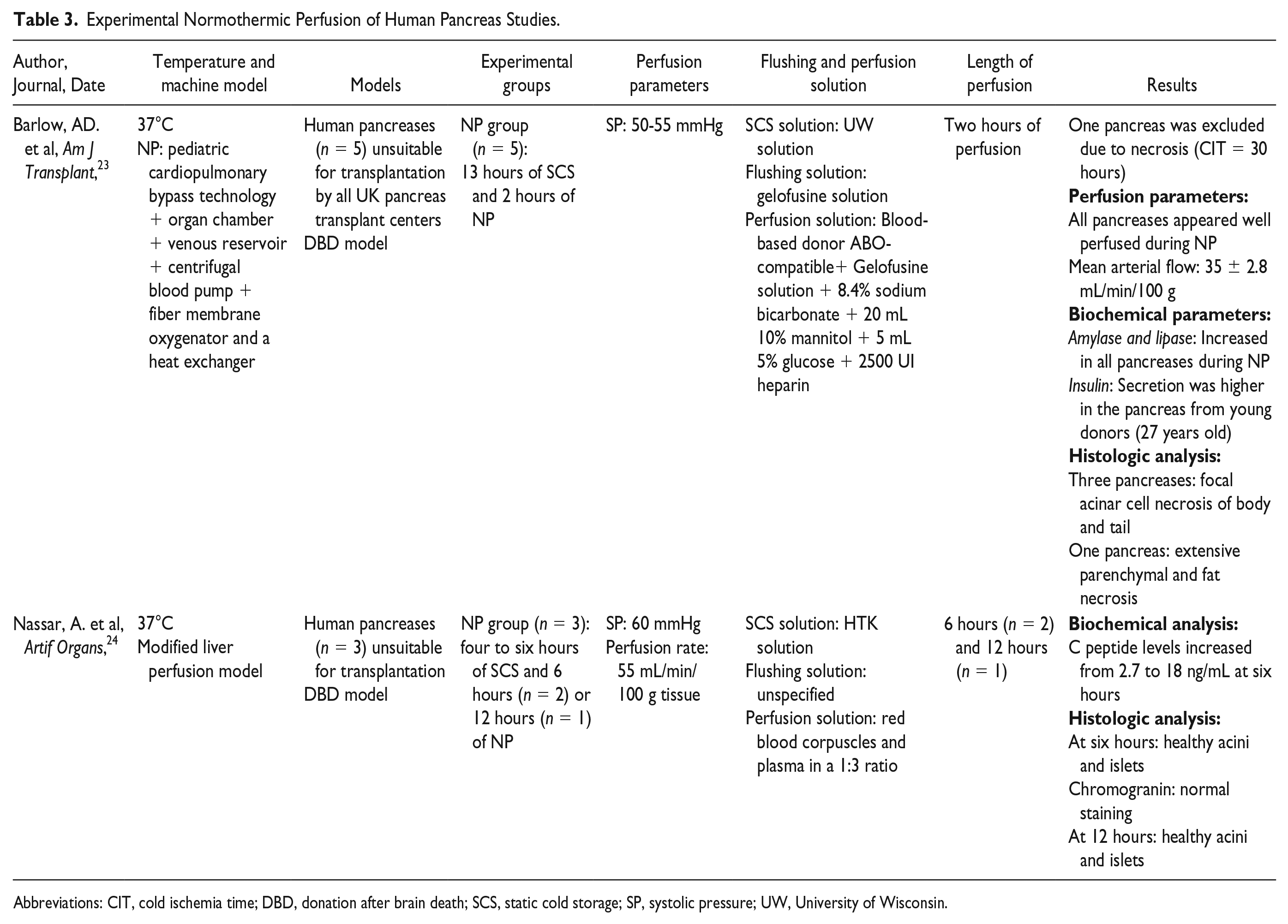
Abbreviations: CIT, cold ischemia time; DBD, donation after brain death; SCS, static cold storage; SP, systolic pressure; UW, University of Wisconsin.
Experimental Normothermic Perfusion of Animals’ Pancreas Studies.
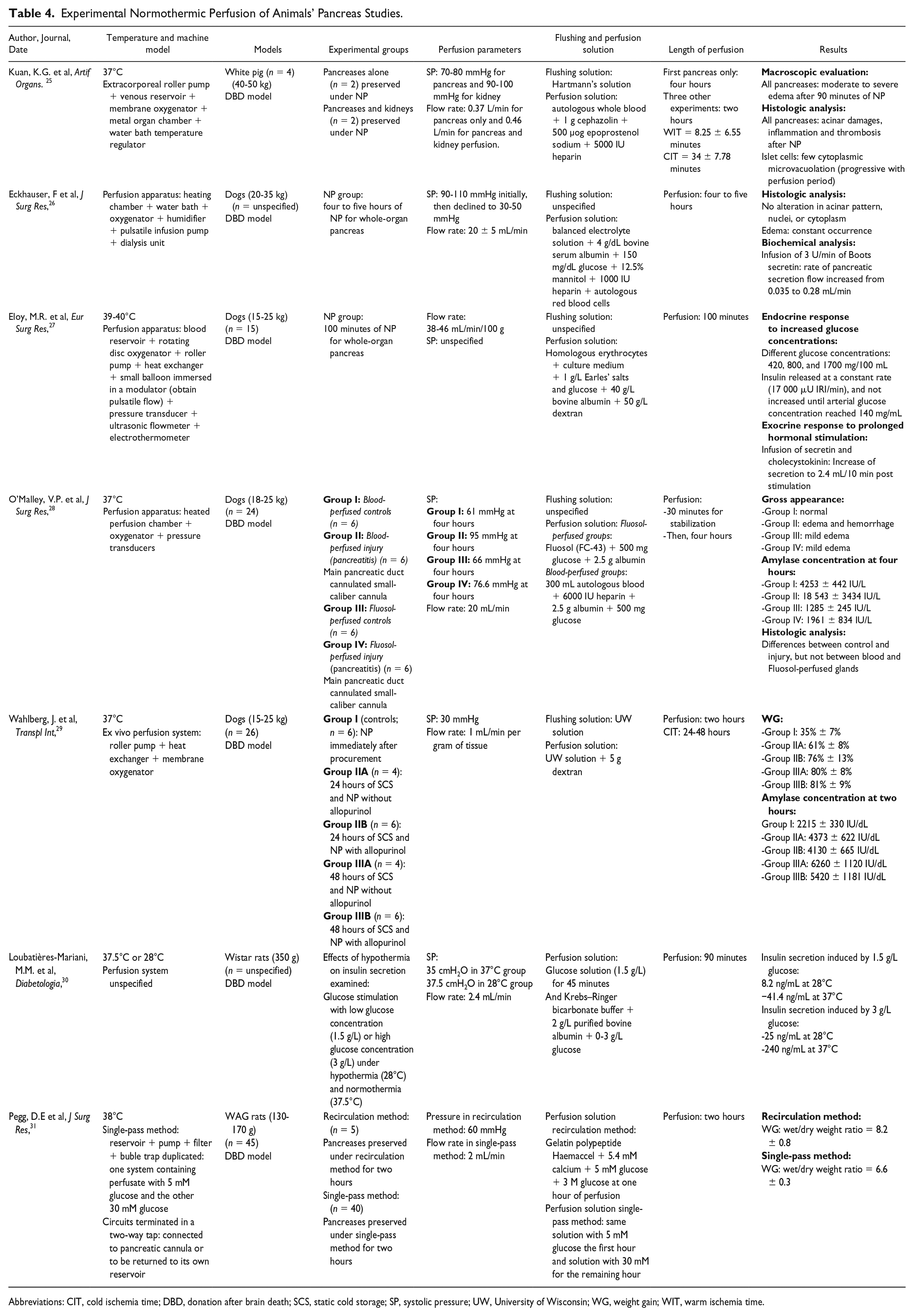
Abbreviations: CIT, cold ischemia time; DBD, donation after brain death; SCS, static cold storage; SP, systolic pressure; UW, University of Wisconsin; WG, weight gain; WIT, warm ischemia time.
Human experimental normothermic pancreas perfusion studies
Barlow et al 23 and Nassar et al 24 reported human experimental normothermic perfusion studies.
Barlow et al evaluated the impact of 13 hours of SCS followed by 2-hour NP in human pancreases (n = 5) unsuitable for transplantation. They used a pediatric cardiopulmonary bypass technology with organ chamber, venous reservoir, centrifugal blood pump, and a heat exchanger. The SP was 50-55 mmHg. They used UW as SCS solution, gelofusine as flushing solution, and a typical NP solution (blood-based donor ABO-compatible, gelofusine, sodium bicarbonate, mannitol, glucose, and heparin) as perfusion solution. One pancreas was excluded due to prolonged cold ischemia time (CIT; 30 hours). They reported a good perfusion during NP, with a mean arterial flow of 35 ± 2.8 mL/min/100 g. Concerning biochemical parameters, amylase and lipase levels increased in all pancreases during NP. Insulin secretion was higher in the pancreas from young donors (27 years old). Concerning histologic analysis, three pancreases presented focal acinar cell necrosis of the body and the tail and one pancreas presented extensive parenchymal and fat necrosis.
Nassar et al evaluated the impact of 4-6 hours of SCS followed by 6 hours (n = 2) or 12 hours (n = 1) of NP in human, pancreases unsuitable for transplantation. They used a modified liver perfusion model. The SP was 60 mmHg, with a perfusion rate of 55 mL/min/100 g. They employed HTK as SCS solution and a perfusion solution containing red blood corpuscles and plasma. Concerning biochemical analysis, C-peptide levels increased from 2.7 to 18 ng/mL at six hours. Concerning histologic analysis, at 6 and 12 hours of NP, they reported healthy acini and islets.
Animal experimental normothermic pancreas perfusion studies
Machine perfusion system
The first experimental normothermic pancreas perfusion was realized in 1926 by Babkin and Starling, using a dog model. Several normothermic machine perfusions were presented in the studies included. All normothermic machine perfusions had perfusion pump (pulsatile or centrifugal), oxygenator, blood reservoir, and heat exchanger (e.g. circulating water bath). Dialysis unit was added in three studies, and in three studies, the data were missing. Pegg et al 31 used a single-pass method for their experiments, which included two systems of normothermic perfusion, which allowed to use two different perfusion solutions.
Experimental models
Experimental models were porcine models in two studies,14,25 adult mongrel dogs in four studies,26-29 and rat models in two studies.30,31 Nine studies were conducted with DBD model and one study with DCD model.
Perfusion parameters
Eckhauser et al 26 started dogs’ pancreas perfusion at an SP of 90-110 mmHg and then declined to 30-50 mmHg. O’Malley et al 28 compared different SP in dogs’ pancreases models (61, 66, 76.6, and 95 mmHg). WG was not correlated with SP. Pegg et al 31 used WAG rats’ models, perfused using an SP of 60 mmHg.
Flushing and perfusion solution
Kuan et al 25 used Hartmann’s solution as SCS and autologous whole blood associated with cephazolin, epoprostenol sodium, and heparin for perfusion. O’Malley et al 28 evaluated adjunction of Fluosol, an oxygen-carrying emulsion in perfusion solution used in their dogs’ model. WG was more important in the Fluosol group and no histologic differences have been highlighted between Fluosol- and blood-perfused groups.
Length of perfusion
Studies included reported perfusion durations from 90 minutes to 12 hours.
Discussion
Despite almost a 50-year history of pancreatic perfusion, SCS remains the gold standard conservation. This review included studies of pancreas perfusion, in hypothermic and normothermic settings, in the objective of whole-organ transplantation. We have shown that there are important hurdles to overcome for pancreatic perfusion. Of utmost importance is the use of a low perfusion pressure during a short perfusion period (<12 hours). As pancreas is a low vascularized organ and very sensitive of barotraumatism lesions, the use of low perfusion pressure is essential to avoid training of edema.
The contribution of the perfusion would be to assess the organ prior to transplantation with regard to steatosis and the likelihood of post-transplant pancreatitis and to estimate β-cell viability and function of the organ.
Thus, these experimental studies provide elements of answers about adequate viability markers of the pancreas. Weight gain was evaluated to evaluate the edema grafts.
Histologic examination using a conventional staining method (hematoxylin eosin saffron) was performed to assess the degree of ischemic necrosis or congestion of exocrine and endocrine tissues and duodenum. Immunohistochemical analysis was performed to assess the islets viability, with insulin, glucagon, somatostatin, and ATP.
In kidney transplantation, some authors32-34 considered high renal resistance during perfusion as an independent risk factor for the development of delayed graft function. PRI was monitored14,15,17,19-20,22-24,28,31 and decreased during the perfusion. This reflects initial and evolving status of pancreatic microcirculation and PRI should be used as a marker of pancreas transplant viability. Moreover, the pancreatic microvascularization preservation during the storage could help to reduce the risk of pancreas thrombosis. Biochemical analysis of the perfusion solution was performed to assess markers of pancreatic suffering, including lipase, amylase, lactate dehydrogenase, lactates, insulin, glucagon, glucose, and C-peptide.
We reported results of three human experimental hypothermic pancreas perfusion studies. These are feasibility studies of pancreas perfusion, in hypothermic and normothermic settings. Thus, none of these pancreases has been transplanted to assess the reperfusion lesions. Moreover, these pancreases were all rejected for vascularized organ or islet transplantation because of their poor quality. Then, the results presented in this paper did not reflect the possible consequences of the perfusion of an optimal pancreas. Hamaoui et al 14 used porcine and human pancreases with long period of SCS, probably due to logistical problems. However, they reported no pancreatic damages after SCS and higher pancreatic damages after NP than HPP. Thus, in this study, NP would seem to induce more pancreatic lesions.
Concerning experimental hypothermic animals pancreas perfusion studies, the results seem to indicate that a low SP (<25 mmHg) should be used. Therefore, perfusion period longer than 24 hours provoked ischemic necrosis and cell damages of these pancreases.
We reported results of two human experimental normothermic perfusion studies. These two studies have been realized with human pancreases rejected for vascularized organ or islet transplantation. As in hypothermic settings, the results presented in this paper did not reflect the possible consequences of the normothermic perfusion of an optimal pancreas. However, there is a variability in the results presented by Barlow et al 23 and Nassar et al. 24 Indeed, Barlow et al presented important histologic pancreatic damages after six hours of NP, while Nassar et al reported healthy acini and islets after 6 and 12 hours. Thus, histologic lesions reported by Nassar et al could be due to longer SCS period (13 hours versus 4-6 hours).
Human and animal experimental studies suggest that perfusion of pancreatic allografts results in improved β-cell function. These results are interesting because the rate of pancreas discarded was still 32.8% in 2016 in France, 35 due to increasing age of donors, and graft thrombosis occurred in approximately 15%-20% of recipients. The CIT, one of the factors thought to increase graft pancreatitis, is still not able to be extended. Thus, the only option able to reduce CIT and, therefore, pancreatitis and vascular thrombosis, is NP of the pancreas. However, NP of the pancreas is still an experimental application and needs improvement for clinical application.
Potential benefits of machine perfusion include improvement in circulation of oxygen and nutrients, elimination of metabolic waste and toxins, maintenance of vasculature and endothelial protection, opportunity for viability assessment and therapeutic manipulation or gene therapy, and allow long-distance organ sharing. 36 Moreover, use of HP machine with pulsatile flow also enabled maintenance of vasculature and endothelial protection. Indeed, pulsatile flow allowed to maintain shear stress, known as an important factor in regulating endothelial cells’ inflammatory responses. 37 Moreover, this particular pulsatile action may activate endothelial protective genes such as Kruppel-like factor 2. 38 This gene, overexpressed by the endothelium during pulsatile perfusion, is thought to inhibit proinflammatory responses and protect endothelial cells.39,40 The protective role of hypothermic machine perfusion for pancreas transplant may be evaluated by exploration of major ischemic reperfusion injury pathways such as hypoxia-inducible factor 1-alpha, inflammation, and endothelial nitric oxide synthase activation.
In our mind, due to decrease of standard donor (>18 or <50 years old, body mass index <30 kg/m2, no medical history of alcoholism, diabetes, and cardiac arrest), the target of pancreas perfusion should be ECD.
A major limitation of most of these studies is the absence of in vivo evaluation of the pancreas. Further experimentation in animal models is needed to confirm the protective effect of pancreas perfusion, to select precise perfusion parameters useful for pancreas evaluation, and to explain the mechanisms of tissue protection. We could then consider the use of pancreas perfusion for human pancreas to broaden the organ pool and improve outcomes.
For the future, it should be important to evaluate ischemia-reperfusion injuries by model of transplantation and to invest in NP technology as has been done in liver and kidney transplantation. Indeed, with future development of portable NP machine devices, CIT can be minimized as the organ does not need to travel. Moreover, advantage of NP machine is the possibility to treat the organ (accommodation) prior to transplantation, instead of treating the recipient.
Conclusion
This review evaluated the feasibility of ex vivo machine perfusion of experimental pancreas for whole-organ transplantation. Pancreas perfusion is feasible and could be a helpful tool to evaluate pancreas transplant prior to transplantation. Pancreas perfusion (in hypothermic or normothermic settings) could reduce ischemic reperfusion injuries, and maybe could avoid pancreas thrombosis and reduce the morbidity of pancreas transplantation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.