
Abstract
Background and Aim:
Costs for the treatment of diabetes and its comorbidities are a major international issue. A recent randomized clinical trial showed that the introduction of color range indicator (CRI)-based glucose meters (GMs) positively affects the HbA1c of patients with type 1 and type 2 diabetes, when compared to GMs without a CRI. This budget impact analysis aimed to translate this beneficial effect of CRI-based GMs, OneTouch Verio Flex and OneTouch Verio, into potential monetary impact for the healthcare systems of five European countries, Germany, Spain, Italy, France, and the United Kingdom.
Material and Methods:
Data from a randomized controlled trial, evaluating the effect of CRI-based GMs, were used to estimate the ten-year risk of patients for fatal myocardial infarction (MI) as calculated by the UK Prospective Diabetes Study (UKPDS) risk engine. On the basis of assessed risks for MI, the potential monetary impact for the healthcare systems in five European countries was modeled.
Results:
Based on a mean HbA1c reduction of 0.36%, as demonstrated in a randomized controlled trial, the UKPDS risk engine estimated a reduction of 2.4% of the ten-year risk of patients for fatal MI. When applied to our economic model, substantial potential cost savings for the healthcare systems of five European countries were calculated: €547 472 (France), €9.0 million (Germany), €6.0 million (Italy), €841 799 (Spain), and €421 069 (United Kingdom) per year.
Conclusion:
Improving metabolic control in patients with diabetes by the utilization of CRI-based GMs may have substantial positive effects on the expenditure of the healthcare systems of several European countries.
Keywords
Introduction
The International Diabetes Federation (IDF) calls for higher awareness of the global epidemic of diabetes. According to IDF, an increase by 48% from 425 to 629 million in diabetes prevalence is expected worldwide by 2045. 1 In Europe, 58 million individuals (age 20-79) lived with diabetes in 2017. 1 Diabetes is a chronic condition and a proven risk factor for long-term complications. Subsequently, it accounts for a twofold excess risk of stroke, coronary heart disease (CHD), or deaths due to other vascular diseases, being responsible for 325 000 deaths per year in high-income countries alone.2,3
A pressing issue on international agendas is the treatment cost of patients with diabetes. Globally, the costs caused by diabetes reached $727 billion in 2017, $166 billion in Europe alone. 1 A current economic analysis estimates that the individuals with diabetes have a 2.3 times higher average of medical expenditures than a person without diabetes. 4 Therefore, lowering diabetes expenditures is of global relevance. 5 A possible solution to lower healthcare costs is the reduction of long-term complications based on improved self-monitoring of blood glucose (SMBG),6,7 a main pillar of diabetes management. 8 If performed regularly, it can improve HbA1c and slow down and reduce the number of hospitalizations due to long-term complications. 9 Utilization of color range indicator (CRI)-based blood glucose meters (GMs) is an applicable solution to improve glycemic control and HbA1c as well as patient and physician satisfaction.10-12 Evidence indicates that the use of a CRI-based GM improves the health literacy by engaging the patients in SMBG, and therefore, acting in a timely manner on blood glucose level. 13
A recent randomized control trial (RCT)—ACCENTS—compared CRI-based GMs (OneTouch Verio Flex (Flex) and OneTouch Verio (Verio), LifeScan, Wayne, PA, United States) with GMs without CRI to analyze the impact of CRI on glycemic control in patients with type 1 and type 2 diabetes mellitus (T1DM and T2DM). The RCT demonstrated a statistically significant and clinically meaningful reduction (0.36%) in HbA1c when using Flex and Verio meters in patients with T1DM and T2DM. Looking at results from Flex and Verio GM groups separately, a decrease of HbA1c by 0.21% and 0.42% could be observed, respectively. Utilization of Flex or Verio GMs empowered the patients and fostered their independence in interpreting the results and taking informed choices. 11 This recent RCT confirmed previous studies that showed a reduction of HbA1c when using CRI-based GMs in both patients with T1DM and T2DM.14-16
A previous analysis indicated that the use of CRI-based GMs may result in annual savings of €40 to €70 million for the German healthcare system. 17 A European analysis (France, Germany, Italy, Spain, and the United Kingdom) could show that the utilization of CRI-based GMs with or without a telemedical application may reduce healthcare costs from €10.5 million (United Kingdom) up to €63.3 million (Germany). 18 However, a direct comparison between GMs with and without CRI with regard to monetary savings has not been performed yet.
This budget impact analysis aimed at evaluating the financial impact of using a CRI-based GM compared to a GM without CRI for SMBG. The estimated cost impact was calculated for five European countries: France, Germany, Italy, Spain, and the United Kingdom.
Methods
Economic modeling was done in accordance with previously published work17-20 using the UK Prospective Diabetes Study (UKPDS) risk engine. The UKPDS risk engine is a well-established risk calculator specific for comorbidities of T2DM, facilitating the prediction of the risk of nonfatal and fatal CHD, as well as nonfatal and fatal stroke. Risk calculations are based on parameters such as age, sex, ethnicity, HbA1c level, systolic blood pressure, and cholesterol levels. In total, the risk engine is built on approximately 53 000 patients’ years of data from the UKPDS (https://www.dtu.ox.ac.uk/riskengine/).
Data from the abovementioned study on the advantages of CRI-based GMs for SMBG 11 were incorporated into risk assessment with the UKPDS risk engine to estimate the ten-year risk for nonfatal and fatal myocardial infarction (MI) and nonfatal and fatal stroke. Additional values for blood pressure and lipids were taken from a previously published observational study on SMBG with CRI technology. 12 Based on the ten-year risk assessment, potential monetary savings were calculated for five European countries—France, Germany, Italy, Spain, and the United Kingdom. The estimated monetary savings are reductions of direct costs arising from a reduction of expenditure due to a decrease of diabetes-related medical costs, attributable to improved diabetes management. These costs involve direct costs for acute MI, direct costs for follow-up (first year), and direct costs for successfully treated MI. Latest available data for these diabetes-related costs were retrieved from the following references: France,21-24 Germany,25,26 Italy,27-29 Spain,30-36 and the United Kingdom37-43 (summarized in Table 1).
Summary of Parameters Incorporated into the Analysis.
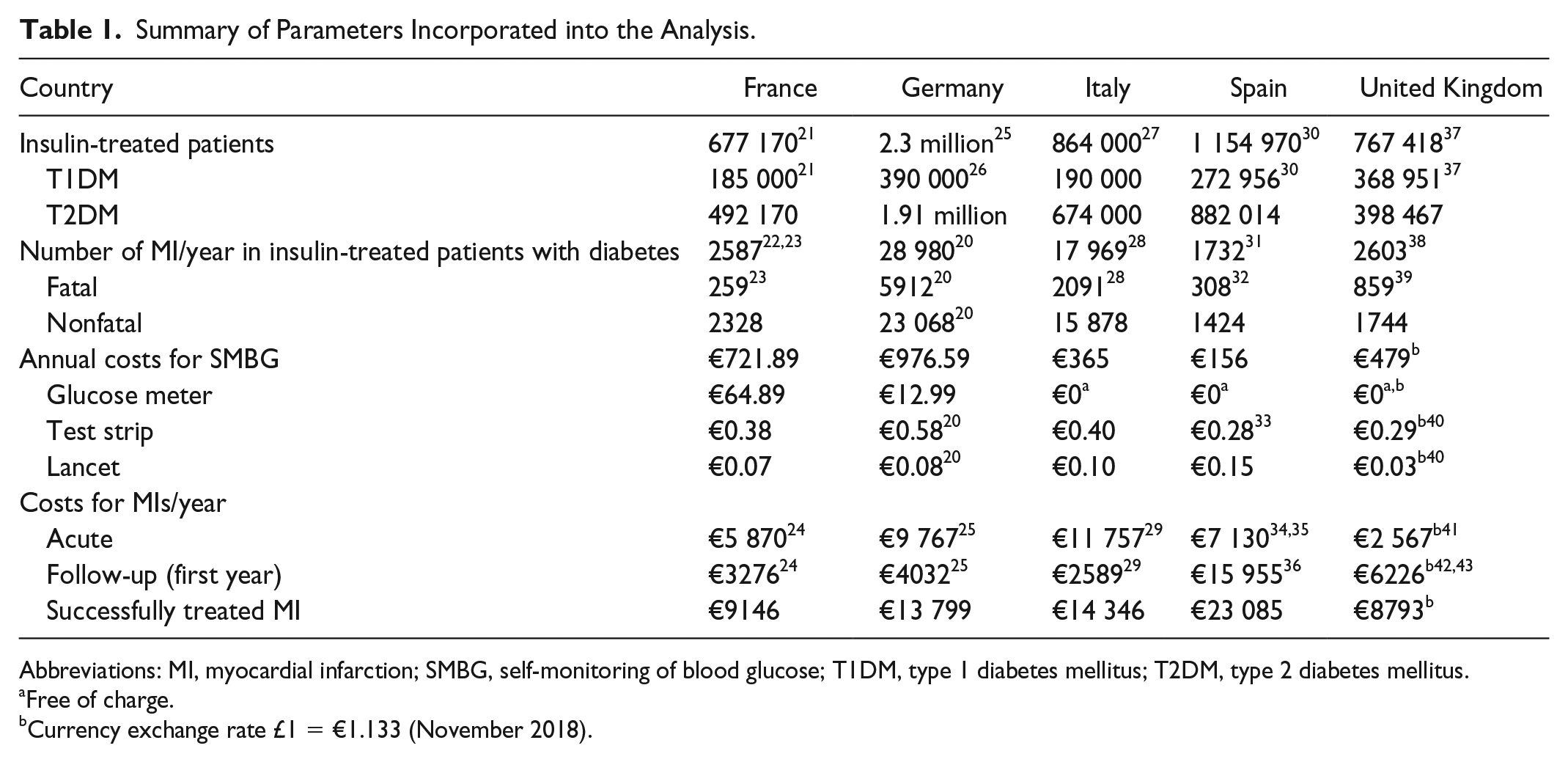
Abbreviations: MI, myocardial infarction; SMBG, self-monitoring of blood glucose; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Free of charge.
Currency exchange rate £1 = €1.133 (November 2018).
Average annual costs were modeled for each country for all insulin-treated patients with diabetes (including patients with T1DM and T2DM) as well as per patient per year. This analysis focuses on reductions of medical costs for the healthcare systems due to a decrease of diabetes-related risk for fatal and nonfatal MIs upon the usage of SMBG with a CRI. The decrease of risk for stroke and possible cost reductions for nonfatal and fatal stroke were not considered here.
All costs were calculated in the European Union currency Euro (€) for the control (usual care) and intervention groups of the study. 11 National currency of the United Kingdom was converted into € using nominal exchange rates from the HM Revenue & Customs Department of the UK Government from November 2018 (£1 = €1.133).
Analysis was performed for four groups of the RCT: (1) Control (usual care), (2) Flex + Verio, (3) Flex, and (4) Verio. Flex or Verio groups represent patient groups using either device with associated medical improvements. The Verio GM has additional features (eg, pattern detection tools, and motivational and achievement messages) distinguishing it from the Flex GM. 11 The Flex + Verio group represents aggregated values for a combined outcome for the use of SMBG with a CRI in the previously defined patient group.
Cost Estimates
Self-Monitoring of Blood Glucose
Based on recent prices for test strips and lancets multiplied by average measurements per day, multiplied by 365 days, and added to the price for GM, the average annual cost of SMBG was calculated. Reimbursement of GM varies between countries (Table 1).

Myocardial Infarction
National and international publications provided the current values of expenditures for both fatal and nonfatal MI events.20,22,23,28,31,32,38,39,42,43 According to fatal MI events in the diabetic population, fatal MI events were estimated for insulin-treated patients. Costs for fatal and nonfatal MI events were calculated as acute treatment costs and successfully treated (acute treatment costs summed with the first-year follow-up costs). For both fatal and nonfatal MIs, the average costs were calculated as the number of cases per year multiplied by average costs for specific treatment:

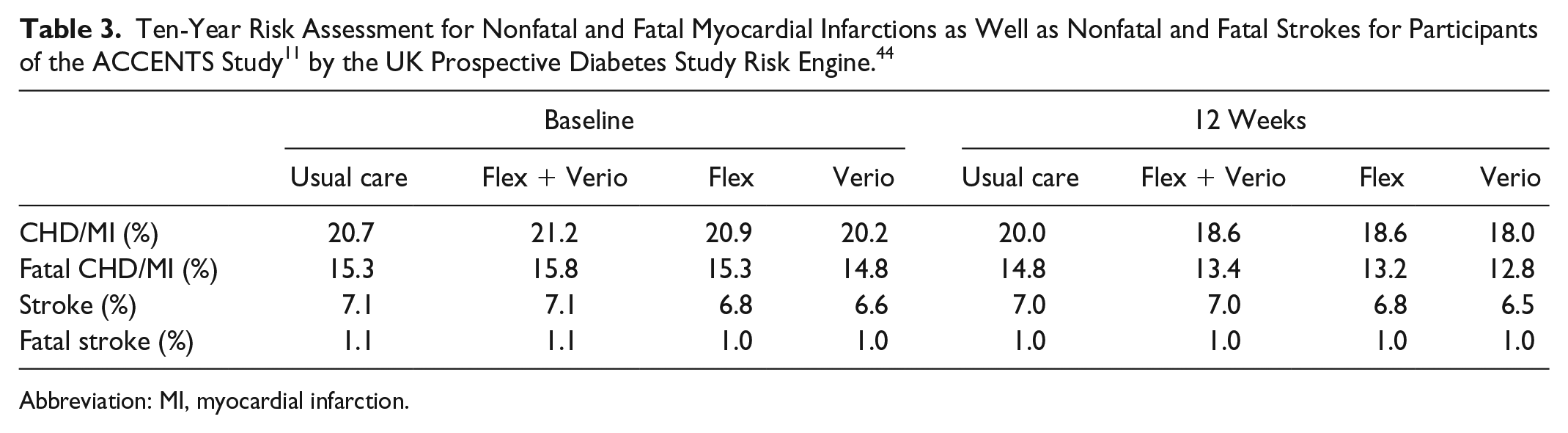
UK Prospective Diabetes Study Risk Engine 44
Reduction of HbA1c level after 12 weeks in the usual care group (0%), and intervention groups (0.24% [Flex], 0.45% [Verio], and 0.36% [Flex + Verio]) compared to baseline 11 and the data of Schnell et al 12 (systolic blood pressure, total cholesterol, and high density lipoprotein cholesterol) (Table 2) were applied to the UKPDS risk engine to predict ten-year risk reduction for fatal and nonfatal MI and fatal and nonfatal stroke.
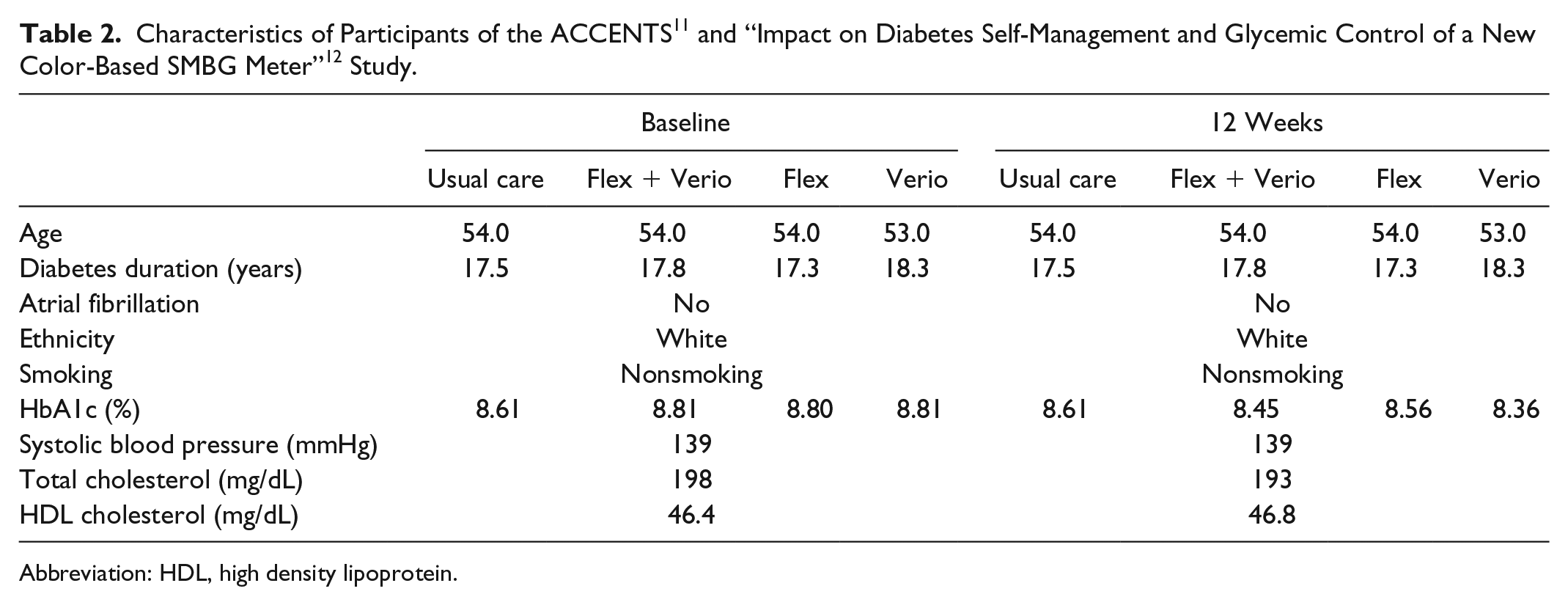
Abbreviation: HDL, high density lipoprotein.
Cost Calculations
Myocardial Infarction
Based on the reduction of the ten-year risk of fatal MI and the treatment cost of MI in insulin-treated patients with diabetes, the annual savings were calculated for all insulin-treated patients per year and per patient per year:


Results
Ten-Year Risk Assessment of Fatal MI
Risk assessment with the UKPDS risk engine suggested a 0.5% ten-year risk reduction of fatal MI in the usual care group which had no HbA1c reduction but rather a minor improvement in lipid profile. A HbA1c reduction of 0.36% in the Flex + Verio group resulted in a ten-year risk reduction of fatal MI of 2.4%, while a 2.1% (0.24% HbA1c reduction) and a 2.0% (0.45% HbA1c reduction) ten-year risk reduction of fatal MI were observed for the Flex and the Verio group, respectively (Tables 2 and 3).
Abbreviation: MI, myocardial infarction.
Economic Analysis for the Flex and Verio Group Vs the Usual Care Group
According to the UKPDS risk engine, improving glycemic control should positively influence the risk of diabetes-related cardiovascular events. To evaluate different GMs—Flex and Verio—separately, an additional cost analysis was performed. Looking at costs for fatal and nonfatal MI in insulin-treated patients in five different European countries, financial impact considering all insulin-treated patients was calculated. In each country, cost reductions for the usual care group, the Flex group, and the Verio group were calculated, according to corresponding reductions in HbA1c and derived estimated MI risk.
This analysis suggests cost reductions of €114 056 (usual care group) compared to €479 038 in the Flex group and €456 226 in the Verio group in France; €1.9 million (usual care group), €7.9 million (Flex group), and €7.5 million (Verio group) in Germany; €1.3 million (usual care group), €5.3 million (Flex group), and €5.0 million (Verio group) in Italy; €175 374 (usual care group), €736 574 (Flex group), and €701 499 (Verio group) in Spain; and €87 723 (usual care group), €368 435 (Flex group), and €350 891 (Verio) in the United Kingdom (Figure 1; Table 4).
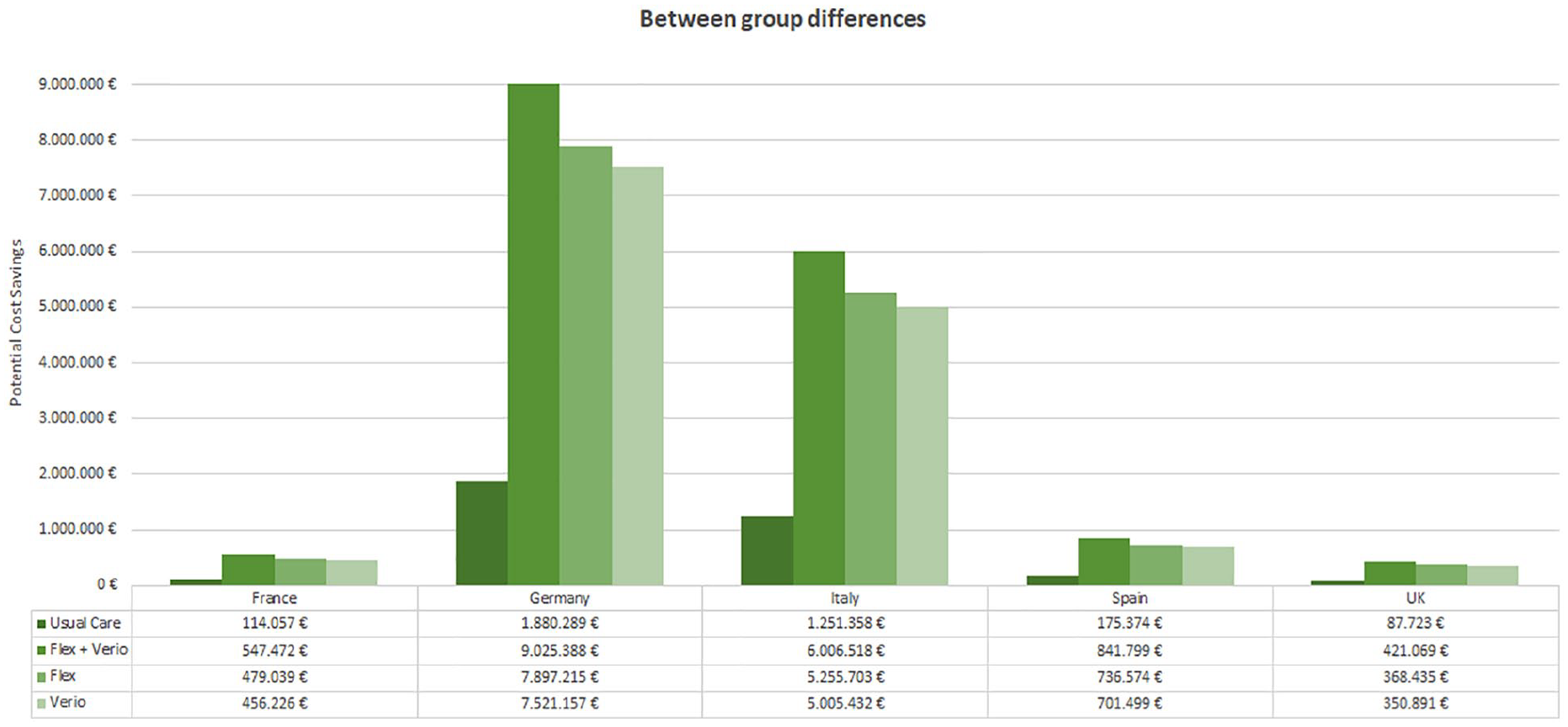
Potential cost savings for five European healthcare systems and for all insulin-treated patients resulting from a 0.5%, 2.4%, 2.0%, and 2.1% risk reduction in fatal myocardial infarction in the next ten years.
Cost Savings Per Patient and for All Insulin-Treated Patients Resulting From a 0.5%, 2.4%, 2.0%, and 2.1% Risk Reduction in Fatal Myocardial Infarction in the Next Ten Years.
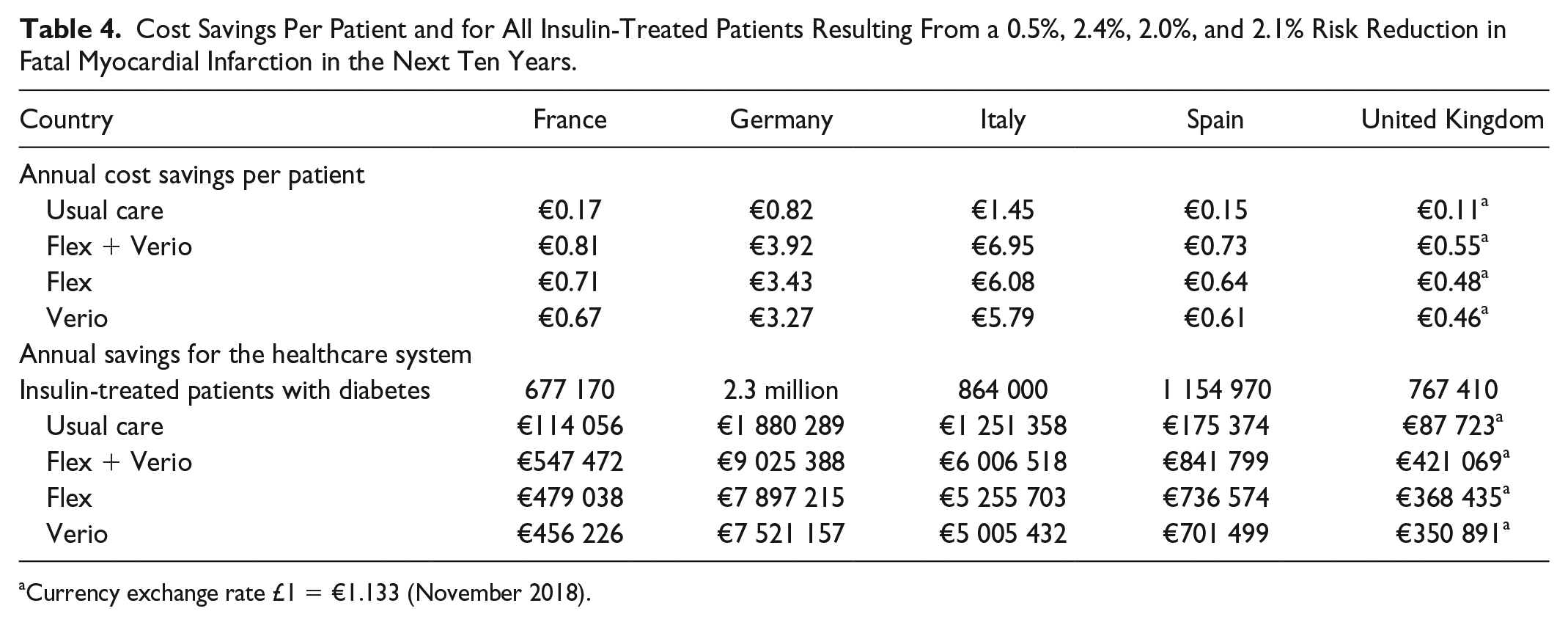
Currency exchange rate £1 = €1.133 (November 2018).
Economic Analysis for the Combined Flex + Verio Group Vs the Usual Care Group
An aggregated analysis of both, Flex and Verio (Flex + Verio), resulted in a higher ten-year risk reduction of fatal MI (2.4%). As a consequence, potential monetary savings for the healthcare system of the five European countries increased substantially.
France: Utilization of a CRI-based GM could result in cost savings per patient per year in France from €0.17 to €0.81. Translating this to all insulin-treated patients with diabetes in France, cost savings were calculated to be €547 472 (Figure 1; Table 4).
Germany: When analyzing cost impact due to the reduction of fatal MI for Germany, the cost savings could be €3.92 per patient per year. Calculated for all insulin-treated patients with diabetes in Germany, cost savings sum up to €9.0 million if patients use a CRI-based GM (Figure 1; Table 4).
Italy: Italy has 864 000 insulin-treated patients with diabetes. Potential cost savings for the Italian healthcare system due to the utilization of a CRI-based GM were determined to be €6.0 million, when focusing on estimated reductions of fatal MI. Per patient per year, €6.95 could potentially be saved (Figure 1; Table 4).
Spain: In Spain, cost savings per patient per year as a result of decreasing risk of MI in the next ten years were estimated to be €0.73. Scaled for all insulin-treated patients with diabetes in Spain, cost savings were calculated to be €841 799 (Figure 1; Table 4).
United Kingdom: Similar to Spain, cost savings per patient per year were €0.55 for a reduction in fatal MI. Looking at all insulin-treated patients with diabetes in the United Kingdom, cost savings were calculated to be €421 069 (Figure 1; Table 4).
Discussion
This budget impact analysis evaluated potential financial savings for the healthcare systems of five European countries, France, Germany, Italy, Spain, and the United Kingdom, for the utilization of CRI-based GMs (Flex and Verio) compared with GMs without CRI in patients with T1DM and T2DM. 11 Risk estimation and cost calculations were done as previously published17,18,19,20 and described. Clinical and economic impact of this study go hand in hand. Using the clinical data from the RCT ACCENTS, the reduction of HbA1c facilitated by the use of SMBG with CRI, compared to SMBG without CRI, ten-year risk for MI was calculated using the UKPDS risk engine. Potential monetary benefits for individual patients were not looked at. The RCT ACCENTS reported a decrease in HbA1c by 0.24% in the Flex group, a HbA1c reduction of 0.45% in the Verio group, and a decline in HbA1c of 0.36% in the Flex + Verio group. 11 These results translated into a 2.1%, 2.0%, and 2.4% risk reduction of fatal MI in the next ten years, respectively, as calculated by the UKPDS risk engine. Thus, UKPDS risk engine assessments suggested that improving glycemic control by the utilization of a CRI-based GM could positively influence the risk of diabetes-related cardiovascular events as reduction of fatal and nonfatal MI risk in patients with T1DM and T2DM. The economic impact of this study is represented in the estimated cost savings for the analyzed healthcare systems. Per patient, potential cost savings in the Flex + Verio group in France, Germany, Italy, Spain, and the United Kingdom were calculated to be €0.81, €3.92, €6.95, €0.73, and €0.55, respectively. Associated annual savings were estimated to be €547 472 in France, €9.0 million in Germany, €6.0 million in Italy, €841 799 in Spain, and €421 069 in the United Kingdom in the intervention group vs less pronounced savings in the usual care group, €114 056, €1.9 million, €1.3 million, €175 374, and €87 723, respectively. This clearly indicates that every healthcare system would have a monetary benefit if insulin-treated patients with T2DM apply SMBG with CRI, as compared to SMBG without CRI.
Inclusion criteria of the ACCENTS study were an age of 18 to 79 years, diagnosed with T1DM or T2DM for ≥3 months, a current HbA1c of 7.5% to 11%, and performance of SMBG. Mean HbA1c in ACCENTS was 8.6% in the control group and 8.8% in the intervention group, with approximately 56% and 44% females, respectively, and a mean age of 54 years. 11 While it may be argued that a HbA1c > 8% may not be representative of the average T2DM population, one needs to consider that particularly in populations initiating or receiving insulin treatment, blood glucose often is out of range and elevated, not seldom with HbA1c levels above the here mentioned. High HbA1c levels have been clearly associated with worsening clinical prognosis of diabetes mellitus 26 and an increasing HbA1c has been associated with an increasing risk for MI. 45 Thus, it may be claimed that the estimated MI risk derived from HbA1c levels in the ACCENTs study 11 and the additional clinical data used 12 in this study does represent a population average. A recent study estimated risk for MI using the UKPDS risk engine with clinical characteristics from 5717 patients from the TECOS-trial population, yet analyzing predefined 1%-HbA1c-steps with a HbA1c range of 6% to 10%. With every 1%-HbA1c step, in comparison to the reference HbA1c of 10%, a relative risk reduction of approximately 4.5% was observed. This translated to a mean absolute risk for MI of 22.3% with a HbA1c of 10%, while a HbA1c of 6% still translated into an absolute risk of 19.4% for MI. 46 These values are comparable to those computed in this analysis, supporting risk estimations made here.
In contrast to a previous study, 18 this analysis only calculated cost savings provoked by a reduction of MI, not taking into account cost savings for a reduction of hypoglycemic events. A key aspect responsible for the variability in cost savings in the individual countries might be the respective diabetes prevalence. While diabetes prevalence in the United Kingdom (5.9%), France (7.3%), and Italy (7.6%) is below European average (regional prevalence 8.8%), prevalence rises above average in Spain (10.4%) and particularly Germany (12.2%). 47 Also, the differences in the “cost per person with diabetes,” ranging from €2744 in Spain to € 5539 in France 1 (€1 = $1.1743, November 2018, www.federalreserve.gov), could potentially have an impact on economic outcomes. In this study, differences in treatment costs are reflected in the heterogeneity in treatment cost of MI in five different healthcare systems.
This economic analysis offers a unique perspective on the utilization of CRI-based GMs. The key obstacles for successful SMBG are knowledge barriers (interpretation of values obtained), human factor barriers (inadequate technical handling), logbook barriers (incomplete data recording), and economic barriers (financial affordability of SMBG).48,49
Knowledge barriers are considered as lack of knowledge of SMBG users on how to properly interpret the numbers obtained and lack of concomitant therapy and/or lifestyle adjustments. 48 A survey conducted with patients with T2DM revealed that about 56% did not regularly respond to out-of-range glucose values. 50 When looking at utilization of the obtained SMBG results specifically in insulin-treated patients, the study revealed that only 36% regularly adjusted their meals accordingly, with even lower percentages when focusing on physical activity (15%) or medication (22%). 50 This knowledge gap could either be filled by intensified care by physicians 48 or using intuitive technologies like CRI-based GM. The ACCENTS study demonstrated that a CRI-based GM significantly reduces knowledge barriers 11 which in turn can lead to a better understanding of diabetes management. 49
Overcoming human factor barriers can be mediated by providing patients with different choices of GMs, best fitting their needs. Limiting factors for conventional GMs may include, for example, that many patients with diabetes are elderly with bad eyesight 51 or have other limiting disabilities such as bad numeracy. 52 It has been shown that low health literacy is not only associated with inadequate glycemic control and a higher frequency of self-reported hypoglycemia53,54 but also with deprivation and other adverse social factors such as smoking which in turn are associated with poor health outcomes. 55 In both cases—bad eyesight and low health literacy—a CRI-based GM may provide adequate assistance to allow the patients to make necessary adjustments. So far, two studies by Grady et al could show the impact of CRI-based GMs in participants with lower health literacy: they would preferentially take action on SMBG results shown with color compared to results without color, 52 and a comparable HbA1c reduction was observed in participants with different health literacy. 11 These results indicate a beneficial effect of CRI-based GM, specifically in patients with diabetes with bad numeracy.
Economic barriers encompass difficulties to access SMBG accessories like an appropriate amount of test stripes due to financial limitations. 48 This critical aspect is not addressed by the introduction of CRI-based GMs and should be discussed on a more country-specific level. Similarly, logbook barriers cannot be resolved by the utilization of CRI-based GMs. Those could rather be improved by digital innovation for standardized recording of blood glucose values and possibly also implicated in telemedical programs.
In summary, a variety of studies has analyzed the effects of CRI-based GMs10-12,16,48 and found a consensus when it comes to the improvement of clinical parameters11,12,16,48 as well as patient and physician satisfaction.10-12 In combination with budget impact studies,17,18 there are clear indications that the utilization of CRI-based GMs may be beneficial, not only for the patients’ health but also for the health economics of the individual countries. This new economic analysis shows that substantial monetary savings can be made by switching patients from GMs without CRI to CRI-based GMs. As all participants of the study had the previous experience with SMBG, the impact of CRI is particularly emphasized. 11
Limitations
This study is based on existing studies and reports. Limitations include a relatively small sample size in the RCT by Grady et al 11 and the retrieval of blood pressure and lipid level values from a different study population, investigating the use of a GM with CRI. 12 It should be taken into account that the UKPDS risk engine was designed on a population of newly diagnosed male and female T2DM patients, while our analysis included both people with T2DM and T1DM. This study focuses on direct cost savings derived from a reduction of macrovascular complications, neglecting the impact of microvascular complications on people with diabetes which could be reduced by an improved metabolic control. Also, this analysis does not include social perspectives and is limited to financial savings from a healthcare system perspective. Differences between countries regarding the number of MI/year in insulin-treated patients, as well as differences in costs for MI/year, which contribute to the overall differences observed in budget impact in each country in this study are a limitation. Both number and cost of MI/year are based on the best currently available evidence from each country.
Conclusion
The improvement of metabolic control, ie, a mean HbA1c reduction by 0.36% when using CRI-based GMs (Flex and Verio) instead of GMs without CRI, resulted in monetary savings for the health systems of five European countries—France, Germany, Italy, Spain, and the United Kingdom—in our economic model. The results stress the financial relevance of improved glycemic control in diabetes mellitus patients, which can be facilitated by the improvement of patient knowledge and self-management by, for example, CRI-based GMs. In combination with a previously performed economic analysis of telemedical approaches, 18 this study adds insights on strategies of how to apply resources for diabetes management in an economically efficient way.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KF, KB, CS, and KFB have no conflict of interest. MRA, AN, BK and BV are members of the LifeScan Advisory Board. YH is a full-time employee of LifeScan GmbH. OS has acted as member of advisory boards and given lectures for companies which are involved in glucose monitoring; and is CEO and founder of Sciarc GmbH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by LifeScan Inc.