
Abstract

Keywords
Hypoglycemia is associated with increased physical and psychosocial morbidity and is a risk factor for mortality.1,2 Hypoglycemia is very common in patients with type 1 diabetes mellitus. Patients trying to obtain or maintain a tight glycemic control suffer from frequent episodes of asymptomatic hypoglycemia. Some studies suggest that plasma glucose levels may be less than 60 mg/dL (3.3 mmol/L) 10% of the time. Moreover, on average, patients with type 1 diabetes suffer from two weekly incidents of symptomatic hypoglycemia.1,3,4 We have in two previous studies5,6 investigated the potential of using continuous glucose monitor (CGM) and additional heart rate variability (HRV) data to predict hypoglycemia. Data from ten patients with type 1 diabetes studied during insulin-induced hypoglycemia were obtained and tested. 5 Furthermore, in 21 patients with type 1 diabetes prone to hypoglycemia monitored with CGM and a Holter device while they performed normal daily activities, we found that using information from both HRV and CGM yielded more accurate predictions than using information from CGM only. 6 However, questions still remained if these results could be generalized to a large cohort of patients. Therefore, we sought to validate the algorithm developed in the previous studies on a new larger and more diverse population of patients with type 1 diabetes.
We investigated data from 56 patients with type 1 diabetes who had been monitored with CGM and Holter device for up to seven days. The characteristics of the patients were 40 men, mean (SD) age 68.7 (6.3) years, diabetes duration 34.5 (15.6) years, 40 men/16 women, BMI 25.9 (3.3) kg/m2, systolic blood pressure 143 (20) mmHg, diastolic blood pressure 77 (11) mmHg, and 27 patients (48%) had signs of peripheral neuropathy. Hypoglycemia was defined as CGM levels below or equal to 3.9 mmol/L and we set up the algorithm to predict if CGM reading of 4.4 mmol/L or below would result in hypoglycemia within a 20-minute timeframe. The algorithm as described previously5,6 is based on patterns from the historical HRV and CGM data. For instance, when predicting from one point in time (t0) up to 20 minutes ahead (t+20), the algorithm would use data prior to t0 such that one-hour window was used (data t-20 . . . data t0) to extract patterns from HRV and CGM. We compared three models for hypoglycemia prediction: simple CGM, algorithm CGM, and algorithm CGM + HRV implemented according to the previous study. 6
Table 1 shows the results for the prediction. During night, 94 CGM readings of 4.4 mmol/L or below were identified, resulting in 23 episodes of hypoglycemia. The algorithm CGM + HRV performed best, finding 23/23 episodes compared to 20/23 for algorithm CGM and 18/23 for simple CGM. Prediction during the day yielded a smaller improvement using the additional information from HRV.
Results From the Hypoglycemia (Hypo) prediction.
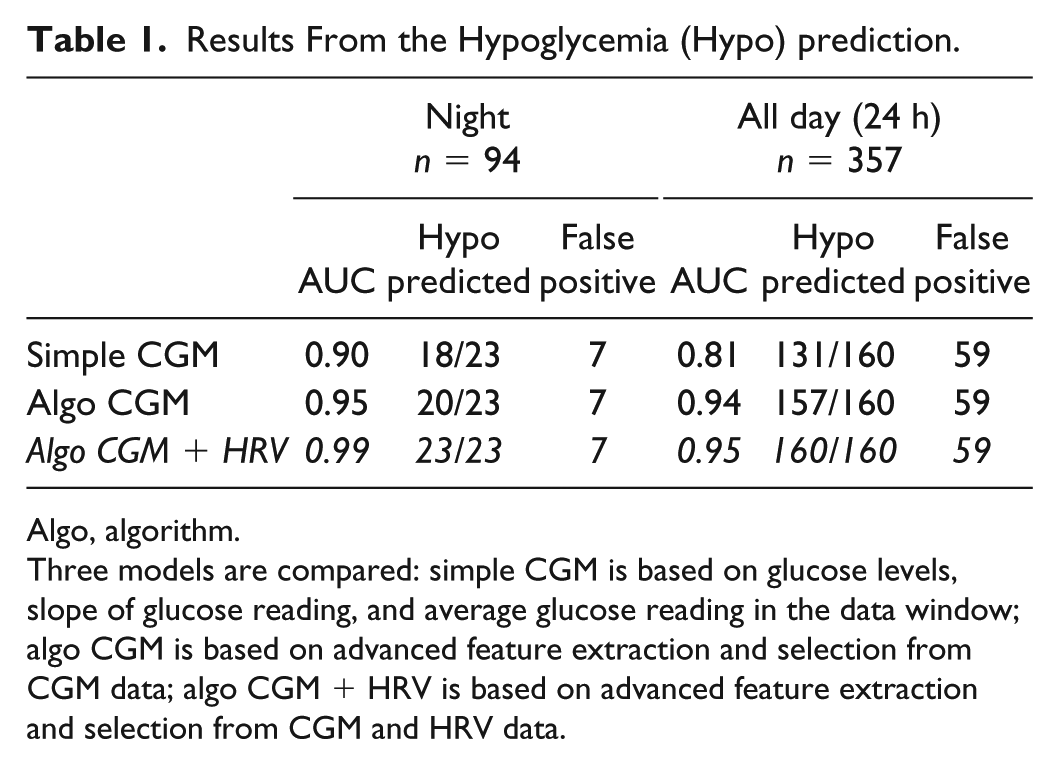
Algo, algorithm.
Three models are compared: simple CGM is based on glucose levels, slope of glucose reading, and average glucose reading in the data window; algo CGM is based on advanced feature extraction and selection from CGM data; algo CGM + HRV is based on advanced feature extraction and selection from CGM and HRV data.
Our results validate that the combined use of CGM and HRV data could potentially improve the prediction accuracy of identifying upcoming episodes of hypoglycemia in patients with type 1 diabetes.
Footnotes
Author Contribution
S.L.C and J.F generated the study hypothesis; developed the study design; acquired, analyzed, and interpreted data; and drafted and revised the manuscript. M.M.H collected data and contributed to the discussion and critically revised the manuscript. B.T, U.P.B. and L.T contributed to the discussion and critically revised the manuscript. S.L.C. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The algorithm tested in this article was developed by Medicus Engineering. S.L.C. and J.F. are consultants for Medicus Engineering.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This investigation was funded by the Innovation Fund Denmark.