
Abstract

Response to Letter to Editor:
We thank the author of this letter for raising his concerns regarding the section about electronic glucose management systems (eGMS). In our review article, we aimed to provide a general update on available technologies for the management of hyperglycemia and diabetes in the critically ill population. No comparison of outcomes or endorsement of any specific technology was intended, as supported by our introductory statement of the eGMS section: “To date, there have been no head-to-head studies comparing differences among these eGMS. However, there have been studies assessing the safety and efficacy suggesting that these eGMS likely provide better glycemic control compared to paper-based algorithms.” 1
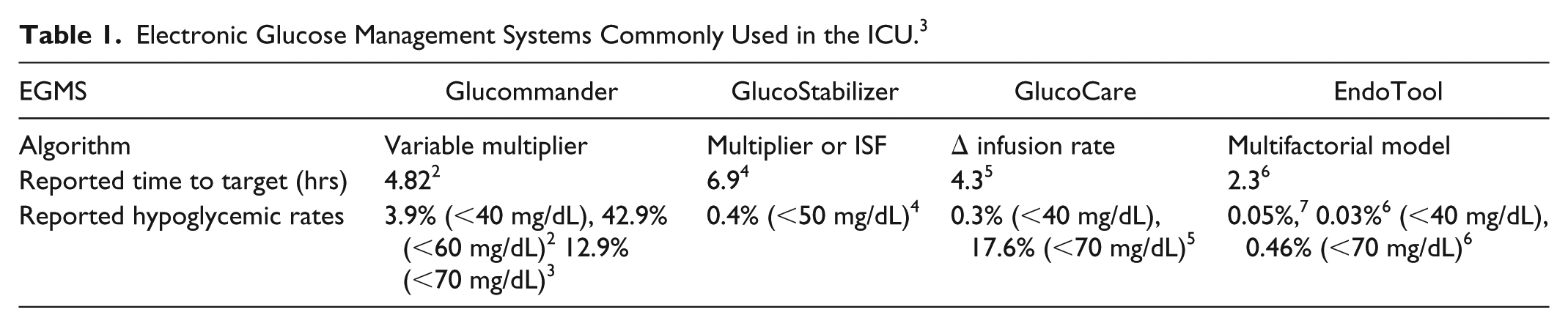
Within this general review, in the section of eGMS, we agree with the author that there is a lack of consensus on reporting rates of hypoglycemia for hospitalized patients and that different studies have used different measures, including percentage of hypoglycemic values, percentage of patients with hypoglycemia, and percentage of patient-days with hypoglycemia. For this review, we documented rates of hypoglycemia exactly as reported by authors in the cited studies with the appropriate reference made to each study as can be found both in the text of the section, as well as in Table 1. However, absolutely no manipulation of the data was done, and more importantly, no values or measures were favored or chosen to be reported, as incorrectly claimed by Rhinehart in this letter. Both cited articles for the Glucommander (GM) referenced only one measure of hypoglycemia within their results section, which was the one used in our review.2,3
Electronic Glucose Management Systems Commonly Used in the ICU. 3
In this general review of glucose technologies, effort was made to choose studies with higher quality of evidence, such as those with prospective randomized design or large sample size when possible. In agreement with the author, a more recent study comparing GM vs paper protocol was not detected in our search and thus was not included. 8 However, it is worth mentioning that both studies used in our review for the GM section, including both the 77-arm ICU prospective randomized controlled study by Newton et al, 2 and the more recent retrospective study published in 2018 of 2665 patients with DKA, 3 were significantly larger than the referenced small retrospective study which only used 27 patients for the GM arm. 8 No results from abstracts or posters were included in this review.
In summary, no randomized controlled studies comparing different eGMS were available, and no attempt was made in this review to favor any technology in particular. We understand the concerns raised by the author of this letter regarding the reporting of different measures for hypoglycemia presented in various studies evaluating diverse technologies, and we agree that consensus on glucometrics should be reached to make comparisons more valid among studies. However, an attempt to compare or make conclusions on outcomes of the different technologies was beyond the scope of this general review, and more importantly, no values were chosen or manipulated to favor or discredit one technology over another.
Footnotes
Abbreviations
DKA, diabetic ketoacidosis; eGMS, electronic glucose management systems; GM, Glucommander; ISF, insulin sensitivity factor.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CEM is part of the medical advisory board for Monarch Medical Technologies. Other author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.