
Abstract
Background:
Many people with type 1 diabetes (T1D) do not achieve levels of exercise recommended by the American Diabetes Association, often due to unique barriers, including fear of hypoglycemia. This study aimed to broaden the understanding of barriers and facilitators to exercise among adults with T1D by exploring social media—specifically T1D-themed blogs—in addition to more traditional interviews and journals.
Methods:
Data sources included exercise-focused T1D blog posts (n = 67) and associated comments (n = 717), as well as interviews of and journals kept by adults with T1D (n = 10). Data were analyzed using a qualitative inductive thematic approach. Shared and unique themes were identified among the three data sources. Content mapping illustrates these relationships and interplay.
Results:
Three metathemes were identified: (1) exercise with T1D requires significant planning, (2) hypoglycemia often interrupts or causes alteration to exercise, and (3) “ordinary” activities can cause greater insulin sensitivity and hypoglycemia, much like planned exercise, but are often unrecognized as exercise. Unique themes found only in the blogs, only in interviews, or only in journals are also reported.
Conclusions:
Social media such as blogs can be a valuable addition to qualitative research, especially when combined with other sources of data. This study suggests a need for providing adults with T1D with more instruction on preventing hypoglycemia during exercise, as well as links to organized or online activities that can provide support and education. Health care providers may wish to consider strategies to help adults with T1D recognize glycemic impact from daily activities not typically recognized as exercise.
Physical activity contributes to overall health and mental wellbeing in all adults, 1 and for adults with type 1 diabetes (T1D) there are crucial incremental benefits compared to individuals without diabetes, such as decreased cardiovascular disease and mortality. 2 The American Diabetes Association (ADA) recommends that adults with diabetes perform at least 150 minutes of moderate-to-vigorous activity and 2-3 sessions of resistance training per week, with no more than two consecutive days without exercise. 3 A recent consensus statement provides recommendations including glucose targets, nutrition, and insulin adjustments in exercise management. 4 Despite these recommendations and guidelines, most adults with T1D—like most adults in general—do not get the recommended amount of exercise.5-7 While there are multiple barriers to exercise in the general population (eg, lack of time and/or motivation, limited access to facilities, inclement weather, and unsafe neighborhoods),8-10 specific additional barriers exist for adults with T1D, such as fear of hypoglycemia.11-16
Qualitative research is “intended to generate knowledge grounded in human experience” 17 and is an important methodology to better understand the barriers and facilitators that adults with T1D experience while attempting to exercise. Previous studies on barriers to exercise for people with T1D have employed traditional qualitative methods such as questionnaires with open-ended responses, focus groups, and interviews.14,15
Social media is a growing platform for conducting research,18-22 including for the study of diabetes. There is a vast and vibrant Diabetes Online Community (DOC)—a term widely used to encompass the people and their various online activities related to living with diabetes. 23 Blogs (online journals usually maintained by one person, whereby people can leave comments to start meaningful conversations) are one part of the DOC that can represent a breadth of people living with T1D and that can help broaden understanding and identify barriers and facilitators to exercise in T1D that may not have been found previously. Blogs allow people to share their thoughts and experiences when and where they choose, unconstrained by time, geographic proximity to other participants, or a research environment. They allow for anonymous participation, if desired, and enable asynchronous interaction between bloggers, commenters, and noncommenting blog readers. This study adds to the growing literature on barriers and facilitators to exercise in adults with T1D by combining blogs with traditional qualitative data sources, thereby seeking to broaden understanding further. Such a complementary array of data sources allows representation from a broader population, through more diverse means of expression, thereby mitigating the limitations of each unique type of data source. To our knowledge, there have been no prior studies analyzing blogs to further explore challenges and successes in exercising with T1D.
Methods
This study was approved by the Penn State College of Medicine Institutional Review Board. Informed consent was obtained from all participants prior to participation. Three different types of data were utilized: blogs, individual interviews, and handwritten journals.
Data Sources, Participants, and Data Collection
Blogs
Blogs were selected through a combination of previous work analyzing the DOC 23 and snowball sampling 24 with a focus on well-known, sustained blogs with high volumes of usage. Snowball sampling began with the most visited and visible T1D blog, Six Until Me (www.sixuntilme.com), which serves as a gateway to other blogs. This yielded a group of four online blogs written by adults with T1D that also had available on them content tags for “exercise” and/or “fitness,” or whose blog owner was willing to add such tags. Based on viewable data from the blogs themselves (eg, pageview counters) and analytics supplied by the bloggers, the included blog sites were viewed approximately 90,000 times per month by 45,000 unique individuals. Blog authors were contacted via email, and each provided permission to retrospectively analyze the posts and comments on their blogs. All included data were publicly available online; all blogs could be found by internet search engine, did not require invitation, permission, or password to access content, and could therefore be viewed and have comments added by anyone with internet access via standard web browsers.
Interviews and Journals
To obtain interview and journal data, ten people with T1D between the ages of 18 and 65 years were recruited from the Penn State Hershey clinical population. A large age range was selected to include barriers and facilitators to exercise across a broad age distribution. To understand exercise barriers especially, those who did not meet current ADA recommendations for exercise 3 were sought.
Data were collected via qualitative interviews conducted by two authors (TKO and GW) based on a topic guide that addressed exercise barriers that participants faced while trying to exercise, factors that made it easier to exercise, and the sources from which participants obtained information on exercising with diabetes. To study the experience of exercise in a longitudinal manner, participants completed three individual 30-minute interviews—one at baseline, after week 1, and after week 2—totaling 90 minutes for each of the ten participants.
To capture “real-time” thoughts and reduce the influence of recall bias relating to exercise in this population, journals were also mailed to participants prior to the study, with instructions to write in the journal any time they thought about exercise or participated in exercise, and how T1D affected their exercise experience during the 2-week study period.
Data Analysis
All qualitative data sources (blog posts including associated comments, interview transcripts, and exercise journals) were imported into qualitative data analysis management software (NVivo, QSR International; Burlington, MA). The study team employed an inductive thematic approach25-28 to construct themes represented in the data. Blog data were analyzed separately from interview and journal data to allow comparison of themes derived from each method, and especially from the traditional sources (interviews and journals), to the more novel approach of utilizing blogs. Primary coders (TKO, SMO) reviewed the data and noted initial impressions. For each of the three data source types, a preliminary codebook was created and revised through ongoing discussions among the study team, establishing a basis for coding procedures by all. After coding 10% of the datasets, Cohen’s kappa was calculated as one method to assess intercoder reliability; Cohen’s kappa is a measure that incorporates how frequently multiple coders agree that a given code applies to a segment of data and how frequently they agree that a given code does not apply to a segment of data. 29 Kappa was calculated for each dataset and found to be high (0.911-0.958). With intercoder reliability established, the remainder of the datasets were coded, proceeding until saturation was established (when the primary coders determined that no new codes or themes were being uncovered, subsequently corroborated by the full study team). Undertaking an inductive approach to determine emergent themes, the team performed a detailed review of coded content to identify frequently utilized codes as well as pairs of codes frequently appearing together to construct themes occurring within the datasets. As themes were determined separately for each type of data source, any metatheme reported as existing in all data source types must have been present independently as a theme in each of those source types. In other words, a metatheme reported as existing across all source types must have been independently identifiable as a theme within the blog data, within the interview data, and within the journal data. Likewise, a theme from the blog data which was supported by only one or two comments in the interviews and the journals would not satisfy this criterion to be a metatheme.
Results
Data Sources and Participants
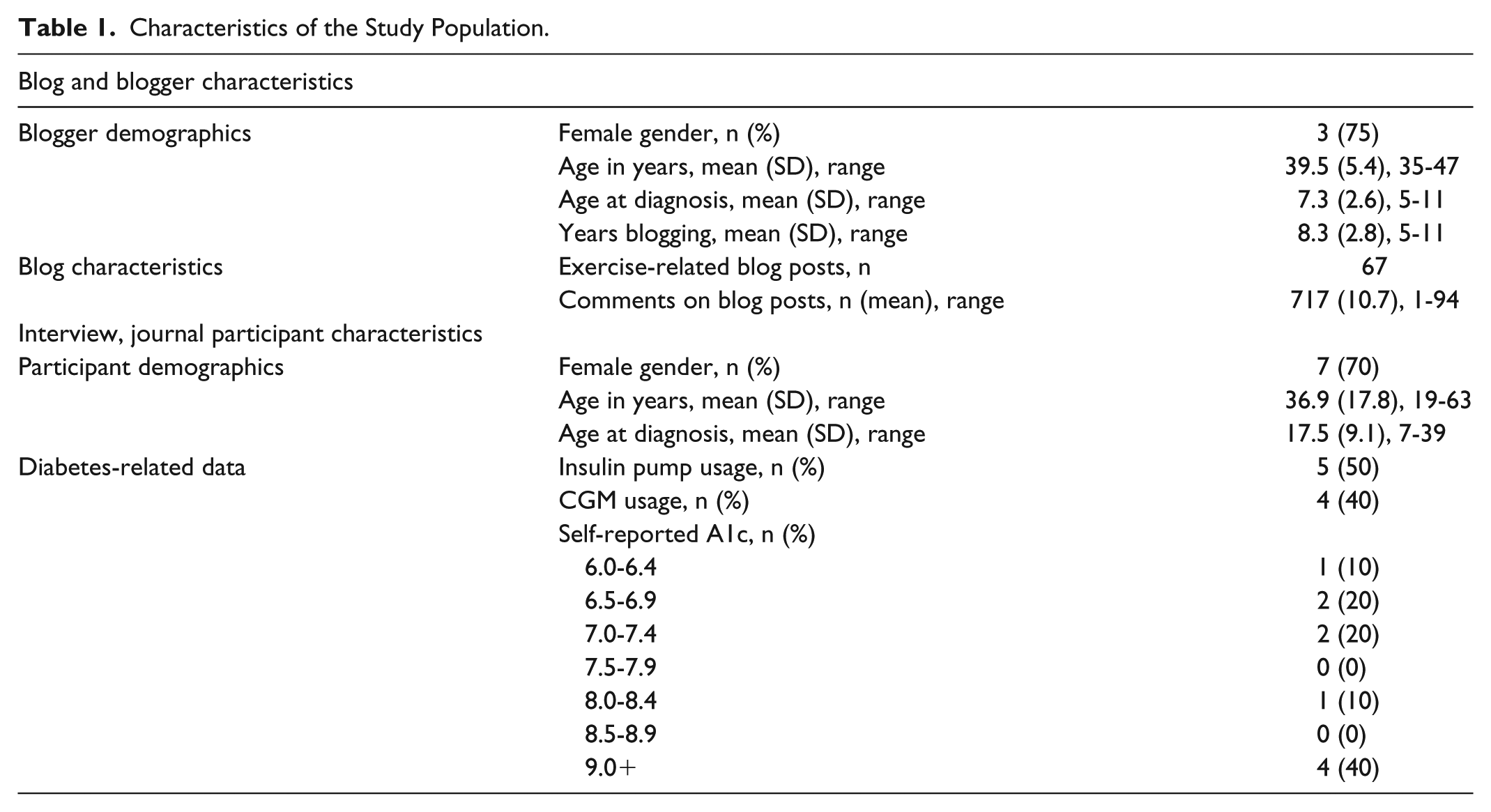
Table 1 summarizes characteristics of the study population. Sixty-seven blog posts and 717 associated comments were analyzed. Ten participants engaged in three 30-minute interviews each (totaling thirty 30-minute interviews) and provided 100 journal entries (mean 10.0, range 2-17, SD 5.75) over a 14-day period. Interview and journal participants ranged in age from 19-63 years (mean 36.9, SD 17.8). Average age at T1D diagnosis was 17.5 years (range 7-39). Participants were predominantly female (70%), with 50% using an insulin pump and 40% using a continuous glucose monitor (CGM) system. This information was not available for bloggers or commenters.
Characteristics of the Study Population.
Data Analysis
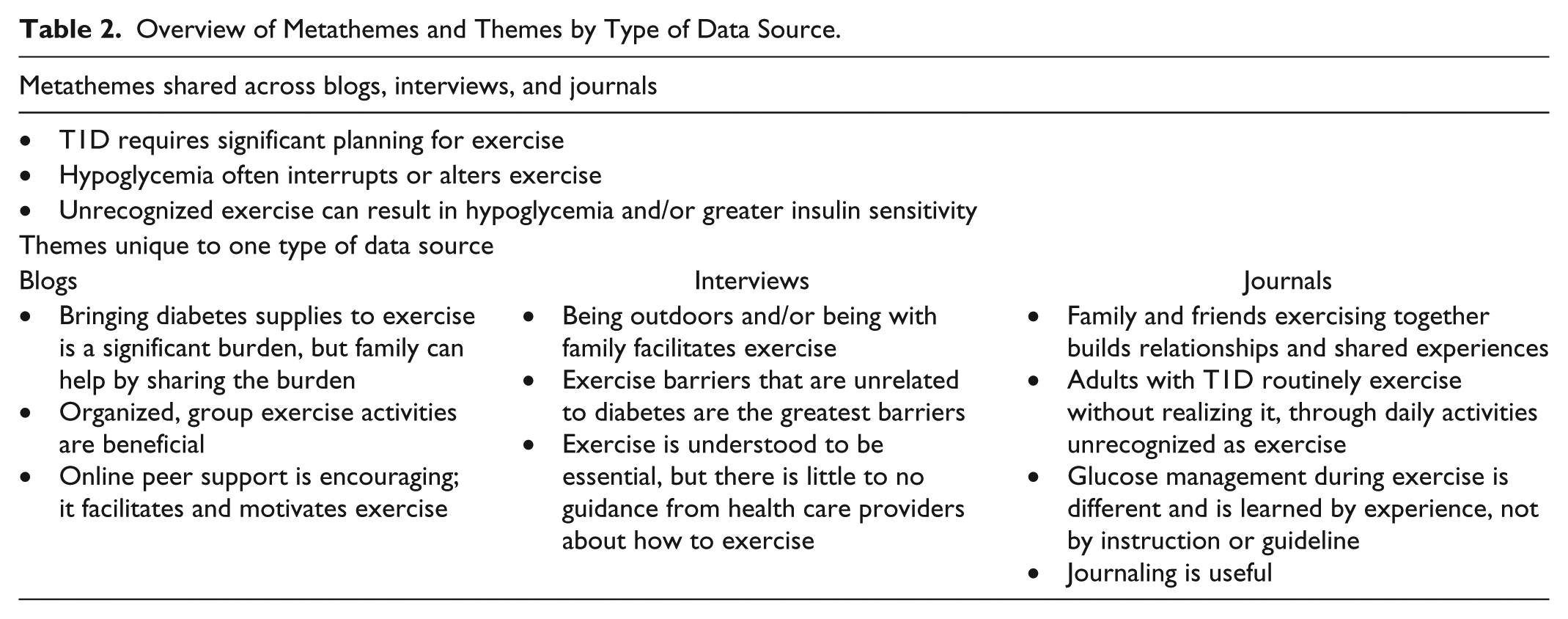
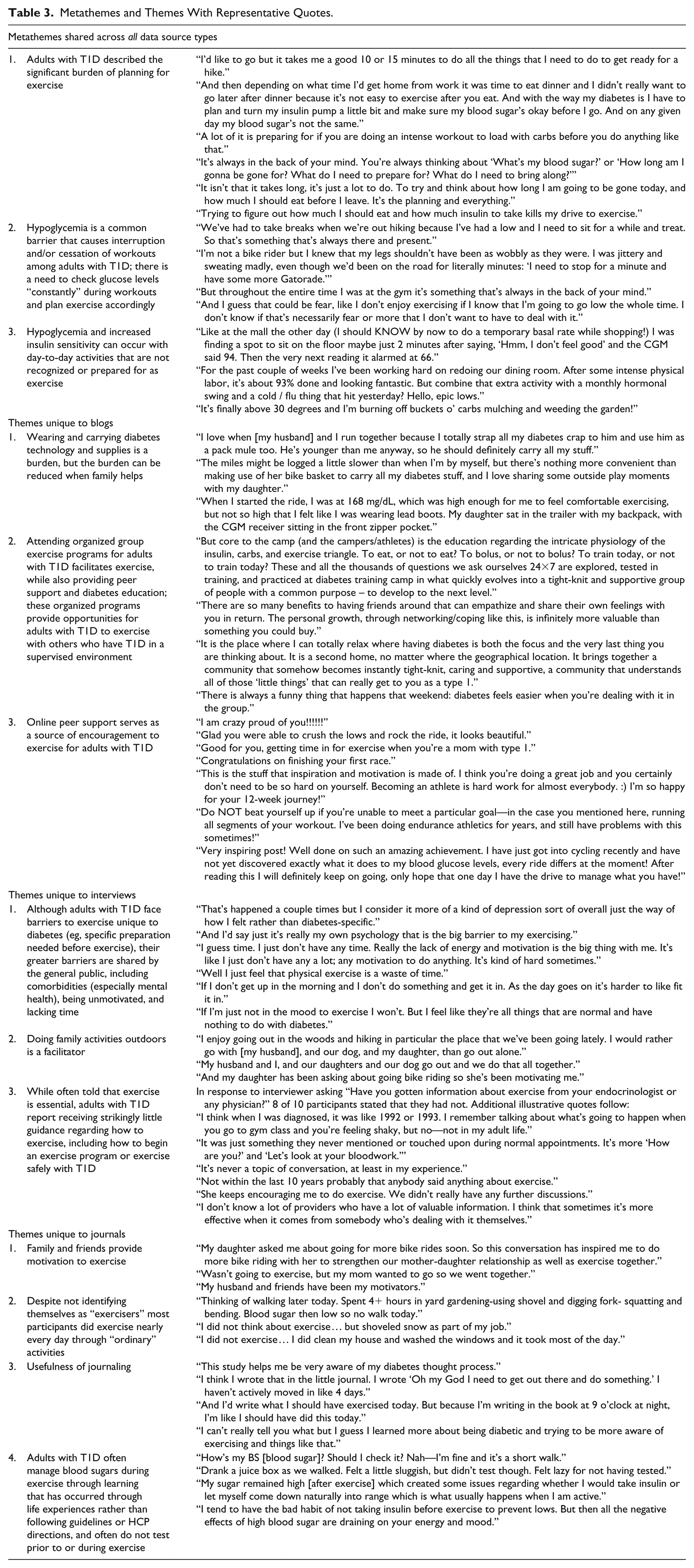
Thematic analysis revealed metathemes shared across blogs, interviews, and journals, as well as themes unique to each data source type. Even where similar topics were discussed (ie, content coded to the same topic area), the nuanced meanings captured in the themes sometimes differed by data type. The metathemes and themes by data type are summarized in Table 2 and fully presented with representative quotes in Table 3.
Overview of Metathemes and Themes by Type of Data Source.
Metathemes and Themes With Representative Quotes.
Analysis resulted in three metathemes present across all data source types: (1) adults with T1D feel that exercise requires significant planning, (2) hypoglycemia often interrupts exercise, or causes adults with T1D to have to alter their planned exercise, and (3) “ordinary” activities can cause greater insulin sensitivity and hypoglycemia, similar to planned exercise. These are discussed in greater detail below.
Adults With T1D Feel That Exercise Requires Significant Planning
In all three data sources, people describe the amount of planning that they must perform to feel that they can exercise, and how this can be a deterrent to exercising: “It’s always in the back of your mind. You’re always thinking about ‘what’s my blood sugar?’ or ‘How long am I gonna be gone for? What do I need to prepare for? What do I need to bring along?’” Participants identified that it is not the time needed to plan, but the emotional burden of having to plan: “It isn’t that it takes long, it’s just a lot to do. To try and think about how long I am going to be gone today, and how much I should eat before I leave. It’s the planning and everything.” As one participant succinctly summarized when discussing the emotional burden of preparation needed to exercise: “Trying to figure out how much I should eat and how much insulin to take kills my drive to exercise.”
Hypoglycemia Often Interrupts Exercise or Causes Adults With T1D to Have to Alter Their Planned Exercise
Through the incorporation of blogs, interviews, and journals, we found that participants did not describe fear of hypoglycemia as much as the burden of having exercise interrupted or changed due to hypoglycemia: “I had to not work out as hard as I wanted, to keep my blood sugar from dropping below 80 before class was over. It was very frustrating and agitating that I couldn’t do the workout I wanted because of my diabetes.” Even when asked directly about fear of hypoglycemia, one participant responded: “I don’t know if that’s necessarily fear or more that I don’t want to have to deal with it.” They described the impact of hypoglycemia on family activities (“We’ve had to take breaks when we’re out hiking because I’ve had a low and I need to sit for a while and treat. So that’s something that’s always there and present”), as well as the burden of constantly having to think about the possibility of low blood glucose (“Throughout the entire time I was at the gym it’s something that’s always in the back of your mind”).
“Ordinary” Activities Can Cause Greater Insulin Sensitivity and Hypoglycemia, Similar to Planned Exercise
This analysis of three data sources demonstrated that although adults with T1D may not exercise on a regular basis, they are often physically active: “I did not exercise—I did clean my house and wash windows (it took me most of the day).” Such activities unrecognized as “exercise” were also associated with unexpected hypoglycemia: “Like at the mall the other day (I should KNOW by now to do a temporary basal rate while shopping!) I was finding a spot to sit on the floor maybe just 2 minutes after saying, ‘Hmm, I don’t feel good’ and the CGM said 94. Then the very next reading it alarmed at 66.” At times, planned exercise was prevented by hypoglycemia resulting from other physical activity not recognized as exercise: “Thinking of walking later today. Spent 4+ hours in yard gardening—using shovel and digging fork—squatting and bending. Blood sugar then low so no walk today.”
In addition to metathemes, each data source identified unique themes that were often interrelated, as demonstrated in Figure 1. For instance, family was identified as a facilitator to exercise among blogs, interviews, and journals, but the more specific way in which family was helpful differed among the sources: blogs identified family as helping to decrease the burden of carrying diabetes supplies during exercise; interviews identified family as facilitators through exercising together outside; and journals identified family as motivating to exercise. In addition, facilitators identified through one data source presented opportunities to decrease barriers identified by another source. For instance, interviews and journals respectively identified potential barriers in lack of exercise information from health care providers (HCPs) and “winging it” (improvising, making decisions and adjustments based on experience, intuition, trial, and error) with diabetes management during exercise, yet blogs identified a facilitator in organized T1D activities as a possible avenue to obtain education and practice problem solving in a safe environment.
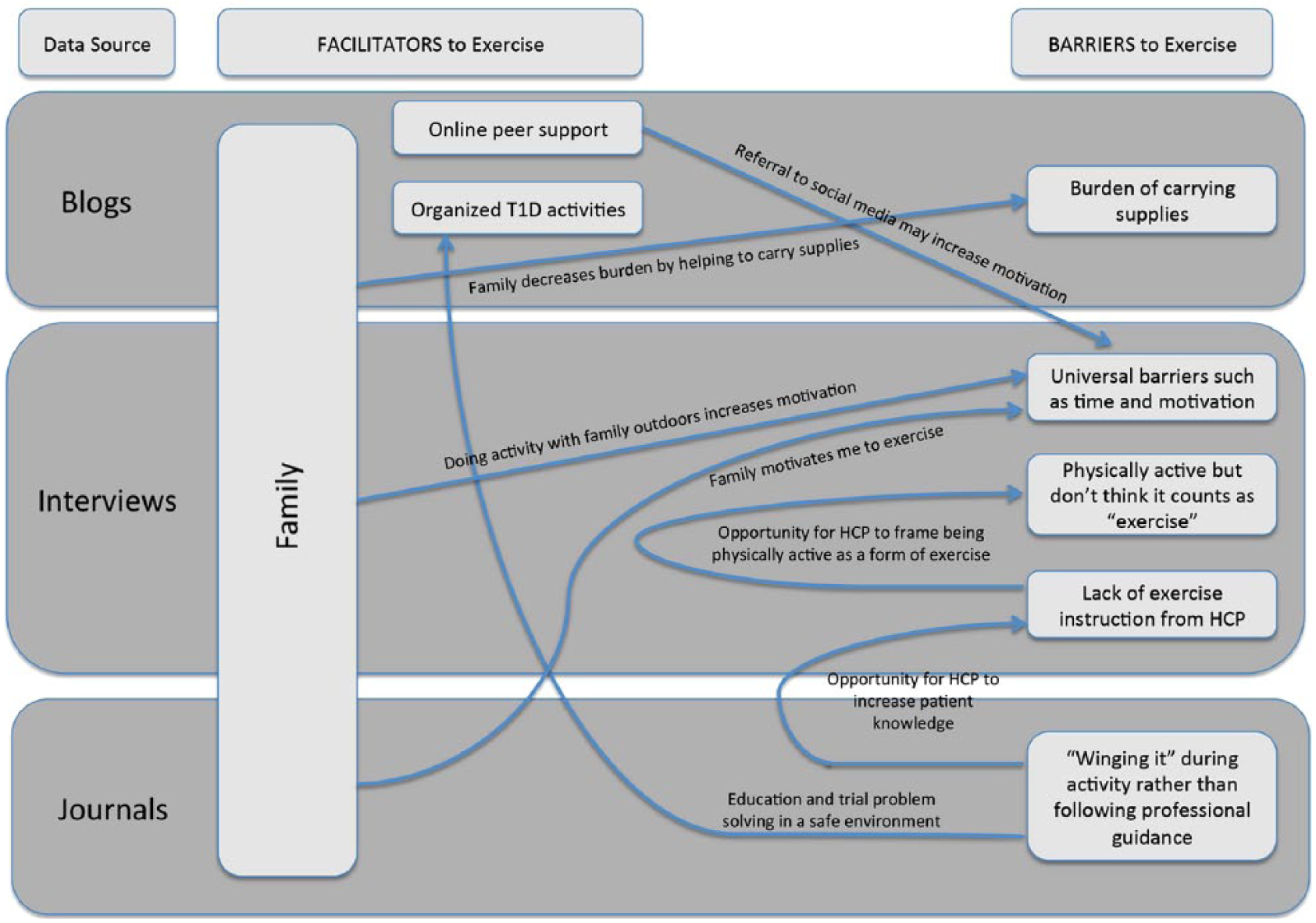
Concept map of themes relating to barriers and facilitators to exercise with type 1 diabetes, by data source.
Discussion
This qualitative study uses the addition of social media through the inclusion of blogs to supplement traditional methods such as interviews and journals. Through combining three sources of data, themes identified in this research add to the growing body of literature on barriers and facilitators to exercise in adults with T1D. Clear guidelines now exist for exercise management, including glucose targets, nutritional, and insulin dose adjustments to help prevent exercise-related glucose excursions. 4 Yet many adults with T1D do not meet the ADA’s recommendations for exercise. 3 This study agrees with others that hypoglycemia is a major barrier to exercise, yet unlike in our previous work involving caregivers to children with T1D 22 and others who cite fear of hypoglycemia as a barrier,4,11,12 participants in this study seemed to be more burdened by the effect of low blood glucose on their ability to complete their exercise as planned. We agree with Campbell et al 30 that many adults with T1D are active through daily living and recreational activities even though HCPs and adults with T1D alike may not identify this as exercise, and therefore unexpected hypoglycemia can occur. Like Kime et al, 14 we found that adults were often “winging it” when exercising with T1D, with little to no guidance from HCPs. Family was found to be an important facilitator across all three data sources and helped not only to decrease burdens associated with diabetes (eg, carrying equipment while exercising), but also helped by participating in exercise together, as well as motivating adults with T1D to exercise. Consistent with prior studies,11,12 this study found that adults with T1D feel safer and more comfortable exercising when they are with a group of others who also have T1D, noting a sense of shared experience and knowledge that only comes from living with T1D.
This work supports the development of a model applying social and behavioral modification problem solving strategies31-33 to the barriers adults with T1D face in relation to exercise. HCPs can help increase adult with T1D preparedness and engagement in exercise through the steps of general orientation, problem definition and formulation, generation of alternatives, decision making, and verification.31-33 HCPs and adults with T1D share a mutual role in identifying and validating that there are issues related to exercise (general orientation). HCPs can then aid in identifying individualized problems facing the adult with T1D in relation to exercise engagement (problem definition and formulation), for example, becoming hypoglycemic on a family bike ride. Next, HCPs can help the adult with T1D brainstorm ways to be prepared for managing hypoglycemic events (generation of alternatives) and then help them examine several of the alternatives to identify which may be most effective and realistic (decision making). HCPs with ongoing patient relationships are perfectly poised to check in at follow-up visits, assess effectiveness of the strategies (verification), and negotiate how best to modify them for the future. Through problem solving, HCPs can better prepare adults with T1D for exercise by using their expertise to share a variety of response alternatives for dealing with potential problematic situations 31 (eg, a handout listing specific foods and quantities to promptly treat hypoglycemia, a list of available online T1D social networking groups to learn from others’ experiences, or education about insulin dose adjustment), and thereby increase the likelihood that adults with T1D will select the most personally effective responses from among these alternatives. 31 Implementing this model could increase activity in those who are inactive and reinforce persistence in those already exercising—a potential area for future research.
To our knowledge this is the first social media study to use blog analysis specifically to conduct a qualitative analysis of exercise habits among adults with T1D. Blog content is publicly available and freely shared and is not constrained by interview scripts, questionnaires, or other traditional methods of data collection. Bloggers and commenters are unaffected by researcher bias, as their content is not based on what they believe a researcher wants to know or hear. Nor are they asked to think back retrospectively, and somewhat artificially, to previous experiences. Instead, blogs provide a near real-time glimpse into the attitudes and emotions around a specific topic. In the blogs analyzed in this study, bloggers wrote about same-day or recent experiences they had while being physically active, and commenters responded as they read the blog posts. Since blogs are public and meant to be shared, perhaps this helps explain why some of the themes found in the blog analysis are more group-oriented, including the helpfulness of organized exercise activities, diabetes camps, and—especially online—peer support.
This study also revealed that blogs themselves provide support and encouragement for adults with T1D to be physically active. One reason people with T1D turn to the DOC is to receive much-needed peer support that is traditionally missing from their diabetes care.23,34-35 With this information, HCPs can encourage adults with T1D to find a T1D-dedicated exercise group or to join the DOC and read blogs. The use of social media, such as blogs, can be an important source of information in research studies such as this, but can also provide HCPs with a lens through which to learn what the daily life of those living with T1D encompasses and thereby to deliver more highly personalized patient-centered care.
Also evident from this work is the advantage to using a combination of source types to form a more complete picture of the issues faced by the target population. Specifically, the findings of metathemes found across blogs, interviews, and journals strengthens the use of each modality as a qualitative data source. And the finding of unique themes from each, whether highly different or whether resembling each other but with important nuance in the differences, highlights the utility of employing multiple modalities to complement each other.
Limitations of this research include a relatively small sample size and lack of generalizability—but these are common limitations in qualitative research. 25 We tried to balance the impact of sample size by including the broader array of source types: blogs (including blog posts as well as comments), interviews, and journals. Blogger participants were motivated to publicly share their successes and challenges, and thus may not represent the general population of adults living with T1D. It is also impossible to know many characteristics of the people who contributed to the blog content, such as demographics and insulin pump use or CGM use; this is an inherent limitation of anonymous online sampling and of blogs as a medium. The participants that were interviewed were recruited from one hospital system and their views may not represent those of the broader adult T1D population. However, including both groups should reduce concerns about generalizability compared to including only one or the other.
Future research is needed to develop and evaluate interventions to help adults with T1D overcome the barriers identified in this and earlier studies so that they can achieve the recommended amount of exercise. Such future interventions could target efforts to involve family, peer-led initiatives, and HCP delivery of information not only about the importance of exercise, but also recommendations about how to exercise safely with diabetes, as well as what constitutes exercise (including activities not typically recognized as exercise but which can still result in hypoglycemia).
Conclusions
This study demonstrates that the use of technology in the form of social media (blogs), in addition to interviews and real-time journaling, can provide a fuller understanding of the barriers and facilitators associated with exercising with T1D. This information can contribute to supporting and educating people with T1D by providing them with recommendations for safe exercise practice and preventing hypoglycemia during exercise. These findings also support the need for future research to continue to study this population, as the themes yielded from the qualitative data analysis present various opportunities for improvement in exercise management for adults with T1D.
Footnotes
Abbreviations
ADA, American Diabetes Association; CGM, continuous glucose monitor; DOC, Diabetes Online Community; HCP, health care provider; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under Award Number DP3DK104054. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.