
Abstract
Background:
There is a lack of systematic ways to analyze how diabetes patients use their insulin pumps to self-manage blood glucose to compensate for alcohol ingestion and exercise. The objective was to analyze “real-life” insulin dosing decisions occurring in conjunction with alcohol intake and exercise among patients using insulin pumps.
Methods:
We recruited adult type 1 diabetes (T1D) patients on insulin pump therapy. Participants were asked to maintain their daily routines, including those related to exercising and consuming alcohol, and keep a 30-day journal on exercise performed and alcohol consumed. Thirty days of insulin pump data were downloaded. Participants’ actual insulin dosing behaviors were compared against their self-reported behaviors in the setting of exercise and alcohol.
Results:
Nineteen T1D patients were recruited and over 4000 interactions with the insulin pump were analyzed. The analysis exposed variability in how subjects perceived the effects of exercise/alcohol on their blood glucose, inconsistencies between self-reported and observed behaviors, and higher rates of blood glucose control behaviors for exercise versus alcohol.
Conclusion:
Compensation techniques and perceptions on how exercise and alcohol affect their blood glucose levels vary between patients. Improved individualized educational techniques that take into consideration a patient’s unique life style are needed to help patients effectively apply alcohol and exercise compensation techniques.
Keywords
Diabetes mellitus is a complex, chronic disease affecting 29.1 million (9.3%) US residents. 1 Chronic hyperglycemia can result in potentially devastating microvascular and macrovascular complications, leading to major morbidity, mortality, and economic consequences in this patient population. Evidence demonstrates that these complications can be prevented by maintaining glycemic control to near normal levels. Achieving and maintaining adequate glycemic control requires consistent medical care, and most importantly, ongoing patient self-management. 2
While evidence shows that alcohol and exercise affect the absorption of insulin and increase the risk of hypoglycemia, there is a lack of evidence-based decision tools to allow for translation of this information into practice.3-6 Patients with type 1 diabetes (T1D) must manage their disease by injecting insulin deliverable through syringes, insulin pens, or insulin pumps. Premeal insulin dosage compliance and accuracy is a key factor in achieving target postprandial glucose levels. In 2013 insulin pumps were being used by over 350 000 people in the United States, 7 incorporate proprietary mathematical algorithms called bolus calculators or bolus wizards to determine individualized premeal dosing.8-10 The benefits achieved through the use of insulin pumps and continuous glucose monitors (CGMs) are not necessarily a direct result of wearing the devices but rather due to behavioral and management changes enabled by the information provided by the devices to the users. 11 While bolus calculators and CGMs can lead to better glucose control,12,13 bolus calculators currently cannot account for the lifestyle complexities of alcohol ingestion and planned exercise.14-20
A review of the literature demonstrated a lack of systematic studies analyzing adult T1D patients’ self-reported behaviors against their actual behaviors documented from data collected by an insulin pump. Better understanding of these behaviors could help in the design of individualized educational programs, particularly as relates to intensive insulin therapy, and aid in designing better dosing algorithms that account for behaviors related to alcohol consumption and exercise patterns. The aim of this study was to analyze adult T1D patients self-reported versus actual self-management behaviors occurring in conjunction with alcohol intake and exercise.
Materials and Methods
Subject Recruitment
After Institutional Review Board approvals, 19 adult T1D patients were recruited from an academic outpatient endocrinology clinic. Participants were between the ages of 18 and 70, nonpregnant, and English speaking and had been using an insulin pump from a single vendor for at least 1 year. Patients in fragile health, limited life expectancy, a history of mental health problems, advanced vascular disease or microvascular complications, and known history of severe hypoglycemia were excluded. Study personnel identified potential subjects at the time of their scheduled outpatient visit. Subjects were handed a flyer that provided details on the study.
Data Collection
The study team conducted structured interviews to collect participants’ self- reported perceptions of how alcohol and exercise affected blood glucose levels and the sources of information they had used to learn about these interactions. In addition, subjects were asked if they accounted for alcohol and exercise in their insulin dosing decisions, and what type of techniques they used to compensate for these behaviors (eg, carbohydrate consumption, reduction in insulin bolus or basal rate, or some combination of these methods).
Participants were asked to maintain their daily routine, and to keep a journal on the time, duration and intensity of exercise performed (eg, at 9:00
The study team also obtained the data contained within the participants’ insulin pump during the same 4-week period. The patients uploaded the insulin pump data through a website provided by the insulin pump’s manufacturer, which was remotely accessed by study personnel. Once the data were downloaded the patients were encouraged to change their passwords. Alternatively, patients could meet in person with a member of the study team who could download the data from the patients’ insulin pump.
Data Analysis
Subjects’ perceptions of the effect of alcohol and exercise on glucose levels and their sources of information regarding alcohol and exercise were tabulated. Data from the paper-based diaries were electronically coded and analyzed to quantify for each study participant number of drinks and frequency of exercise. To report patients’ observed behaviors for exercise and alcohol we reviewed data downloaded from the insulin pumps and from the participants’ paper-based diaries to quantify how often patients used techniques to compensate for alcohol ingestion and exercise activity, such as adjusting insulin (basal rate or bolus) or taking a snack within 30 minutes before exercising. Computer algorithms were written to associate self-reported days and times of alcohol consumption and exercise to the corresponding data collected by the insulin pumps. Using the aggregated data the frequency of compensation techniques related to carbohydrate consumption, insulin boluses delivered, and blood glucose monitoring occurring in close temporal proximity to exercise or alcohol consumption was computed for each study participant. Close temporal proximity was defined as ±30 minutes of alcohol consumption or exercises.
Results
Demographics
Nineteen subjects with T1D were recruited. Mean (SD) age was 48 (15) years, 12 were women, and 18 were of white race. Mean (SD) hemoglobin A1c was 7.3 (1.0)%, self-reported duration of diabetes was 27 (13) years, and duration of insulin pump therapy was 11 (5) years. Seven participants wore a CGMS, and the remaining used capillary glucose monitoring. There were 4249 interactions between the study participants with the insulin pump bolus calculator analyzed. There were 347 exercise events recorded by 17 participants and 155 alcohol events recorded by 11 participants.
Perceived Interactions and Sources of Alcohol and Exercise Information
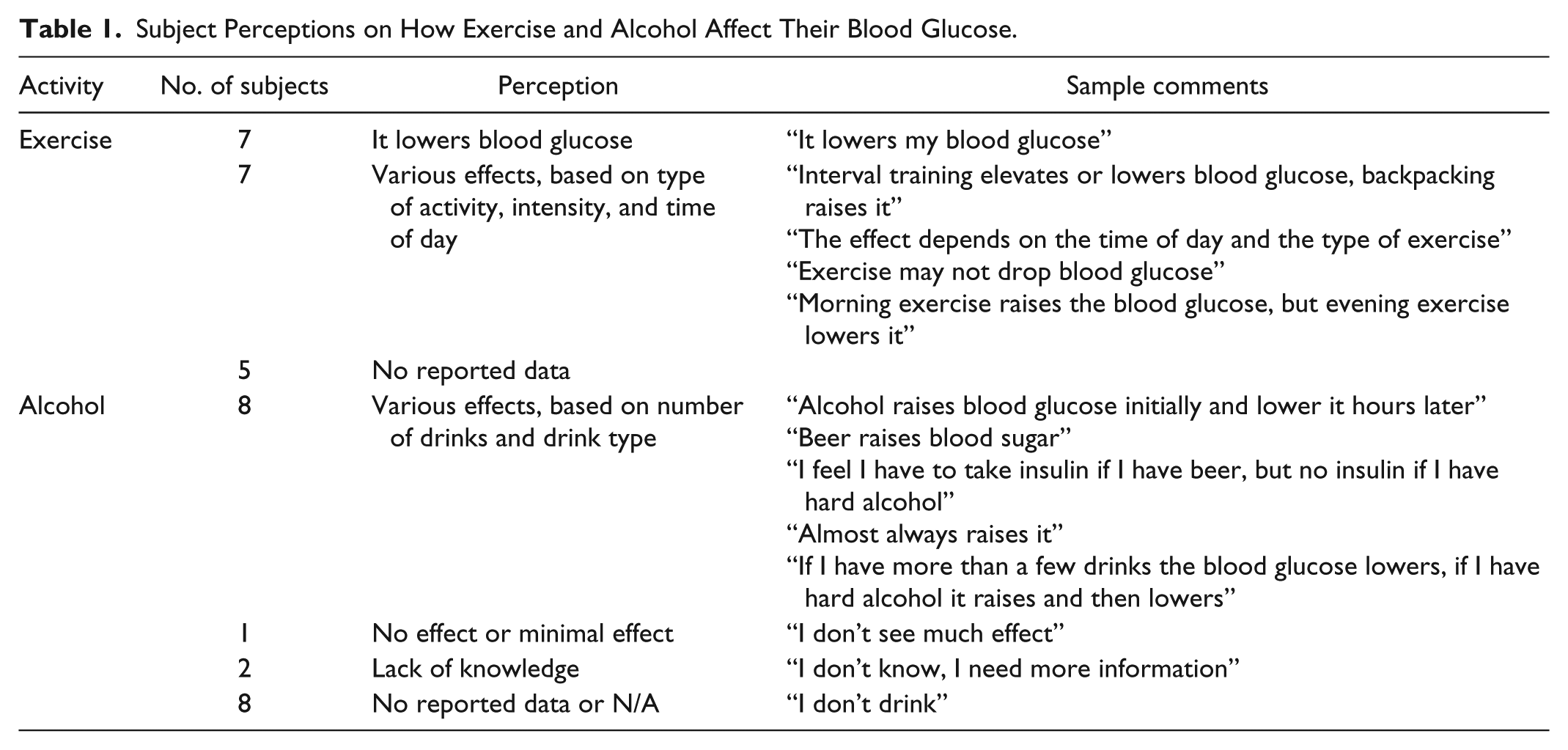
When subjects were asked about how alcohol or exercise impacted their glucose control, there were no consistent responses observed (Table 1). There were 7 participants who all stated that exercise lowers blood sugar independently of the type and time of exercise, another 7 whose responses varied on how glucose reacted to different exercise types (variety of endurance, athletic, aerobic, and anaerobic types of exercises were mentioned) and times (eg, morning, evening), and another 5 without responses. With respect to alcohol (Table 1), 8 participants stated that their reactions to alcohol depended on factors like the number of drinks (eg, only compensating when consuming 2 or more drinks) or type of drinks (eg, differentiating between drinks with high or low alcohol concentration), 1 who stated there was no effect on glucose, 2 who did not know, and 8 who did not respond.
Subject Perceptions on How Exercise and Alcohol Affect Their Blood Glucose.
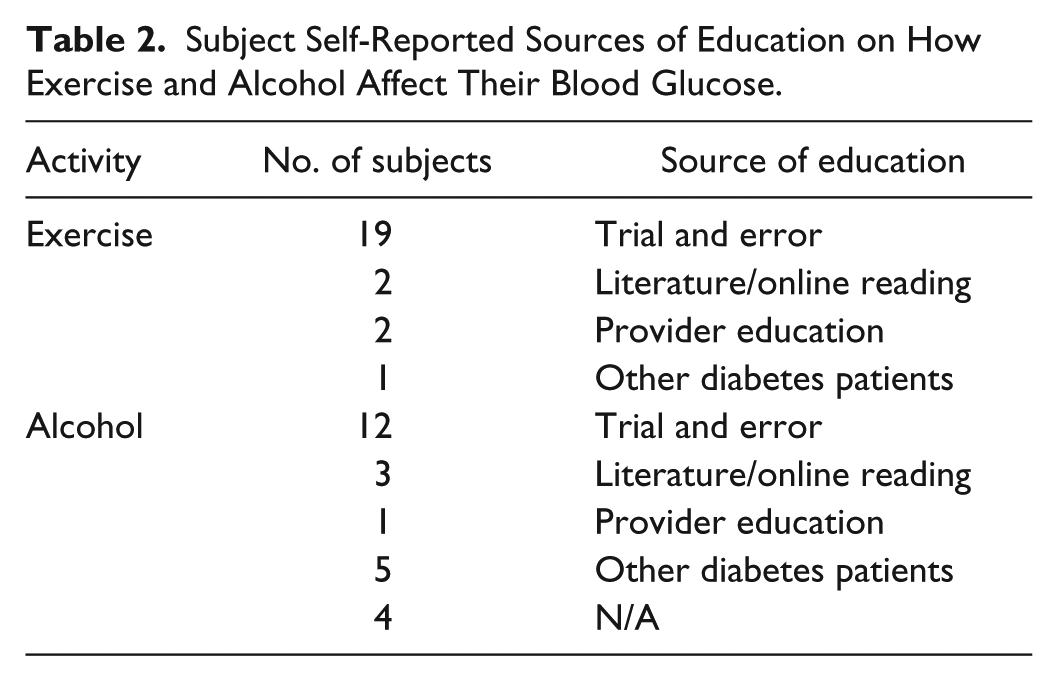
Participants also reported deriving information on how exercise and alcohol affected their blood glucose from a number of different sources (Table 2). Most participants indicated they learned about the interactions from trial and error and had developed their own heuristics. Few participants reported having received information or education from providers on approaches to compensate for alcohol or exercise when self-managing blood glucose. Two participants indicated that they would like to receive more information on the way alcohol affects blood glucose.
Subject Self-Reported Sources of Education on How Exercise and Alcohol Affect Their Blood Glucose.
Overall Self-Management Behaviors
Current American Diabetes Association (ADA) Standards of Care Guidelines suggest that patients should consider checking blood glucose prior to exercise and recommend that to avoid hypoglycemia the insulin dose and/or carbohydrate intake may need to be altered. 21 Many health care organizations suggest that alcohol should be consumed with a meal containing carbohydrates to avoid hypoglycemia.22-24 Data entered into the subjects’ insulin pumps indicated self-management techniques did not match current recommendations (Figure 1). When comparing self-management techniques for exercise versus alcohol, participants consumed carbohydrates (40.9% vs 20.6%), delivered an insulin bolus (38.3% vs 26.8%), or checked their blood glucose (60.7% vs 27.3%) more consistently with exercise than when consuming alcohol.
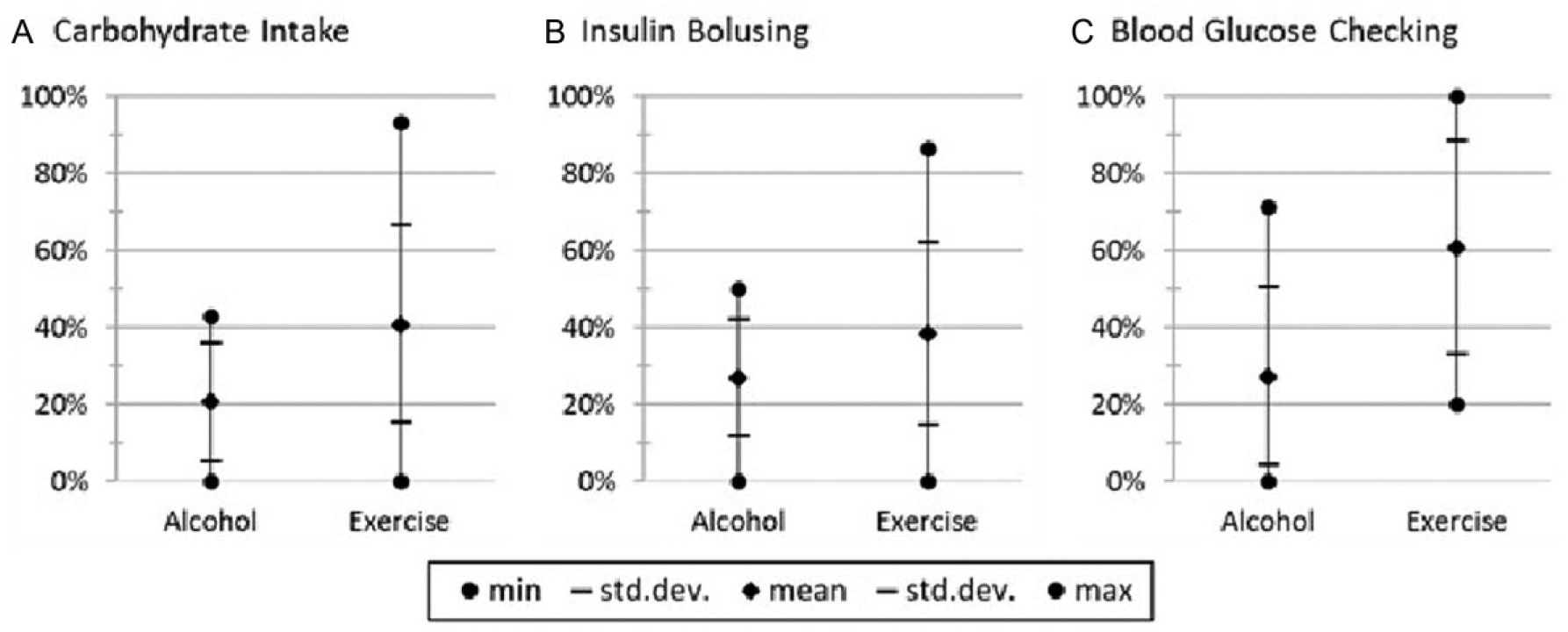
(A) Carbohydrate intake, (B) insulin bolusing, and (C) blood glucose checking within ±30 minutes of exercise or alcohol consumption. For instance, as depicted in (A), in temporal proximity of alcohol events subjects consumed carbs with 20.6% mean, 15.3% standard deviation, and 0-42.9% range. In contrast, in proximity to exercise events subjects consumed carbs with 40.9% mean, 25.5% standard deviation, and 0-93.3% range.
Similar to Hendricks et al, 25 study participants’ adherence to ADA recommendations for alcohol consumption and exercise 21 were quantified. According to the guidelines “adults with diabetes should be advised to perform at least 150 min/week of moderate-intensity aerobic physical activity (50-70% of maximum heart rate), spread over at least 3 days/week with no more than 2 consecutive days without exercise.” Weekly adherence to this guideline by study participants was 38.4% (45.4), with 5/17 subjects reporting 100% adherence and 10/17 subjects at 0%. The ADA also recommends “adults with diabetes who drink alcohol should do so in moderation (no more than one drink per day for adult women and no more than two drinks per day for adult men).” The mean (SD) adherence to the ADA guidelines for daily alcohol moderation was 94.6 (9.2)% within the range of 70 to 100%.
Observed Versus Actual Behaviors Associated With Exercise and Alcohol
Next we contrasted subjects’ reported self-management techniques against observed behaviors for exercise and alcohol, as derived from analysis of corresponding data contained with the subjects’ insulin pumps. Self-described compensatory self-management techniques for exercise and alcohol consumption were categorized as no compensation, adjusting insulin (reducing basal rates or boluses), ingesting snacks, or removing the pump. When examining behaviors related to exercise, discordance was seen between what subjects claimed they did versus actual behavior. For instance, 16 subjects reported they would adjust insulin pump settings when exercising, while only 7 were observed to have done so (Table 3). Another 2 indicated they would take a snack, but 5 were noted to employ this technique. While 2 study participants reported always adjusting basal insulin, no patients were observed always adjusting their basal settings. Although 2 patients reported sometimes removing the pump during exercise, the pump disconnection was not explicitly recorded in the insulin pump data we had access to, hence we were not able to quantify this behavior.
Patient Self-Reported Compensation Techniques and Observed Behaviors for Exercise and Alcohol.
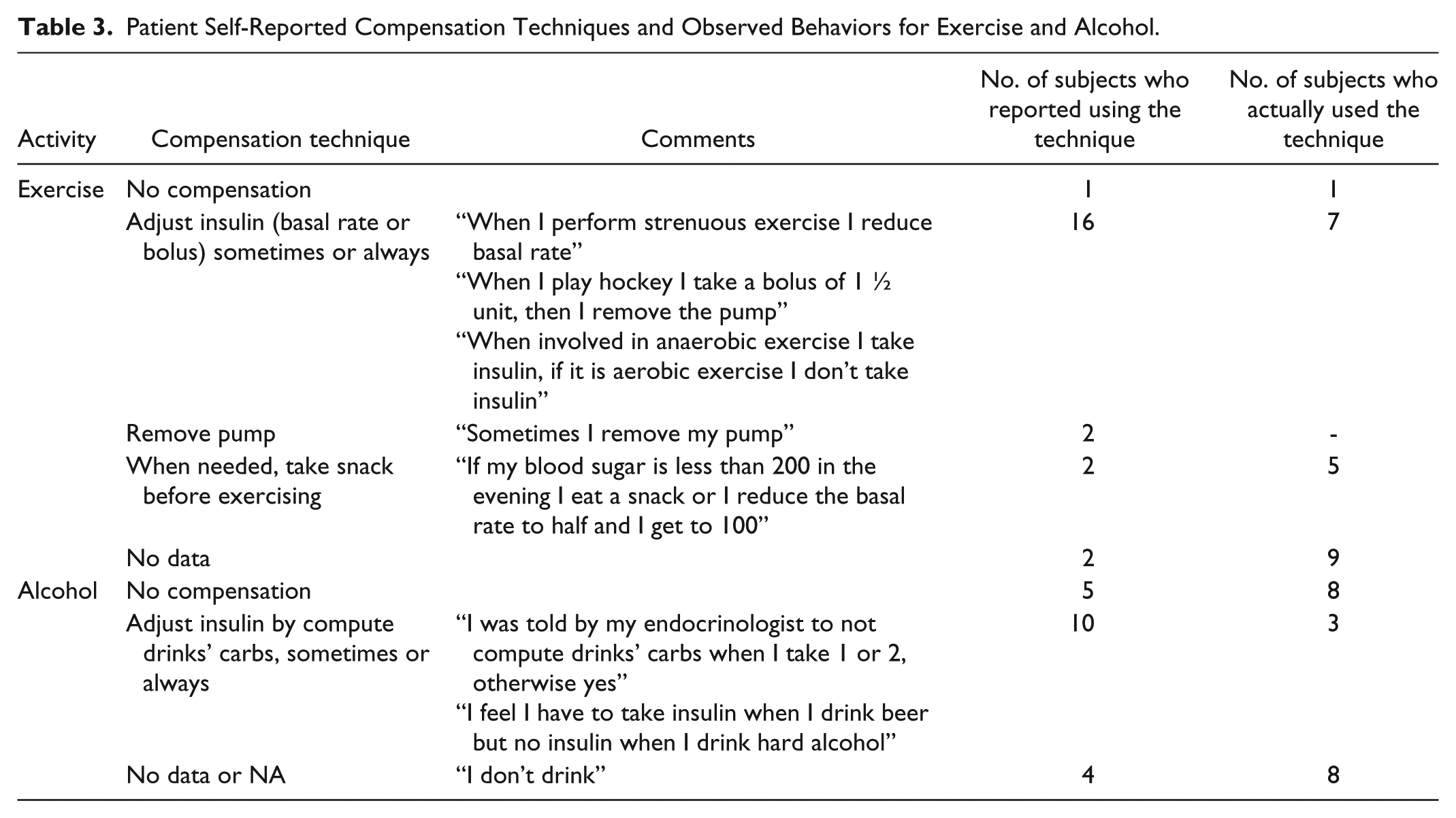
Similar discrepancies were noted between what subjects said they would do and what they actually did when reviewing self-management behaviors related to alcohol ingestion (Table 3). For example, 5 subjects indicated they would not compensate for alcohol use, while 8 were actually observed not making any adjustments. There were 10 subjects who indicated they would adjust insulin when drinking alcohol, but only 3 were noted to have done so.
Discussion
Qualitative studies of children, adolescent, and adult diabetes patients have been performed with the purpose of understanding behavioral diabetes care.25-29 While in general qualitative studies are limited by small sample sizes and do not generate statistically significant data, their findings are crucial to give a glimpse into patients’ beliefs, attitudes, behaviors, culture, and lifestyle. With diabetes in particular, understanding patients’ behaviors is very important to discover the reasons behind nonadherence to treatment or poor glycemic control, and to identify the best ways to deliver effective interventions.
With respect to self-care, qualitative studies have shown that many patients lack understanding of how medications, food, and exercise affect blood glucose control and what kind of information needs to be taken into account (carbohydrate content of food, activity level, etc) to self-manage diabetes effectively.30,31 In terms of physical activity, the qualitative study by Hendricks et al interviewed 49 emerging adults (18 to 26 years old) to understand their exercise habits and to determine their compliance with the ADA recommendations on physical activity. 25 The ADA recommends at least 30 minutes of daily physical activity for youth. In the Hendricks et al study 25 41% of participants engaged in exercise at least once daily; 55% of those individuals who engaged in daily exercise demonstrated a mean duration of 30 minutes or more. Mean exercise duration was 29.56 minutes/day and ranged from 0 to 157 minutes.
To eliminate inaccuracies from self-reported data and to obtain statistically significant results by increasing the sample sizes, quantitative studies are taking full advantage of the data generated by diabetes technology as was conducted here. Blood glucose monitors, CGMs, and insulin pumps can objectively store data that reflect what patients actually do, as opposed to what patients say they are doing (self-reported data). Driscoll and Young-Hyman 32 provide a detailed review of the use of such technology in assessing adherence to diabetes self-management behaviors. Their 2014 review focused on patients’ adherence to the ADA Clinical Practice Recommendations 33 with an emphasis on studies that assessed patient adherence to glucose monitoring, insulin administration, medical nutrition therapy, and physical activity. The review by Driscoll and Young-Hyman did not discuss alcohol consumption. In terms of physical activity, their review highlighted the lack of studies that quantify physical activity and suggest the future use of accelerometers to objectively measure physical activity.
The goal of this study was to address the lack of systematic qualitative and quantitative studies to understand adult T1D patients’ self-management practices occurring in conjunction with alcohol intake and exercise. Results indicated that subjects varied in their understanding of how exercise and alcohol affected their glucose control, and in how they compensated for the impact of these common lifestyle choices in their diabetes management. These results are consistent with patients’ trial and error approaches to fine-tune self-management techniques based on unique personal and situation specific factors that affect blood glucose control in the presence of alcohol and exercise. In addition, there was no one means by which they obtained information on these important topics. Documented adjustments in carbohydrate intake, insulin doses, and glucose monitoring occurred at frequencies lower than what might be expected. In the case of alcohol consumption, very few instances of changes in self-management behavior were noted.
The results demonstrate the need for a revision of current educational strategies to help patients incorporate their personal lifestyle preferences into proper alcohol and exercise compensation techniques. A number of approaches could be utilized, such as the use of social media, or incorporating more individualized training during diabetes self-management education sessions. Another approach could be the development of software applications (apps) that assist patients in making decisions about how to change carbohydrate intake or adjust insulin doses in the event of an exercise or alcohol event. An automatic approach to help prevent hypoglycemic events, including those caused by exercise or alcohol, is to incorporate into insulin pumps a threshold suspend feature that is designed to automatically stop insulin delivery when the blood glucose sensor value reaches or falls below a patient-specific preset threshold.
Further research will be needed to better understand and explain the findings observed here and their practical implications. This study revealed that many patients described using a behavioral technique that was inconsistent with their actual behaviors. While it is clear that subjects were often acting in a manner different than that reported, it is unclear if these study subjects were conscious of these inconsistencies. Future work could aim to better understand real-life insulin pump behaviors and look for explanations for observed behaviors from study participants by recontacting and interviewing them using sets of detailed scenario-based questions that replicate the most frequently observed behaviors. It would also be interesting to review patient data with the subjects to see if they were aware of their inconsistencies. Similar detailed scenario-based questions that could help to understand reasons for patients’ common self-management behaviors could be posted to diabetes patients online communities, like Glu (https://myglu.org) or PatientsLikeMe (https://www.patientslikeme.com), that are designed to accelerate research and amplify the collective voice of thousands of diabetes patients.
An important limitation of our study was the use of paper-based records for collecting participant’s self-reported data on exercise, alcohol, and carbohydrate intake. It is possible that subjects were not recording all their exercise or alcohol events. There are methods available to improve on the accuracy of the data collected that are currently being employed in a follow-up study currently underway. For instance, to achieve higher accuracy in the reported data on exercise wristband heart rate accelerometers are being provided to subjects that measure the intensity and duration of exercise. In this follow-up study, participants are being asked to use a smartphone app (iDECIDE) to self-report data on perceptions on how alcohol/exercise affect insulin absorption and sources of education, and food and alcohol consumed and exercise performed. The authors expect to take advantage of the ubiquity of smartphones to obtain more precise records on food and alcohol consumed and exercise performed (see Figure 2). Another limitation is the small sample size, although each subject did generate multiple behaviors that could be analyzed.
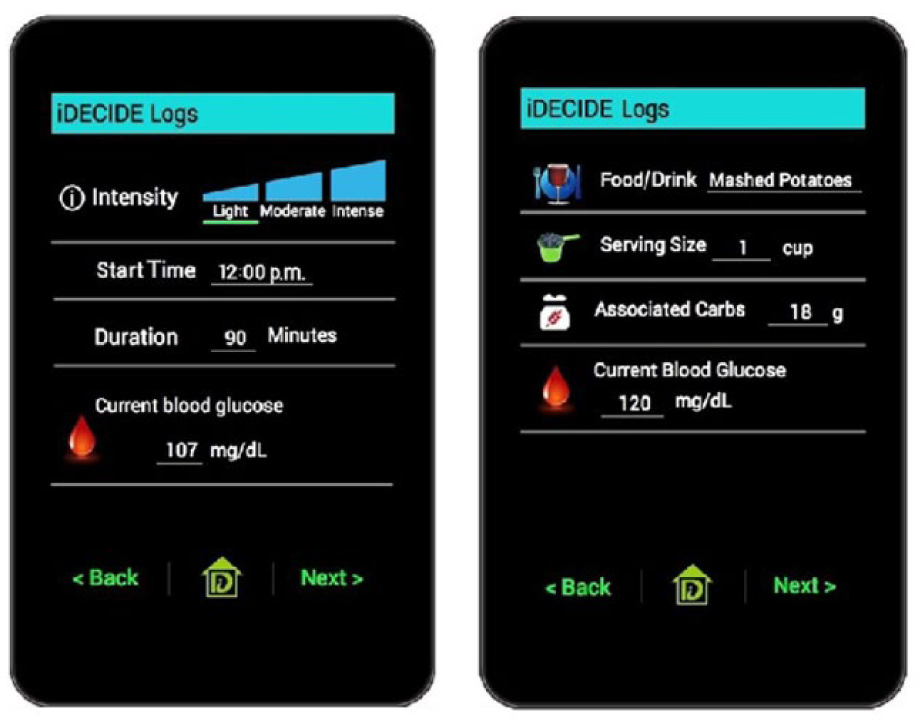
Screenshots of a smartphone app to report (a) plans for exercise and (b) food intake and alcohol.
Conclusion
Despite the limitations, the reported analysis of real-life diabetes self-management decisions provided insight on behaviors occurring in conjunction with alcohol intake and exercise among patients using insulin. The results of this study revealed the need for improved individualized educational techniques and decision support systems to assist patients with incorporating exercise and alcohol into daily life and management of their blood glucose. Further research should focus on understanding reasons behind observed patients’ disease management behaviors and ways to change undesirable behaviors into evidence-based recommended glucose control techniques that could lead to better diabetes self-management.
Footnotes
Abbreviations
ADA, American Diabetes Association; CGM, continuous glucose monitor; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
MAG and DG equally contributed to this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by iDECIDE: Patient-Centered Decision Support Based on Device Data (1U54HL108460), funded by NLM.