
Abstract

Insulin pump therapy (IPT) is an effective method for achieving glycemic control that provides flexibility both in basal infusion rates and the timing and frequency of prandial and correctional bolus dosing. 1 This flexibility allows significant variability among patients in the number of bolus insulin doses administered on a daily basis, which if excessive can increase risk for hyperglycemia or hypoglycemia.2-4 The European Association for the Study of Diabetes and the American Diabetes Association Diabetes Technology Working Group have recently called for an evaluation of human performance with IPT in the clinic setting as a way of identifying and avoiding potential adverse outcomes associated with these devices. 2
The purpose of this investigation was to examine associations between patient practices and glycemic measures in patients using Medtronic® IPT (Fridley, MN, USA) for ≥6 months. This initiative was reviewed by the University Institutional Review Board and approved as a quality improvement project. Two weeks of deidentified IPT data (all insulin doses and blood glucose [BG] measures) from 100 consecutive patients was downloaded at time of scheduled office visits (May 2016-June 2017). IPT data were grouped according to mean bolus frequency of <5 and ≥5 times/day. Statistical analyses for group comparisons were performed using SPSS® (Version 24).
When compared to patients bolusing <5 times/day, those bolusing ≥5 times/day administered more meal and correction doses using the pump calculator (wizard), and performed more overrides of the wizard function (Table 1). This group had better glycemic control by HbA1c and mean BG with less frequent hyperglycemia, and more frequent mild but not moderate or severe hypoglycemia. Among all patients, inverse correlations were observed for bolus frequency with HbA1c (r = –.383, P < .01) and frequency of hyperglycemia (r = –.358, P < .01). No correlations were observed for bolus frequency with glycemic variability or hypoglycemia (P = .17).
Patient Demographics, Glycemic Measures and Pump Practice Patterns.
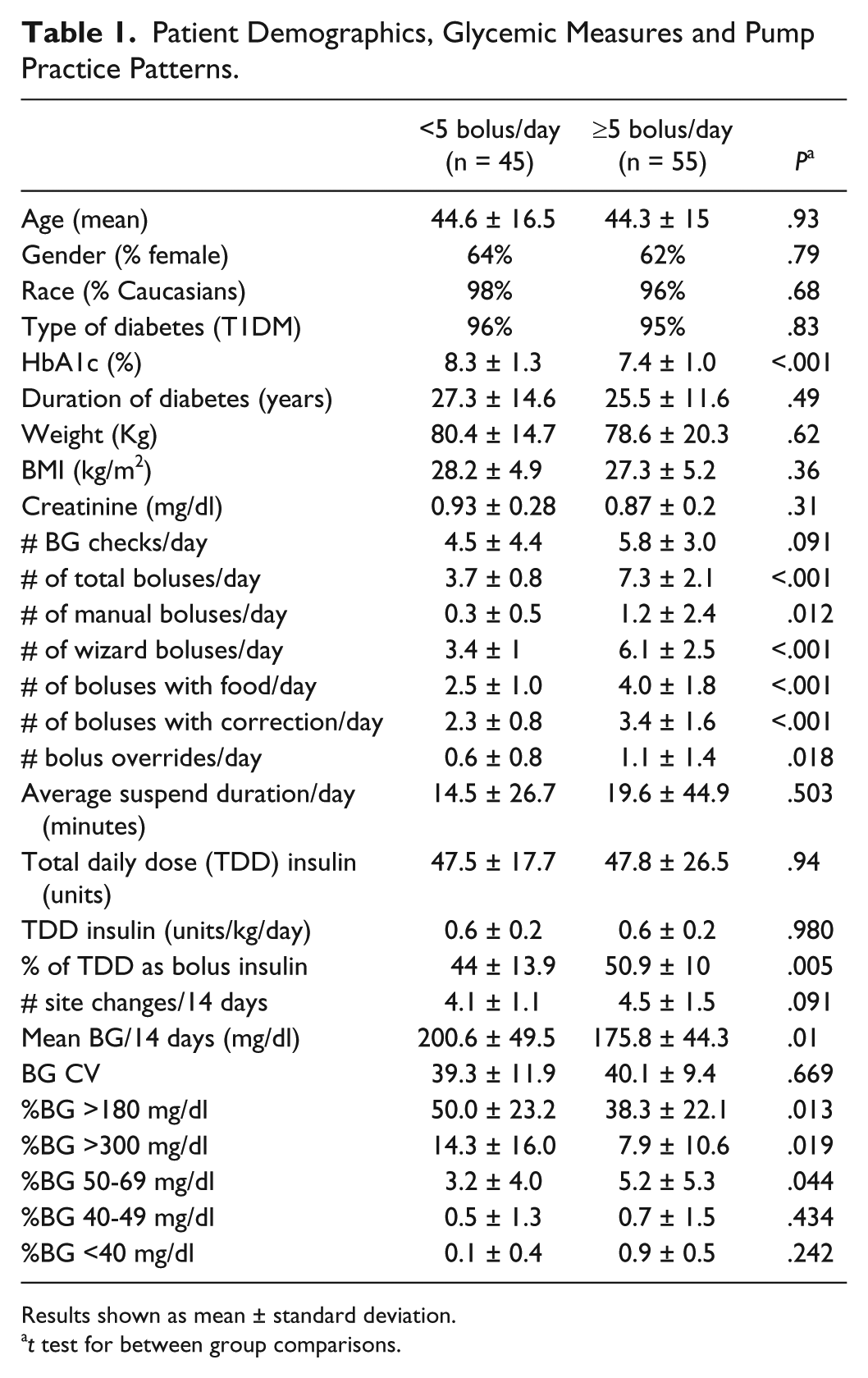
Results shown as mean ± standard deviation.
t test for between group comparisons.
These observations are consistent with prior reports demonstrating that frequent bolus administration is associated with better glycemic control.5,6 The T1D Exchange reported that patients with HbA1c <6.5% were more likely to report administering ≥5 boluses/day when compared to those with HbA1c ≥8.5%. 6 To our knowledge, this is the first report of an increase in mild hypoglycemia events with higher bolus frequency with IPT.
A limitation to the findings in this report is that only two weeks of data were obtained from each patient which may not reflect their practice over longer time periods. Data were obtained only from Medtronic pump devices without continuous glucose monitoring devices (CGM) (except for one patient), which limits the ability to extend these results to other devices with or without CGM.
In summary, these findings reveal that patients administering ≥5 insulin boluses/day have better glycemic control compared to those bolusing less frequently. This improvement in glycemic control occurs with an increased risk for mild but not moderate or severe hypoglycemia. The introduction of sensor-augmented IPT may more reliably guide adjustments of insulin boluses to achieve desired levels of glycemic control with lower risk for hypoglycemia.
Footnotes
Acknowledgements
The authors would like to express their appreciation of the nursing personnel in the UPMC Center for Diabetes and Endocrinology who provided the reports with deidentified downloaded pump data with patient demographics to the authors.
Abbreviations
BG, blood glucose; BMI, body mass index; CV, coefficient of variability; IPT, insulin pump therapy; TDD, total daily dose; T1DM, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.