
Abstract
A tear glucose (TG) sensor with an integrated tear sampler can provide a noninvasive method for calibrating the continuous TG contact lens and monitoring glucose. Expanding from previous work, an improved TG sensor that implements dried reagents, genetically modified glucose dehydrogenase (GDH), and a tear sampler was developed and compared against the TG sensor prepared with commercial GDH. It was found that neither sensor was affected by the tear interferents: ascorbic acid, acetaminophen, and uric acid. The sensor prepared with commercial GDH generated higher current. This suggests that using enzymes with lower Km may be advantageous when operating in low glucose environments like tears. The improved TG sensor also demonstrated the potential of integrating Schirmer’s test strip as a tear sampler for self-monitoring of TG.
Keywords
Tight glycemic control is regarded as the best practice in managing diabetes mellitus (DM) due to its ability to mitigate chronic microvascular complications. 1 Unfortunately, the painful use of needles in current self-monitoring of blood glucose (SMBG) technology discourages people from meeting the quantity of tests required daily2,3 and reduces the resolution of BG trends necessary to accurately predict the changes needed for pharmacological interventions. 3 To achieve sufficient resolution, scientists have shifted their focus to continuous glucose monitoring (CGM) systems and achieved success towards the development of the artificial pancreas.4-6 People without diabetes also wear CGM systems to increase health awareness by monitoring the impact of daily dietary activities. 7 However, depending on one’s lifestyle, cognitive behavior, and preference, the traditional subcutaneous CGM systems are not suitable for every person. 8 Consequently, it is important to have alternative CGM technologies to suit all preferences.
Many successes of CGM contact lens exits9-12 and are expected to become a future technology trend. However, similar to how subcutaneous CGM systems require frequent calibrations, 13 CGM contact lenses will also need a rapid and noninvasive technique of calibration. A reason for frequent calibrations is the use of oxygen as the electron mediator. Many CGM systems today employ glucose oxidase as the sensing element; however, oxygen fluctuation and deficiency can affect the oxidation of glucose, causing errors in glucose measurements. 14 Oxygen fluctuation and deficiency can exacerbate the ocular environment of chronic contact lens wearers who often suffer from various ocular diseases due to significant reduction in oxygen uptake. 15 Although current contact lens have improved gas permeability, the risk of oxygen deficiency and fluctuation still persists due to user misuse and lifestyle choices. Therefore, fabrication of a tear glucose (TG) test strip that does not utilize oxygen as the electron mediator and measures TG in a rapid, noninvasive, and convenient manner offers advantages over the proposed contact lens methods.
Previously, we have reported the development of a TG sensor integrated with a tear sampler and verified its performance with an animal study. 16 TG was found to lag behind BG by approximately 15 minutes with decent correlation. 17 However, improvements and progressions such as testing the sensor against potent interferants in human tears, utilizing dried reagents, and improving the ergonomic and user-friendliness of the tear sampling component should be implemented. In addition, our recent partnership with Tokyo University of Agriculture Technology provided us with genetically engineered glucose dehydrogenase flavin-adenine dinucleotide (GDH-FAD) to incorporate into the sensor. This technical report aims to describe our recent progress in the improvement of the TG sensor through implementing dried reagents and a medical grade filter paper as a tear sampler, comparing the performance between the sensors prepared with engineered GDH-FAD and the commercial GDH-FAD used in the previous work, and investigating the lower limit of detection and robustness against potent tear interferants (ascorbic acid, uric acid, and acetaminophen). The improved TG sensor is a potential calibration means for future continuous TG contact lens. In addition, it can serve as a noninvasive alternative for those who prefer not to use CGMs and SMBG test strips and is a large-scale prototype that can be miniaturized for a smaller sample volume and shorter collection time to improve the comfort and convenience in conventional SMBG.
Methods
Materials
All chemical reagents and materials were acquired from Sigma unless noted otherwise. The 3M adhesive tape was purchased from Grainger. The commercial GDH-FAD was donated by Amano Enzyme Inc. The engineered GDH-FAD was provided by Tokyo University of Agriculture Technology. The GDH-FAD system does not use oxygen as an electron acceptor, 18 making the tear glucose sensor robust against oxygen fluctuations in the ocular environment. The engineered GDH has better thermal stability19,20 and maintains excellent catalytic activity and specificity to glucose.19,21
Sensor Fabrication
To prepare a TG sensor, 30 uL of an enzyme solution containing 1 mg/mL commercial GDH-FAD (activity of 183 U/mg, Km = 15 mM) or engineered GDH-FAD, (activity of 233 U/mg, Km = 35 mM)19,20 was mixed with 10 mM potassium ferricyanide dissolved in 10 mM phosphate buffer saline (PBS). The enzyme solution was then deposited onto the sensing well of a screen-printed sensor (Zensor from CH Instruments) and dried for 1 hour at room temperature in a dehydrator. Afterward, a double-sided 3M tape was attached around the sensing well and an air pathway was constructed at the top of the tape to allow air to exit after sample collection. Sensor fabrication is concluded by attaching a piece of Whatman 41 filter paper. The tape and filter paper was cut by a Universal Laser PLS 4.75 laser cutter with careful control of power to prevent burned edges. The overall schematic is presented in Figure 1.
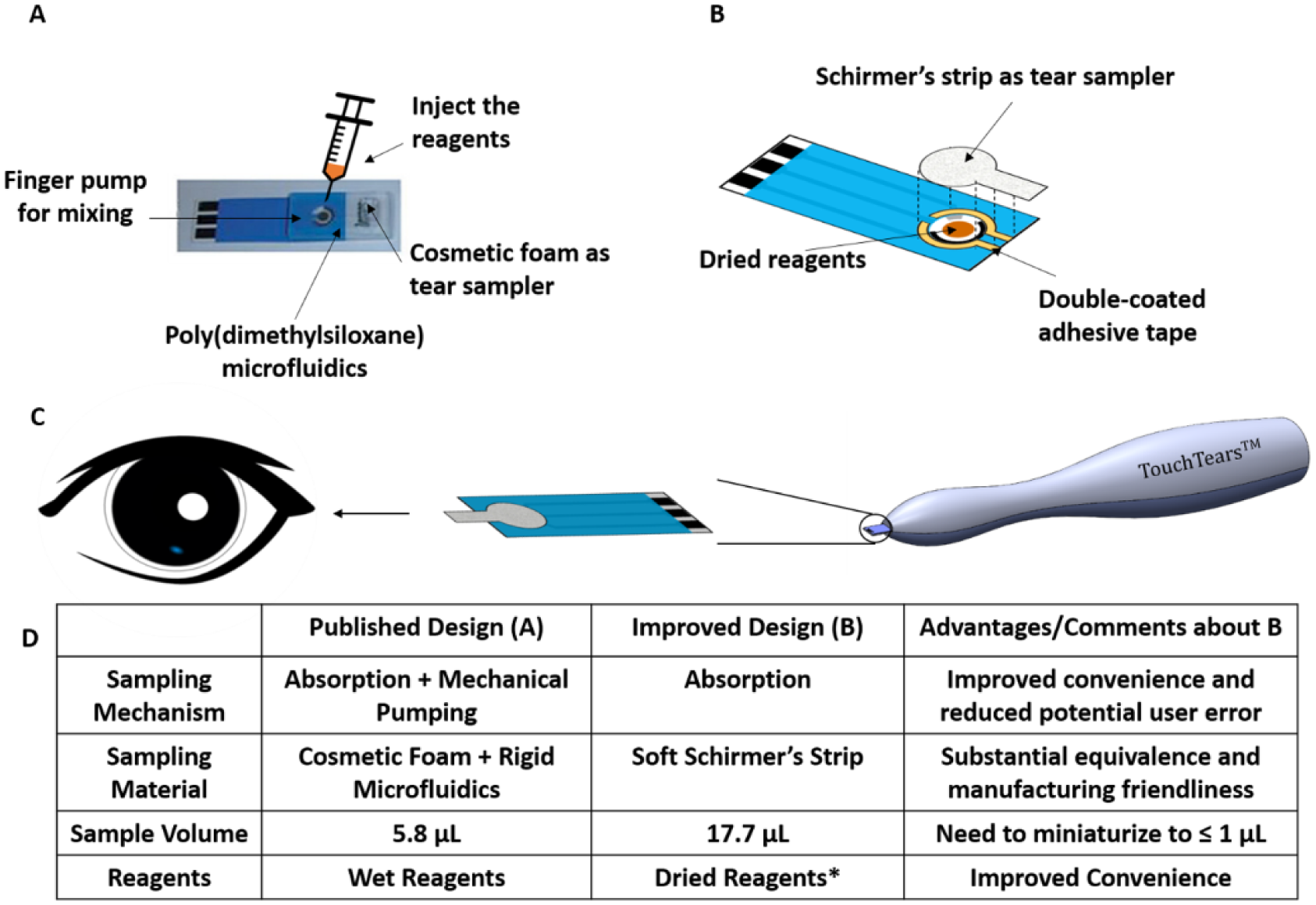
(A) Schematics of an integrated TG sensor published in reference 12. (B) Assembling of the proposed integrated TG sensor after the reagents are dried onto the sensing well, which consists of a carbon working electrode, carbon counter electrode, and silver/silver chloride reference electrode. (C) Design concept of a TG testing system consisting of the improved TG sensor and a hypothetical TG meter. (D) A table comparing the key differences between the two designs. *The manufacturing advantages and disadvantages of engineered GDH-FAD can be found in reference 19-21.
Electrochemical Testing
All electrochemical tests were conducted using the electrochemical station CH1230B from CH Instrument, Texas. First, a cyclic voltammetry (CV) was conducted to characterize the sensor using a scan rate of 100 mV/second from −0.6V to +0.6V. Amperometric measurements were then performed using an applied voltage of 0.35V versus Ag/AgCl for 60 seconds. The integrated TG sensor prototype can collect 17.7 uL of sample with a 6.15% relative standard deviation. To collect sample, the filter paper end of the sensor was dipped into 1 mL of a glucose solution sample for 45 seconds. The glucose concentrations tested for calibration were 0, 5, 10, 15, 20 mg/dL in PBS, covering the physiological ranges in tears.22,23 Another 15 seconds were given to connect the sensor to the CH1230B and all electrochemical tests were performed at t = 60 seconds. For the interference study, 10 uM acetaminophen, 50 uM ascorbic acid and 100 uM uric acid, the most common sources of interference in tears,9,24 were tested at higher values than their physiological levels in tears. 24 The current signals at t = 10 seconds were used as the representing current signal unless otherwise noted. 16 The lower limit of detection (LLD) was calculated by 3.3 * standard deviation / slope of the calibration curve.
Results
Comparison Between Commercial GDH-FAD With Engineered GDH-FAD
The calibration curves of the integrated sensors made with commercial GDH-FAD and engineered GDH-FAD are plotted in Figure 2. The LLDs of the TG sensors prepared by commercial and engineered GDH are 6.4 and 4.0 mg/dL respectively. Both enzymes detected clinically relevant TG levels, 10 but improvements in the reproducibility can improve the LLDs further as the sensors were assembled by hand.
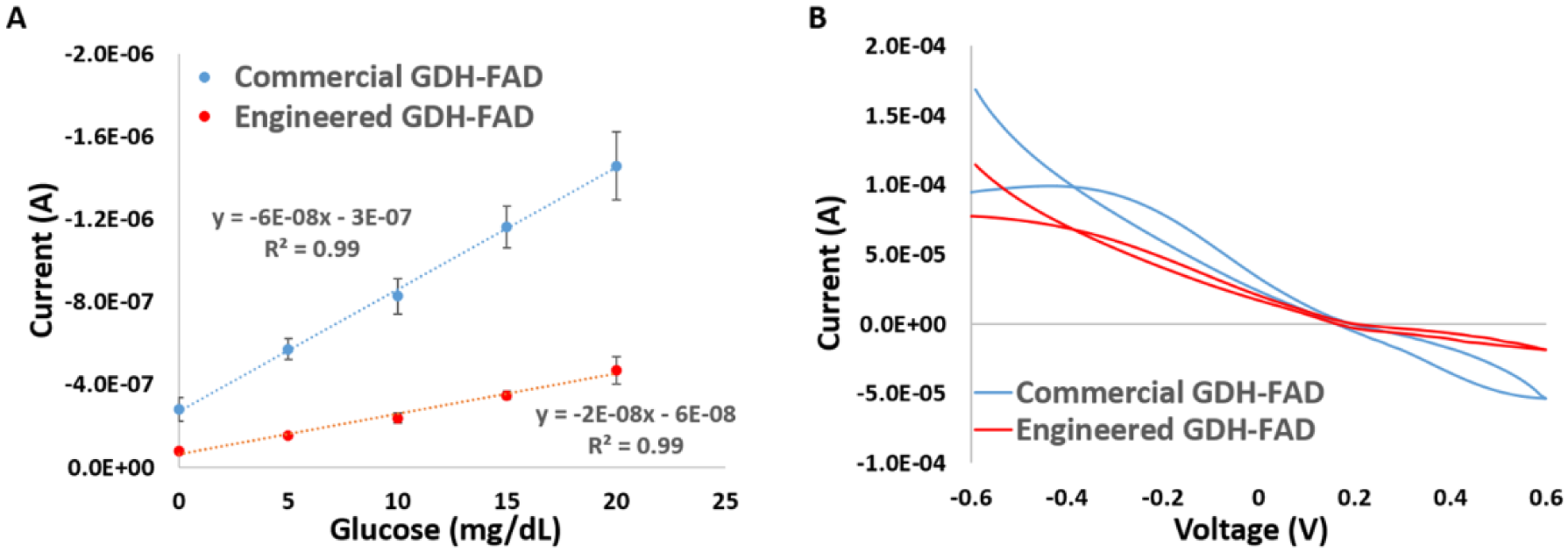
The (A) calibration curves of commercial GDH-FAD and modified GDH-FAD at 0.35V using integrated sensor and (B) CVs of commercial GDH-FAD and engineered GDH-FAD using 10 mg/dL of glucose. The error bars represent 1 standard error. Depending on the concentration, the relative standard deviation (RSD) for commercial GDH-FAD ranges from 9% to 20% and engineered GDH-FAD from 6% to 15%.
Interference Test
Using the commercial and engineered GDH, a comparison study was performed between glucose in PBS and glucose in PBS with 10 uM acetaminophen, 50 uM ascorbic acid, and 10 uM uric acid. Figure 3 shows that neither types of GDH was significantly interfered by the interferents based on the T-test results.
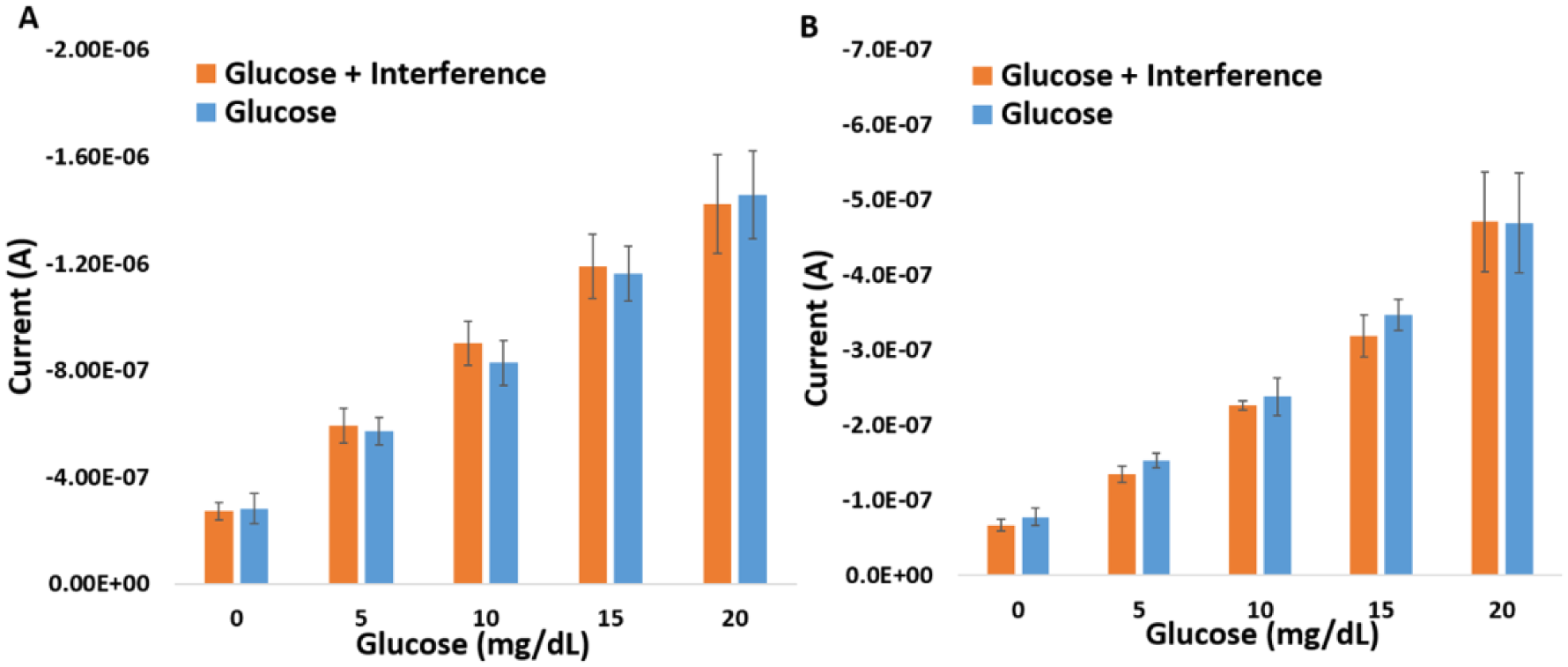
The interference comparison between (A) commercial GDH-FAD and (B) engineered GDH-FAD. The error represents 1 standard error. None of the pairing bars are significantly different based on t-test results (all P values are much greater than .05).
Discussion
Comparison Between Commercial GDH-FAD and Engineered GDH-FAD
As seen in Figure 2, the current generated from the commercial GDH-FAD is larger than in the engineered GDH-FAD. This is perhaps due to a smaller Km value for the commercial GDH-FAD (Km = 15 mM) than the engineered GDH-FAD (Km = 35 mM). The Km value of an enzyme indicates the amount of substrate required to achieve half of the maximum reaction rate. With t = 10 seconds as the representing current signal of the sensor due to the very low glucose concentration in the sample (equivalent to 0–1.1 mM), the commercial GDH with a smaller Km has a higher reaction rate than the engineered GDH, resulting in higher current output. This also suggests that, contrary to common CGM practices, enzymes with a low Km or methods to immobilize enzymes to achieve a low Km may be more advantageous when making a rapid and sensitive TG sensor suitable for self-monitoring of tear glucose (SMTG).
Significance of an Integrated Tear Sampler
Tear collection methods can cause large variance in TG concentration due to reflex tearing and stress-induced responses. 22 A noninvasive TG test with an integrated tear sampler can help reduce the variance and provide a safe, rapid, and comfortable means of tear sampling required for SMTG. According to Posa et al, the use of Schirmer’s strip for tear collecting is preferred greatly over a capillary tube among patients. Comfort and ease during tear collection may be the key to reduce stress-induced responses in patients. The tear sampler in the TG sensor is a Whatman 41 filter paper, a FDA-approved material used in Schirmer’s Test for dry eye detection, therefore, it suggests the feasibility of using a Schirmer’s test strip as an integrated tear sampler and bringing moisture back into the dried reagents. Also with custom-made screen-printed sensors, a miniaturized tear sampler capable of capturing 1 µL of sample can complete the collection in one second, showing its potential for SMTG. Regarding safety, potassium ferricyanide has very low toxicity. A known hazard is mild irritation to the eyes and skin. Future improvement includes the incorporations of safer reagents, such as the third generation GDH-FAD with the capability of direct electron transfer and a nonleaky design. Once miniaturized and optimized, the integrated TG sensor has the potential to provide a calibration technique for CGM contact lens and an alternative for SMBG.
Conclusion
An improved TG sensor with the incorporation of dried reagents and an integrated tear sampler made of Schirmer’s strip was investigated. The comparison between the TG sensors made of commercial and engineered GDH revealed that GDH with lower Km may be advantageous in obtaining stronger signals in low glucose environments such as tears and that neither sensor is affected by potent tear interferants. Also if miniaturized, the proposed TG sensor may be feasible for SMTG, providing a method for calibrating future continuous glucose contact lens and an alternative to SMBG.
Footnotes
Acknowledgements
The authors would like to thank Simran Shrama and Shreya Kodira from PES University, Bangalore for assisting with data collection. Yuka Ito was supported by the Japan Student Services Organization (JASSO).
Abbreviations
Ag/AgCl, silver/silver chloride; BG, blood glucose; CE, counter electrode; CGM, continuous glucose monitoring; CV, cyclic voltammetry; DM, diabetes mellitus; FAD, flavin-adenine dinucleotide; GDH, glucose dehydrogenase; LLD, lower limit of detection; PBS, phosphate buffer saline; RSD, relative standard deviation; SMBG, self-monitoring of blood glucose; SMTG, self-monitoring of tear glucose; TG, tear glucose; WE, working electrode.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Mayo Clinic.