
Abstract
Background:
The artificial pancreas (AP) system, a technology that automatically administers exogenous insulin in people with type 1 diabetes mellitus (T1DM) to regulate their blood glucose concentrations, necessitates the estimation of the amount of active insulin already present in the body to avoid overdosing.
Method:
An adaptive and personalized plasma insulin concentration (PIC) estimator is designed in this work to accurately quantify the insulin present in the bloodstream. The proposed PIC estimation approach incorporates Hovorka’s glucose-insulin model with the unscented Kalman filtering algorithm. Methods for the personalized initialization of the time-varying model parameters to individual patients for improved estimator convergence are developed. Data from 20 three-days-long closed-loop clinical experiments conducted involving subjects with T1DM are used to evaluate the proposed PIC estimation approach.
Results:
The proposed methods are applied to the clinical data containing significant disturbances, such as unannounced meals and exercise, and the results demonstrate the accurate real-time estimation of the PIC with the root mean square error of 7.15 and 9.25 mU/L for the optimization-based fitted parameters and partial least squares regression-based testing parameters, respectively.
Conclusions:
The accurate real-time estimation of PIC will benefit the AP systems by preventing overdelivery of insulin when significant insulin is present in the bloodstream.
Keywords
Type 1 diabetes mellitus (T1DM) is a chronic condition characterized by the autoimmune destruction of pancreatic beta cells, resulting in the inability of the pancreas to produce the insulin necessary for maintaining euglycemia. Without the normal glucose homeostasis mechanism, individuals living with T1DM depend on exogenous insulin administered through either multiple daily injections or continuous subcutaneous insulin infusion (CSII). Insulin infusion pumps and automated control algorithms have enabled automated insulin delivery, the artificial pancreas (AP) technology, where control algorithms calculate the required insulin dose based on continuous glucose monitoring (CGM) measurements and control criteria.1-17 Regardless of the control algorithms, AP systems require a safety constraint to moderate the potential aggressive control actions (insulin overdosing) to minimize the risk of hypoglycemia and significantly improve the performance of the AP.
The primary limiting factor in determining the amount of active insulin present in the body is the lack of sensors capable of nonintrusive and real-time measurement of insulin concentrations in the bloodstream. Estimating the amount of available insulin in the body is challenging because of the inter- and intrapatient variability attributed to physiological differences and metabolic changes throughout the course of the day. Despite the lack of direct measurement, maintaining the blood glucose concentration (BGC) in the target range requires AP systems that are cognizant of the quantity of insulin previously administrated, which if not appropriately incorporated into the control algorithm may cause overcorrection for the postprandial rise in BGC. Such excessive dosing in either the bolus or basal insulin administered through CSII pumps can potentially lead to hypoglycemia. Hence, in addition to the current and target BGC, a constraint expressing an approximation of the insulin present in the body, such as the conventional insulin on board (IOB) estimates, is needed for insulin-dosing calculations.
The IOB is an estimate of the amount of insulin that is present in the blood and the interstitial fluid cavity. It is typically determined through the approximation of the insulin decay curves, which represent the amount of insulin still remaining in the body due to the prior insulin infusions. Static approximations of the insulin action curves are typically utilized in insulin pumps, with IOB calculations primarily relying on basic insulin decay profiles. Furthermore, significant time-varying delays induced by the absorption and utilization of the subcutaneously administrated insulin as well as diurnal variations in the metabolic state of individuals have significant effects on the IOB. Therefore, the insulin action curves for IOB calculations, usually involving static models with basal and bolus insulin as inputs and active insulin as the output, are not accurate enough to be used in an AP control system. Regardless of the sophistication of the IOB calculation, the information obtained from insulin action curves is usually an approximation of the active insulin in the body and is not a direct estimate of the concentration of insulin in the bloodstream. Other approaches to determine the bloodstream insulin information involve estimating plasma insulin concentrations (PICs) and calculating the amount of subcutaneously administered insulin present through insulin absorption models.1,2,8,18-24
Accurate estimates of PIC can be obtained by using CGM measurements with adaptive observers designed for simultaneous state and parameter estimation based on reliable glucose-insulin models. Several methods have been proposed for real-time estimation of PIC.8,25-33 In one study, an extended Kalman filter is used to compute the real-time estimates of PIC from CGM data based on Hovorka’s glucose-insulin model with various time-varying model parameters considered as extended states in the original model.
25
The proposed method is tested using an in-silico study of 100 patients with T1DM and clinical data from 12 patients on CSII therapy to demonstrate the estimation results. An unscented Kalman filter (UKF) is designed to estimate the current PIC based on the measurement of the plasma glucose using a discretized version of Bergman’s minimal model with BGC as an output.
26
Clinical data from an intravenous glucose tolerance test (IVGTT) are used to evaluate the estimation results. The UKF approach is also applied to the extended Bergman’s model to simultaneously estimate parameters and states.
27
An estimator incorporating error feedback is also proposed based on the measured and predicted BGC using Bergman’s third-order nonlinear model designed to tolerate measurement noise as well as discretization errors by means of the
In our previous studies, the design of adaptive and personalized PIC estimators that directly take into account the inter- and intrasubject variabilities in glucose-insulin dynamics is investigated using three different estimation techniques, including continuous-discrete extended Kalman filter (CDEKF), UKF, and moving horizon estimation (MHE).31-33 The results are based on clinical experiments conducted with adolescents at the Yale Children’s Diabetes Clinic (New Haven, CT) involving 13 datasets from subjects with T1DM. Five-hour-long euglycemic clamps were employed on two separate occasions. One clamp was performed with the insulin infusion site warming device (IISWD) and the other without the IISWD. All subjects received insulin Aspart at 0.2 U/kg bolus relative to body weight at the start with or without the IISWD, while the basal infusion of insulin via the insulin pump was suspended. Subsequent to the bolus insulin injection, a variable flow rate of fluid with 20% dextrose was infused and adjusted every five minutes based on bedside measurements of plasma glucose to maintain the BGC within the desired range of 90 to 100 mg/dL throughout the study. Although, the three estimation techniques showed good performance for the clinical data, 33 the MHE had the highest computation time and the CDEKF approach was likely to result in instability or poor performance at certain sampling instances due to the linear approximation of the nonlinear model around the operating point. The UKF provided good PIC estimation and was relatively tractable for on-line real-time applications.
The results from the previous study are limited to the five-hour euglycemic clamp study on adolescent subjects. The above considerations provide a strong motivation for evaluating the proposed UKF-based PIC estimation algorithm in a more realistic setting. Therefore, this study analyzes the performance of the proposed individualized PIC estimation algorithm using 20 clinical datasets from closed-loop experiments conducted continuously over 60 hours involving young adults with T1DM. The diversity of the subjects and the length of the clinical experiments allow for a more comprehensive and critical evaluation of the performance of the PIC estimation method that will be incorporated into the AP system. The significant variability in data for various subjects is due to the different meals (amount and type of carbohydrate intake), varied daily basal rates, varied bolus insulin infusions, physical activity levels, and sleep characteristics. The discrete sampling nature of the CGM measurement output, the lack of knowledge on the exact time and amount of meals, the time-varying nature of human physiology, the unmeasured disturbances caused by exercise and sleep, the intersubject variability, the constraints on the state variables, and the rate of change of the model parameters are some of challenges addressed in this work. The PIC estimator is individualized using readily available demographic information, such as body weight, height, body mass index (BMI), and total daily insulin dose. The PIC estimation results are compared against those obtained through the conventional IOB curves to demonstrate the merits of the proposed individualized PIC estimator.
Methods
Subjects and Clinical Study Experiments
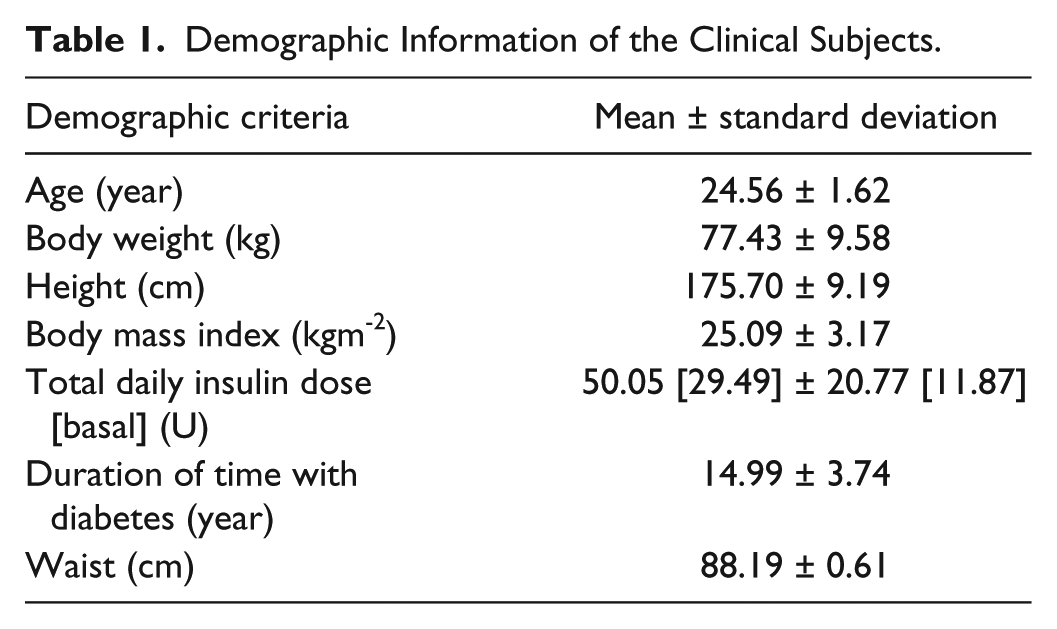
The subjects involved in this study were recruited by the Kovler Diabetes Center, University of Chicago Medical Center (Chicago, IL) and were scheduled for a visit at the University of Chicago General Clinical Research Center. The subjects included healthy, physically active young adults between the ages of 18-35 years with T1D. All subjects used CSII pump therapy. Each patient’s visit was approximately 60 hours long during the closed-loop experiment. The subjects’ own insulin type and pumps were used during the experiments. Subjects were provided a total of 13 meals and snacks during the three days of the closed-loop experiment. Each subject participated in exercise bouts of 20-min sessions for aerobic and resistance (days 1 and 3) or interval (day 2) exercise before and after lunch, respectively. An intravenous catheter was placed in the dominant arm for blood sampling every 30 mins, which was later analyzed to quantify the PIC in the blood samples. These PIC values are used to evaluate the accuracy of the proposed PIC estimation algorithm. Overall there are 20 clinical closed-loop experiments. Table 1 shows the characteristics of the participants of the closed-loop studies.
Demographic Information of the Clinical Subjects.
Glucose-Insulin Dynamic Model
Several models are proposed in literature to provide a mathematical representation of the glucose-insulin system. Hovorka’s model,
34
a widely utilized physiological model for describing the insulin action and the glucose kinetics system, is used in this study for designing the UKF estimator. A brief description of Hovorka’s model is provided for completeness. The model consists of nine state variables and various differential equations that describe the glucose-insulin dynamics, the subsystem pertaining to the BGC dynamics, the subsystem concerning the subcutaneous insulin infusion, and the subsystem for the glucose transport from plasma to interstitial tissues. The BGC dynamics are described using a two-compartment model. The two state variables
PIC Estimator Individualization
The time-varying model parameters
To address the issue of the appropriate personalized initialization of the parameters
Partial Least Squares Models
The demographic information of subjects, such as weight, height, BMI, age, total daily insulin and duration with T1DM, is easily attainable. Hence, this demographic information can be exploited to personalize the initialization of the PIC estimator. To this end, the readily available demographic information is used to identify a relationship between the demographic variables and the model parameters to be individually initialized to each patient. Data-driven approaches, such as PLS regression models, are widely used when the exact underlying mathematical relationship between two sets of data, demographic inputs (matrix
Results
Individualized Parameter Estimation Results
The results for the individualization of the PIC estimators by predicting the initial values for the time-varying parameters using PLS regression models are first presented. In Table 2, the demographic information used as the independent variables and the average of relative error percentage (AREP) for each time-varying model parameter based on leave-one-out cross-validation (LOOCV) are presented.
Input Variables and Accuracy of the PLS Models for Individualization of PIC Estimators.
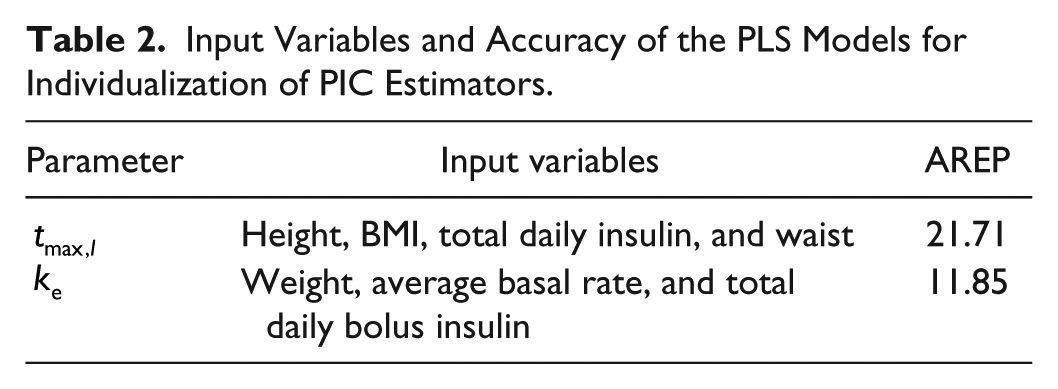
The AREP for the
The use of the demographic information for training the PLS models to provide initial values of the PIC estimators gives good predictions for the initialization of the time-varying model parameters. Table C1 in Appendix C presents the coefficient matrices of the regression model for predicting the
Plasma Insulin Concentration Estimation Results
The PIC values are estimated using the UKF algorithm with the initialization of the model parameters either through the optimization-based fitting parameters or the PLS-regression-based testing parameters. The root mean square error (RMSE) and mean absolute error (MAE) of estimating the PIC values based on different sets of individualized initial parameters are computed. The average values for the RMSE and MAE in PIC estimation using Hovorka’s model without any feedback correction through the CGM measurements for various parameter estimation approaches are presented in Table 3.
RMSE and MAE Values for Estimating the PIC Using Hovorka’s Model With Various Estimates of the Parameters and Without Feedback Correction.
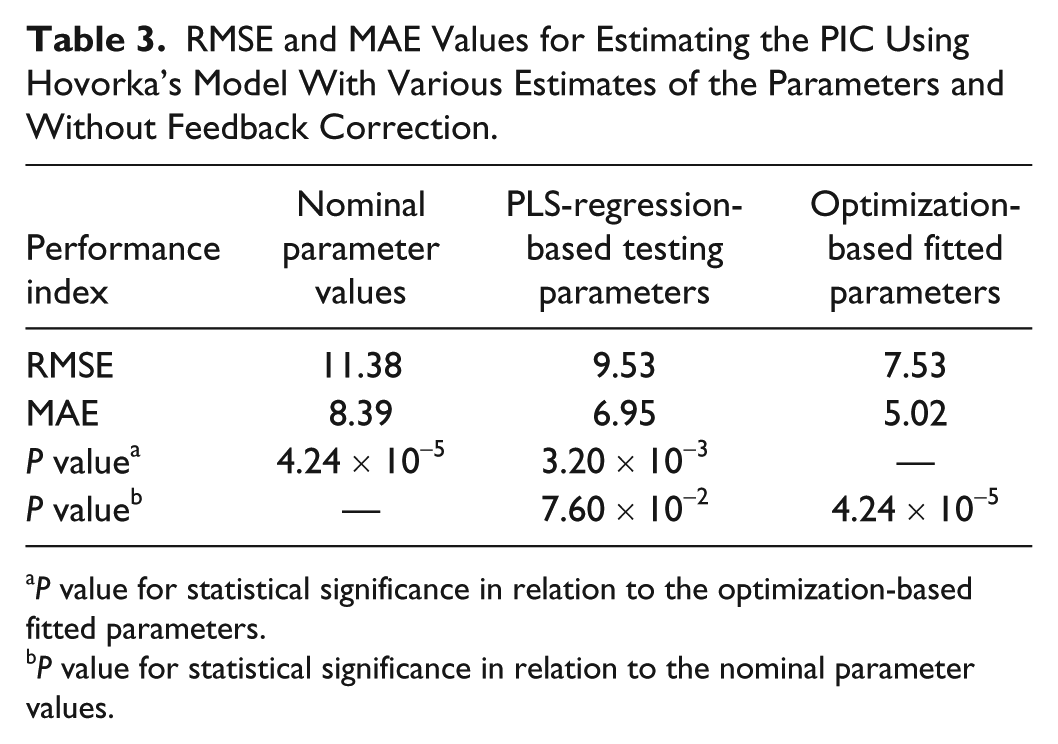
P value for statistical significance in relation to the optimization-based fitted parameters.
P value for statistical significance in relation to the nominal parameter values.
The RMSE and MAE values for PIC estimation without individualization of the time-varying model parameters are greater than the approaches involving personalized parameters. This demonstrates that the nominal model parameters are not sufficient and that the individualization of the parameters for each patient is important in reducing the estimation error. The PLS-regression-based parameters do not significantly improve the PIC estimates (P value =
The results based on UKF for feedback correction through the available CGM measurements are also evaluated and presented in Table 4. The UKF-based approach is also personalized through various sets of model parameters that are determined by different initialization methods of the time-varying parameters. Once again, accurate results are obtained for PIC estimation through the optimization-based fitting parameters, while the initialization of the time-varying parameters through the use of the PLS regression models provides better results than the initialization using the nominal model parameters (P value =
RMSE and MAE Values for Estimating the PIC Using Hovorka’s Model With Various Estimates of the Parameters and With UKF-Based Feedback Correction.
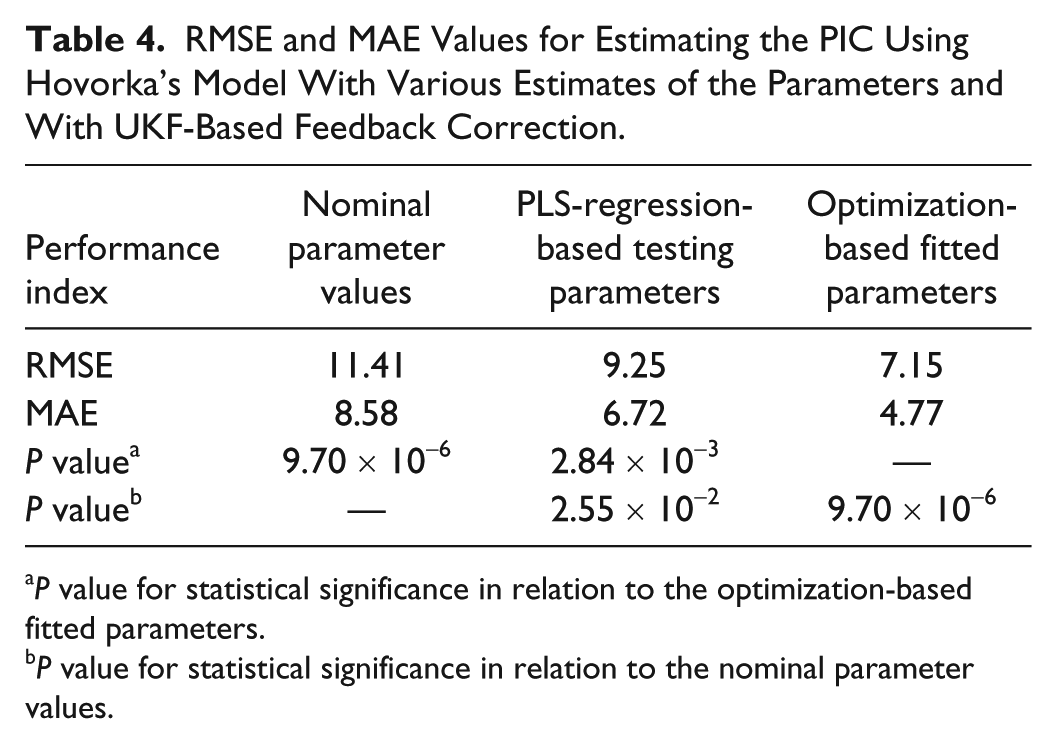
P value for statistical significance in relation to the optimization-based fitted parameters.
P value for statistical significance in relation to the nominal parameter values.
Figure 1 shows the results for the optimization-based fitting parameters and PLS-regression-model-based testing parameters for one clinical experiment. The proposed estimation algorithm is able to accurately quantify the PIC values and closely track the corresponding CGM measurements. Overall, by comparing the presented results in Tables 3 and 4, the requirement for developing an adaptive and individualized PIC estimator is demonstrated.
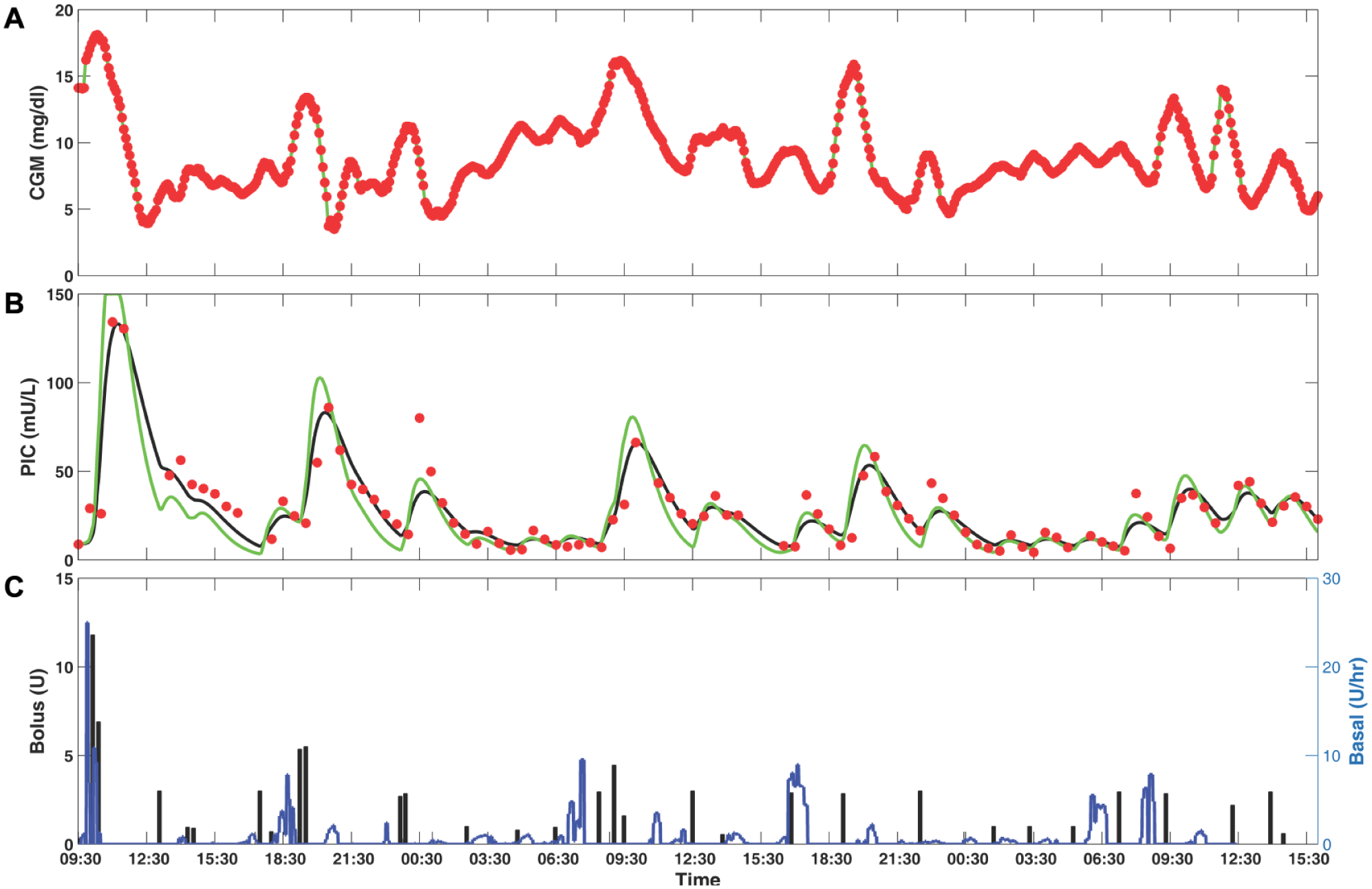
(A) Comparison of estimated and measured CGM data based on UKF. Black line: estimated CGM based on fitting parameters; green line: estimated CGM based on testing parameters obtained by PLS model; filled red circle: measured CGM. (B) Comparison of estimated and measured PIC data based on UKF. Black line: estimated PIC based on fitting parameters; green line: estimated PIC based on testing parameters obtained by PLS model; filled red circle: measured PIC. (C) Basal (blue line) and bolus insulin (black bar).
Figure 2 shows the time-varying parameters,
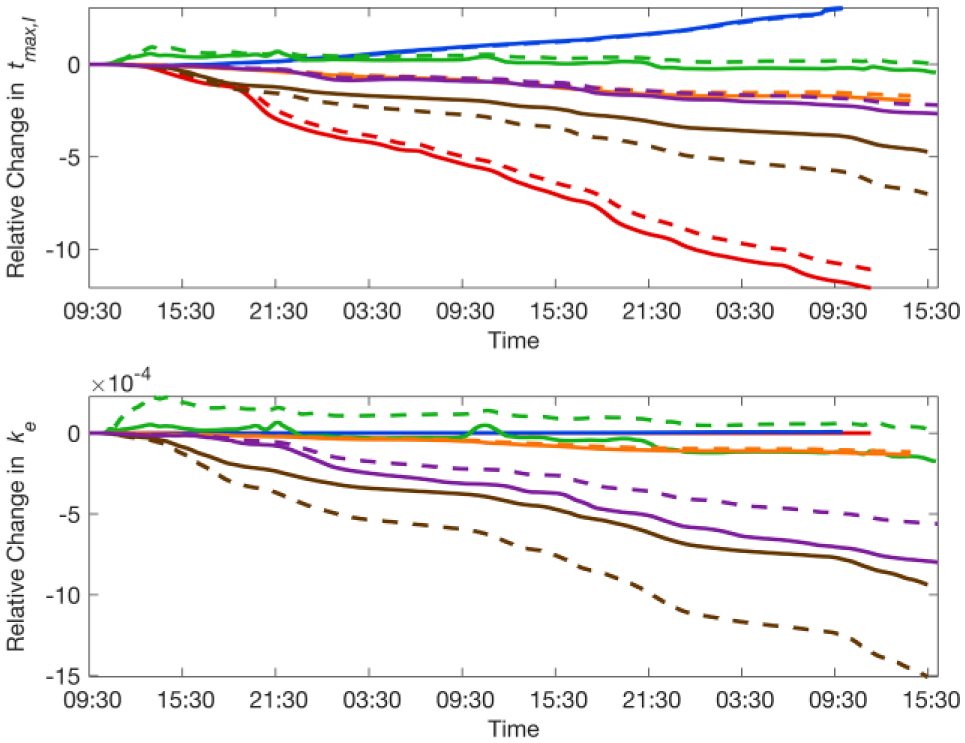
Time-varying trajectory profiles for the
Discussion
A major drawback of using standard IOB curves is the inability to accurately characterize the temporal dynamics of active insulin in the body. Figure 3 shows the estimated onboard insulin based on various IOB curves 18 along with the PIC estimates from the proposed approach for one clinical experiment. Since the units of the values computed by the IOB curves and the PIC estimates are not consistent, both the IOB and PIC estimates results are scaled. The IOB trajectories do not correspond well with the PIC estimates, as exemplified by the fact that the maximum PIC estimates do not coincide with the largest values predicted by IOB curves. This inherent limitation is due to the static IOB curves that do not characterize the temporal dynamics of the absorption of subcutaneously injected insulin.
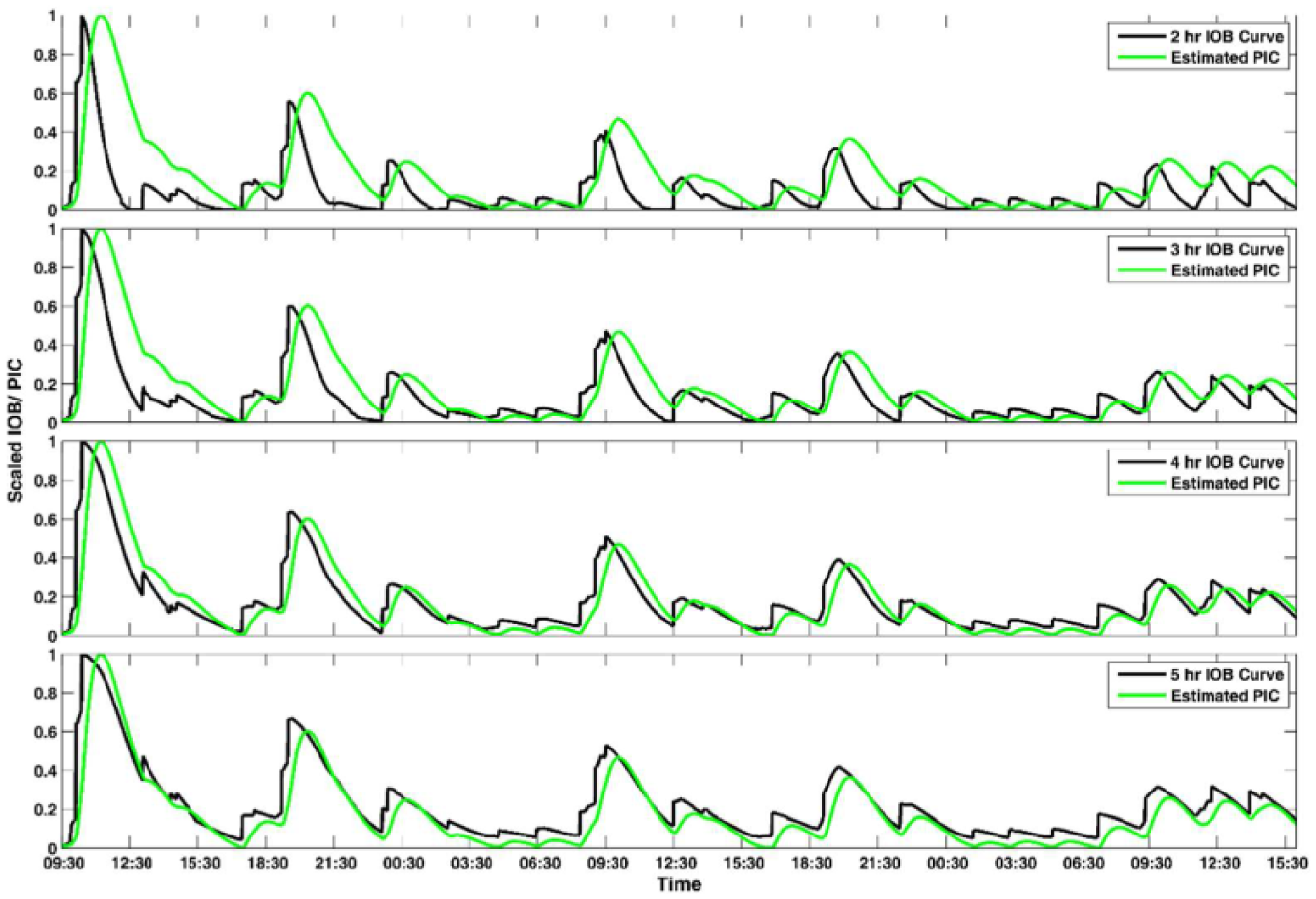
Comparison of scaled estimated PIC and different IOB curves results for one experiment.
As evident in the clinical results, individuation of the PIC estimators is important for the accurate estimation of the PIC. If the initial values for the time-varying model parameters are not specified appropriately, the performance of the PIC estimators may be compromised. Furthermore, temporal variability within the subjects is accounted for by the on-line estimation of the
Nevertheless, the variations in the insulin-glucose dynamics because of the differences in daily activities or the metabolic state of the individuals may also affect other parameters of the model. The proposed PIC estimation approach can also take into account the effects of these other factors by incorporating additional model parameters as extended states to the original model. In this work, a technique to personalize two model parameters in the glucose-insulin dynamic model is presented. Individualizing other model parameters could also affect the accuracy of the model, potentially resulting in better tracking of the CGM data, and consequently yielding better estimates of the PIC values and the time-varying parameters.
In studies investigating the AP system, various types of controllers are applied to regulate BGC, including the proportional-integral-derivative (PID) control and the model predictive control (MPC) algorithm. In all AP control systems, insulin infusion should be limited for safety considerations through the use of information on the available infused insulin present in the body that will gradually affect the BGC. One of the advantages of the MPC control algorithm is the convenience of incorporating additional constraints into the optimization problem formulation.
Another important consideration for AP systems is the on-line computational tractability of the control and estimation algorithms. Although more sophisticated estimation algorithms can be employed to estimate the PIC values, the approaches generally require greater computational effort. On the other hand, decreasing the computational complexity may adversely affect the prediction accuracy as these are typically competing criteria and the tradeoffs between them should be effectively balanced. For on-line real-time applications, it is necessary to consider the accuracy of the estimated PIC values along with the associated computational burden, especially when implementing the algorithms on computationally constrained wearable or implantable hardware.
Conclusions
Accurate information on the amount of active insulin present in the body is necessary for AP systems to avoid overdelivery of insulin. In comparison to conventional IOB curves, the PIC provides a better representation of the active insulin present in the body. Although the PIC cannot be measured in real time, it can be readily estimated through algorithms based on glucose-insulin dynamic models. The proposed method utilizes CGM and infused insulin data to compute the PIC estimates with time-varying model parameters incorporated as augmented states to capture the temporal dynamics in patients. The proposed method would benefit AP systems by providing PIC estimates in real time.
Footnotes
Appendix A
Appendix B
Appendix C
Appendix D
Acknowledgements
The authors are grateful to Paul Rue for conducting skillfully the plasma insulin analysis work.
Abbreviations
AP, artificial pancreas; AREP, average of relative error percentage; BGC, blood glucose concentration; BMI, body mass index; CDEKF, continuous-discrete extended Kalman filter; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; IISWD, insulin infusion site warming device; IOB, insulin on board; IVGTT, intravenous glucose tolerance test; LOOCV, leave-one-out cross-validation; LPOCV, leave-p-out cross-validation; MHE, moving horizon estimation; MPC, model predictive control; PIC, plasma insulin concentration; PID, proportional-integral-derivative; PLS, partial least squares; T1DM, type 1 diabetes mellitus; UKF, unscented Kalman filter; UT, unscented transformation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support by NIH with Grants NIDDK DP3 DK101075-01 and DP3 DK101077-01 is gratefully acknowledged.