
Abstract
Recently, two clinical trials about a “sensor-based flash glucose monitoring system” and its efficacy in reducing time in hypoglycemia were published. Interestingly, patients spent more time at low glucose concentrations in these studies than in other studies related to the efficacy of real-time continuous glucose monitoring (rtCGM). Although it is possible that the study populations differed from those in other studies, another potential explanation is that the CGM system used in these two studies had a negative glucose measurement bias. Such a negative bias was reported in recent literature, suggesting that the CGM system may inaccurately indicate hypoglycemia. Reporting blood glucose monitoring data would help to interpret the CGM data at least in the context of time spent in various glucose ranges as a parameter with which quality of diabetes therapy is measured.
Data from two clinical trials with a “sensor-based flash glucose monitoring system” and its efficacy in reducing time in hypoglycemia (TiH) were published.1,2 In the trial with patients with type 1 diabetes conducted by Bolinder et al. 1 TiH was the trial’s primary endpoint. Blood glucose monitoring (BGM) data were not reported in these publications; however, as outlined subsequently these would be of help to interpret the study results.
A literature search for trials regarding the effect of real-time continuous glucose monitoring (rtCGM) or intermittent-scanning CGM (isCGM) on diabetes therapy outcomes that were published within the last 5 years yielded 50 results. A timeframe of the last 5 years was chosen to reflect the increasing analytical accuracy of newer rtCGM system generations that became commercially available, because accuracy may affect time spent in hypoglycemia as measured by the rtCGM system. Of these 50 publications, 12 were excluded because the number of participants was comparably small, and another 29 publications were excluded because they did not provide data for HbA1c or time spent <70 mg/dL (3.9 mmol/L) or both. The remaining 9 publications were analyzed for TiH, defined as time spent <70 mg/dL (3.9 mmol/L) (see Figure 1).1-9 Figure 1 shows only baseline data from these studies: intervention group results are affected by the intervention, and even control group results might be influenced by a potential study effect. Weighted mean values were calculated for TiH and HbA1c based on the individual results presented in the publications and the number of patients in the intervention and control groups.
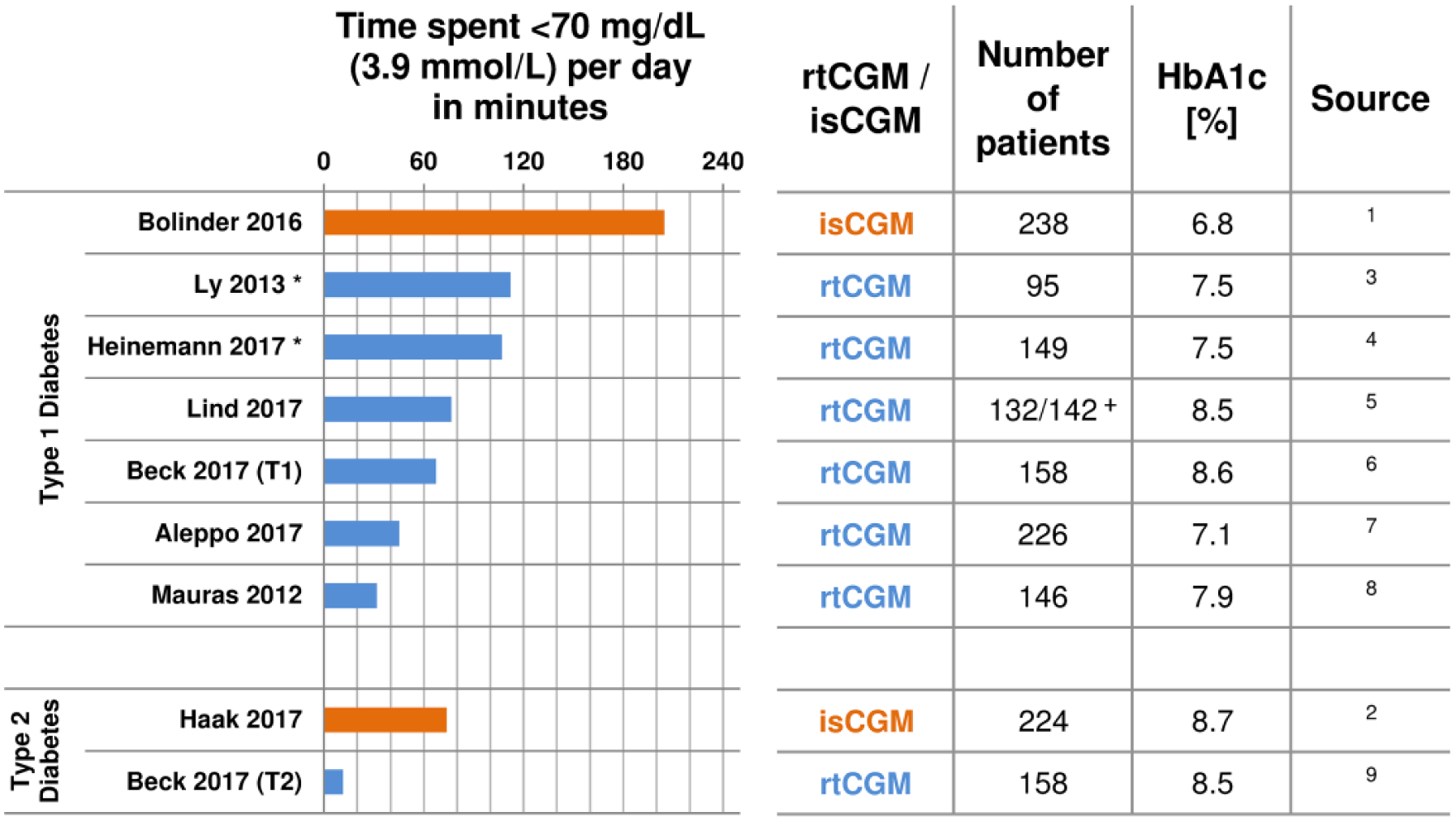
Time spent <70 mg/dL (3.9 mmol/L) measured by rtCGM (blue) or isCGM (orange) glucose levels in various studies. Measurements were performed in patients with type 1 or type 2 diabetes and different baseline HbA1c values.
We would like to focus on two specific studies with rtCGM systems, published by Aleppo et al 7 and by Beck et al. 9 The second study was the only suitable study with patients with type 2 diabetes. The first study was published recently and had a large number of participants whose HbA1c was comparable to that of the participants studied by Bolinder et al. 1
Patients in both studies seemed to spend considerably less TiH than in the isCGM studies: For the “well-controlled” adults (average HbA1c 6.8% [51 mmol/mol]) with type 1 diabetes studied by Bolinder et al, 1 TiH was approximately 205 min per day at baseline. This is well above the approximately 45 min for adults with comparable HbA1c values (7.1% [53 mmol/mol]) studied by Aleppo et al. 7 For the adults with type 2 diabetes (HbA1c 8.7% [72 mmol/mol]) who participated in the study by Haak et al, 2 TiH was 74 min, whereas Beck et al 9 reported 12 min for adults with type 2 diabetes, who had similar HbA1c (8.5% [69 mmol/mol]).
Clearly it is possible that the populations in the two studies with the isCGM system differ from those in the other studies, because inclusion and exclusion criteria were not identical in these studies. For example, Aleppo et al 7 did exclude subjects who experienced severe hypoglycemia, whereas Bolinder et al 1 did not. Haak et al 2 included people using continuous subcutaneous insulin infusion, whereas Beck et al 9 did not.
However, another potential explanation is that the isCGM system had a negative systematic measurement difference (bias) with respect to BGM. If such a bias existed, it would (artificially) increase TiH at baseline. Such a bias could also be a possible explanation why in the study by Haak et al 2 HbA1c decreased slightly less (difference not statistically significant) in the intervention group using nonblinded isCGM than in the control group using regular therapy or blinded isCGM.
A negative bias was reported in a recent publication for the isCGM system when BGM were ≤150 mg/dL (≤8.3 mmol/L). 10 Food and Drug Administration (FDA) premarket approval data for this isCGM system also indicate a negative bias. 11 For the professional-use version of this isCGM system, the FDA explicitly noted in its premarket approval that this system may inaccurately indicate hypoglycemia, because in 40% of cases in which sensor glucose readings were <60 mg/dL (<3.3 mmol/L), BGM were in the range of 81 to 160 mg/dL (4.5 to 8.9 mmol/L). 12
Therefore, we suggest that neither rtCGM nor isCGM data are reported without accompanying BGM data; at least in the context of time spent in various glucose ranges as a parameter with which quality of diabetes therapy is measured. Reporting BGM data would help to interpret rtCGM/isCGM data. If a considerable systematic measurement difference (bias) between CGM and BGM data were found, acknowledging this bias in publications would also be helpful. Quantitative analysis of bias, if one exists, could possibly provide additional information. It should not be forgotten that laboratory analyzers and even most of the hand-held BGM systems for self-use still provide more accurate glucose measurement results than the current generation of rtCGM/isCGM systems.
Recommendation
If rtCGM or isCGM data are reported in the context of a CGM system’s impact on time spent in various glucose ranges, BGM data should also be provided.
Footnotes
Abbreviations
BGM, blood glucose monitoring; CGM, continuous glucose monitoring; FDA, Food and Drug Administration; isCGM, intermittent-scanning continuous glucose monitoring; rtCGM, real-time continuous glucose monitoring; TiH, time in hypoglycemia.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SP is employee of the IDT (Institut für Diabetes-Technologie Forschungs- und Entwicklungsgesellschaft mbH an der Universität Ulm, Ulm, Germany). LH is member of advisory boards/consultant for a number of companies that are developing diagnostic and therapeutic options. He is shareholder of the Profil Institut für Stoffwechselforschung, Neuss, Germany, and ProSciento, San Diego, CA, USA. GF is general manager of IDT, which carries out clinical studies on the evaluation of BG meters and medical devices for diabetes therapy on its own initiative and on behalf of various companies. GF/IDT have received speakers’ honoraria or consulting fees from Abbott, Ascensia, Bayer, Berlin-Chemie, Becton-Dickinson, Dexcom, LifeScan, Menarini Diagnostics, Novo Nordisk, Roche, Sanofi, Sensile, and Ypsomed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.