
Abstract
Studies have found variability in self-care behaviors in patients with type 1 diabetes, particularly when incorporating exercise and alcohol consumption. The objective of this study was to provide results from a survey to understand (1) insulin pump behaviors, (2) reported self-management behaviors for exercise and alcohol, and (3) perceptions of the effects of exercise and alcohol on blood glucose (BG) control. Fourteen participants from an outpatient endocrinology practice were recruited and administered an electronic survey. Compensation techniques for exercise and alcohol, along with reasons for employing the techniques were identified. Also identified were factors that participants said affected BG control with regard to exercise and alcohol. These results confirm the considerable inconsistency patients have about incorporating exercise and alcohol into decisions about self-management behaviors.
Maintaining euglycemia for patients with type 1 diabetes (T1D) requires ongoing self-management, education, and support. 1 Several studies have found that there is variability in self-care behaviors, particularly when incorporating lifestyle preferences such as exercise and alcohol consumption.2-7 A recent study by the authors on patients with T1D using insulin pumps found little consistency on how patients accounted for carbohydrate, alcohol and exercise behaviors when making decisions on insulin bolusing. The study analyzed over 4200 insulin pump interactions for carbohydrates, 155 alcohol, and 347 exercise events from free-living patients.8,9
There have been few studies that have used qualitative data gathered from interviews, surveys and questionnaires to characterize self-care behaviors in patients with diabetes.3,10,11 In addition, little work has been done to understand how patients with T1D using insulin pumps perceive the effects of exercise and alcohol on blood glucose (BG) control, nor have their approaches to compensate for these behaviors been evaluated.
The objective of this report is to provide results of a survey of a similar cohort of adults with T1D to understand (1) insulin pump behaviors, (2) reported self-management behaviors for exercise and alcohol, and (3) perceptions on the effect of exercise and alcohol on BG control.
Methods
Fourteen participants were recruited from an outpatient endocrinology practice. Participants were part of a study which did not require a large sample size. 12 Chart reviews were used to identify adults with T1D on insulin pump therapy paired with a continuous glucose monitoring system. Participants were approached about the study during routine quarterly outpatient visits and were later contacted to set up a recruiting appointment. During the recruiting appointment, an electronic survey was administered onsite to participants. The survey consisted of 11 structured questions and 14 semistructured questions with a free text response option of “other.” Survey questions were developed based on previously identified themes.8,9 Participants were presented all survey questions, even if they indicated that they did not exercise or consume alcohol.
Qualitative data analysis was used to obtain frequencies of responses and analyze associations. All data reported are mean and range.
Results
The mean age of the participants was 48 (25-69) years and the mean hemoglobin A1c was 7.7% (5.3-9.3). The average length of T1D diagnosis was 29 (10-54) years, with 13 (1-22) years of insulin pump therapy. Ten participants were female, and all were Caucasian except for one Hispanic participant.
All participants had a Medtronic (Minneapolis, MN) insulin pump and a smartphone. There were 6 participants that reported using smartphone applications to assist with various health-related tasks, such as tracking body weight, meals, and nutrition, or to assist with estimating nutrition content of meals. With regard to general pump usage, 9 participants reported that they changed the settings on the insulin pump without consulting a clinician and the same number reported overriding bolus suggestions from the insulin pump.
When considering meal time insulin bolus behaviors, six participants changed the waveform of the insulin bolus to compensate for high-fat meals and multicourse meals. Ten participants indicated that they would override the insulin bolus recommendation from the pump to compensate for factors that the pump does not account for, such as reducing the bolus for exercise or increasing the bolus for hyperglycemia. Twelve participants reported that they administer boluses to correct for glycemic excursions without considering carbohydrate intake. Reasons for not accounting for carbohydrates included memory lapse, hypoglycemia, alcohol consumption, physical activity, stress, and illness. Six participants reported not compensating for glycemic excursions when consuming a meal. The primary reason for not including a mealtime BG value was inability to check BG due to dining circumstances.
Of the 14 participants, 2 reported that they drank regularly, 8 drank occasionally, while the remaining 4 reported that they did not drink. In terms of diabetes self-management in conjunction with alcohol consumption, 9 reported checking BG before and/or after consuming alcohol, while 5 indicated not checking BG when drinking.
Participants were asked about techniques used for compensating for alcohol. Half reported that they deliver an insulin bolus and/or take a snack with 4 participants indicating both. Only three participants reported that they adjusted basal rates and none removed their insulin pump. When determining an insulin bolus to account for the effects of alcohol, half of the participants reported calculating carbohydrates based on the drink type. A variety of methods were used to estimate the carbohydrate content: six estimated based on drink type, three used an online database, and one reported using the drink’s nutrition label.
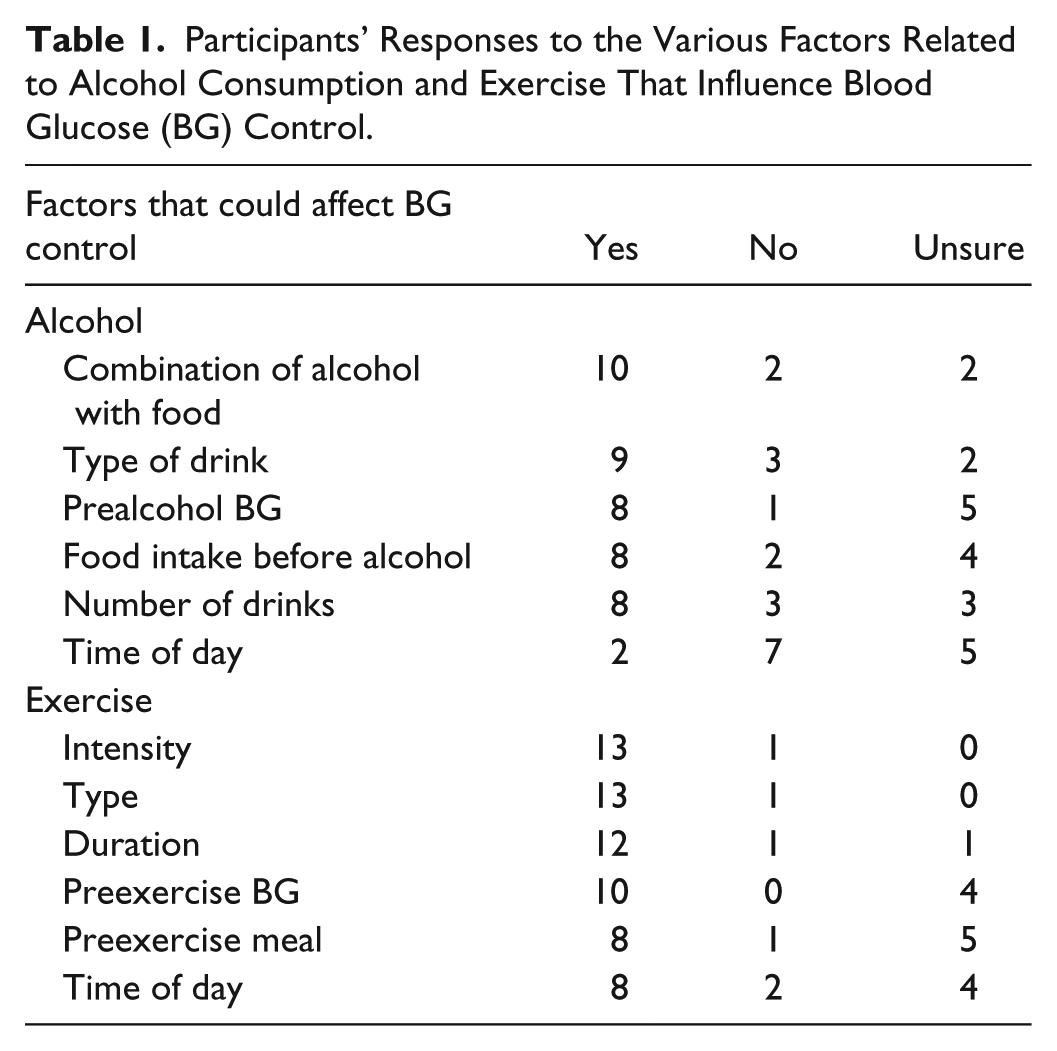
Participants were provided a list of factors that could influence BG when consuming alcohol (time of day, meal before alcohol, combination of food with alcohol, type of drink, number of drinks, BG levels). Ten participants reported that one or more of these factors influenced BG. Ten participants reported that it was the combination of alcohol with food that had an impact, while nine reported effects from the type of drink itself. Half indicated that the time of alcohol consumption had no effect on BG levels. Eight participants reported a lack of knowledge regarding the effects of alcohol on BG (Table 1).
Participants’ Responses to the Various Factors Related to Alcohol Consumption and Exercise That Influence Blood Glucose (BG) Control.
All but one of the participants reported engaging in some form of exercise. Thirteen of the participants reported checking BG before, during, and/or after exercise and one participant reported not checking BG when exercising. Participants were asked about techniques used to compensate for exercise. Thirteen reported they ate a snack, with eight reporting basal adjustments. Five reported removing the insulin pump and four administered an insulin bolus. Four participants reported that BG levels did not affect their decision to exercise, while eight preferred to exercise when they were at target, and six preferred above target, and half reported avoiding exercise if BG was below target.
As with the question on alcohol behavior, participants were also provided a list of factors that could have an effect when exercising (intensity, type, duration, time of day, preexercise BG, and preexercise meal). All 13 of those who engaged in exercise reported that the intensity and type of exercise influences BG and 12 reported effects from duration. All participants reported one or more factors and half reported that they did not have enough knowledge on the effects of some of the provided factors (Table 1).
There were some associations between responses from participants. For example, there were 7 participants that not only reported changing insulin pump settings (n = 9), but also reported overriding bolus suggestions from the insulin pump (n = 9). All 6 of those that reported using smartphone applications also changed insulin pump settings. There were 8 that indicated they adjusted basal rates to compensate for exercise and 7 of those also changed insulin pump settings. When considering adjusting basal rates to compensate for meals, exercise or alcohol, only 2 participants indicated they used the technique for all three scenarios.
The participant who indicated not checking BG when exercising was 1 of 2 who reported not consuming snacks when exercising and was 1 of 2 who indicated that BG levels did not affect his decision whether or not to exercise. Conversely, of the 12 who reported taking a snack to compensate for exercise, 10 of them indicated that preexercise BG levels had an impact on their postexercise BG levels.
Discussion
Consistent with our findings, previous studies found that most participants reported a variety of self-management behaviors when drinking, such as checking BG, adjusting carbohydrate intake and/or insulin.4 -6 These studies focused on emerging adults and alcohol consumption while our study used a wider age range of participants (25 to 69 years), and we also identified factors that participants said affected BG control when drinking. Also, consistent with our findings, a recent online survey conducted by Pinsker et al found that a variety of techniques were used by patients on insulin pumps or multiple daily injections to compensate for exercise, such as eating a snack, delaying exercise if BG levels are low, or reducing basal insulin. 2
Groat et al and Grando et al analyzed real-life and self-reported data from insulin pump users to determine how insulin bolusing decisions correlated with exercise and alcohol behaviors.8,9 The first study identified inter- and intrasubject variability in behaviors while the second study revealed inconsistencies between self-reported compensation techniques for exercise and alcohol when compared against observed “real-life” actions. It was also found that there was a considerable lack of knowledge amongst the participants on some of the factors that influence BG when consuming alcohol. In the second study, participants asked for more information about alcohol’s effects and in this study over half reported having no knowledge on one or more of the presented factors. Both studies showed that self-reported compensation techniques do not always translate into self-management strategies recorded by diabetes technology (eg, insulin pump).
Conclusions
When taken together with previous data (which focused on actual behaviors), these survey results (which assess perceptions) confirm the considerable inconsistency patients have about incorporating carbohydrate, alcohol, and exercise into decisions about self-management behaviors. Educational and training material that help patients better understand the effects of alcohol and exercise on diabetes management are needed. Bedside tools that can merge and analyze perceptions with behaviors would be helpful in providing feedback to patients and designing educational programs. This study focused on a specialized subset of patients with T1D on insulin pumps. Similar studies should be done in patients on multiple daily injections to see if the findings are similar.
Footnotes
Abbreviations
BG, blood glucose; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by iDECIDE: Patient-Centered Decision Support Based on Device Data (1U54HL108460), funded by NLM.