
Abstract
In recent years, continuous intraperitoneal insulin infusion (CIPII) has become a favored treatment alternative for patients with subcutaneous insulin resistance, mainly due to its ability of mimicking physiological conditions of insulin absorption. CIPII has been shown to improve glycemic control as well as to reduce hypoglycemic events and to lead to increased patient satisfaction and quality of life (QoL). Among CIPII delivery systems, Diaport stands out due to its low side effects, its demonstrated clinical efficacy and the potential for integration into closed-loop systems.
Continuous intraperitoneal insulin infusion (CIPII) has been employed for the treatment of diabetes since the 1980s. Currently, this is a preferred treatment option for those patients presenting subcutaneous insulin resistance. 1 Subcutaneous insulin resistance is a rare syndrome, often misdiagnosed, in which patients with poorly controlled glucose levels are thought to suffer from insulin degradation in the subcutaneous tissue by protease activation.2,3 There are, however, other studies on patients where no degrading activity was found subcutaneously, despite extreme insulin resistance. 4 Several treatment approaches have been used to deal with this situation, namely, oral antidiabetic medication, continuous ambulatory intravenous insulin infusion, and last CIPII, which has been proposed to be the best solution for this problem.4,5
Moreover, recent data suggest it might be helpful to reduce the frequency of hypoglycemic events, and constitutes a last treatment option for those patients unable to reach adequate glycemic control despite standard therapy with multiple insulin injections per day or continuous subcutaneous insulin infusion (CSII).6,7
Intraperitoneal insulin administration mimics physiology more closely than standard therapies. 1 Moreover, in cases of subcutaneous insulin resistance it is preferable to intravenous insulin administration, which has several inherent risks, mostly increased infection rates and an increased risk of thrombosis and vascular damage.8,4 CIPII is advantageous for various reasons: first, it allows a faster blood glucose normalization after a meal with reproducible and more predictable insulin profiles than CSII;9-12 second, since most of the insulin is absorbed through the portal venous system, 13 there is an improved hepatic uptake and lower peripheral plasma insulin levels than with intravenous administration. 14 Last, intraperitoneal insulin may improve glucagon secretion and hepatic glucose production in the face of hypoglycemia by alleviating peripheral hyperglycemia 15 and/or by increasing hepatic sensitivity to glucagon/glucose utilization during hypoglycemia.
Numerous clinical trials as well as observational studies have shown a decrease in HbA1c as well as a lower incidence of hypoglycemia with CIPII in comparison with CSII.7,16-24 Glycemic variability (standard deviation of capillary glucose) was also smaller with CIPII therapy.17,20,22-25 Moreover, long-term data from small, nonblinded studies show stabilization of HbA1c levels and lower risk of hyperglycemia.8-9 In addition, CIPII could be advantageous for closed-loop insulin delivery systems, due to a fast insulin absorption.26-28 CIPII has also been reported to be beneficial in terms of QoL as well as to have physiological effects beyond glycemic control.24,29,30
CIPII can be conducted either by the implantation of programmable pumps10,16,17 or by means of a percutaneous port connected to an external pump for insulin delivery.12,22,31,32 One method of CIPII administration involves the use of percutaneous access devices,33,34 its latest implementation being the Accu-Chek® Diaport system (Roche Diabetes Care, Mannheim, Germany). 35 This report aims to summarize all evidence supporting this system as part of a CIPII therapy for T1D treatment.
Intraperitoneal Insulin Delivery for Type 1 Diabetes Management
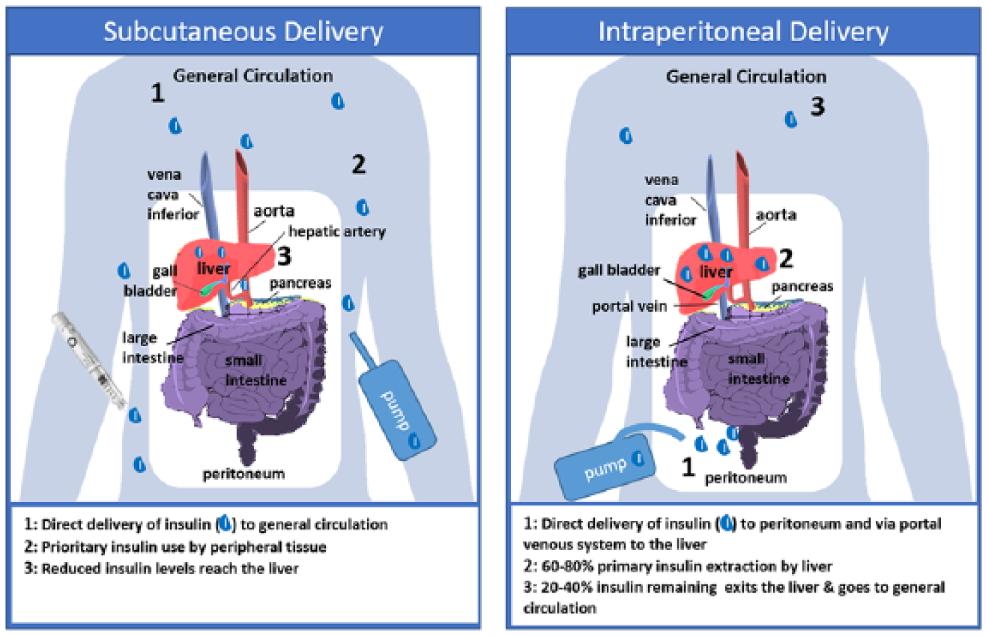
Portal insulin administration—via the umbilical vein—has been shown to be more beneficial in T1D treatment than peripheral insulin administration both in animal models and in humans.36,37 In a similar but less invasive way, intraperitoneal insulin administration permits its absorption via the capillaries of the visceral peritoneum into the portal vein. This absorption will be faster or slower depending on factors such as injected volume, insulin concentration or injection duration, but it will be mostly absorbed directly into the portal system and detectable already within a minute after administration. 1 4 Due to the portal absorption, insulin uptake at the liver is higher, with first-pass liver insulin extraction right after absorption. This in turn achieves a greater reduction of peripheral plasma insulin levels than with subcutaneously administered insulin. Among other likely positive effects are the improvement of the glucagon secretion and glucose production in the liver in response to hypoglycemia and/or exercise. This is possibly either because lower peripheral plasma insulin might restore glucagon release or due to a restoration of hepatic sensitivity to glucagon/hepatic glucose utilization during hypoglycemia.6,15 Subcutaneous delivery, specially of fast-acting insulins, is preferred to multiple daily injections (MDI), among other reasons because contrary to MDI, an increase in bolus-delivered dose does not alter the time-to-peak and the duration of effects. In contrast to subcutaneous delivery, intraperitoneal delivery is characterized for faster effects and a stark reduction of glucose variability. 38 In general, human insulin is preferred for CIPII, even when close attention to insulin aggregation and pump blockade is needed. 39 For a depiction of differences between subcutaneous and portal delivery see Figure 1.
Intraperitoneal insulin administration.
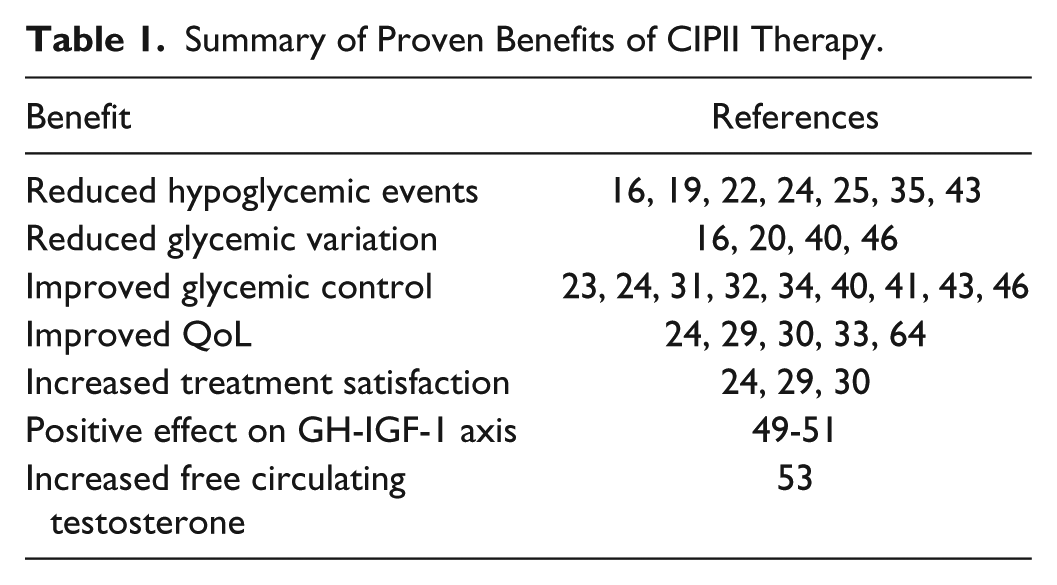
Next, we summarize some of the beneficial aspects of CIPII described thus far. Table 1 shows a summary of evidence for/against CIPII.
Summary of Proven Benefits of CIPII Therapy.
Glycemic control. Several clinical trials have compared CIPII, via an implantable pump, with insulin injections or CSII for glycemic control in T1D patients. A 6-month, randomized, prospective, cross-over study on 10 patients described an improvement in HbA1c as well as in the frequency of hypoglycemia in patients treated with CIPII versus those on multiple daily insulin injections. 20 Another 6-month trial on 21 T1D patients, however, did not find differences between patients treated with CIPII and multiple daily injections, but concedes that CIPII can be beneficial for maintaining a low level of glycemic fluctuations. 40 A more recent 16 month, open-label, randomized, prospective, cross-over study on 24 patients with poorly controlled T1D compared CIPII with subcutaneous insulin delivery either with CSII or MDI. The study found an improved glycemic control in the CIPII group versus the CSII treated group—absolute mean HbA1c difference −0.76% (95% CI −1.41 to −0.11) (P = .03)—without an increase of reported hypoglycemia. 23 A retrospective longitudinal analysis with CIPII usage data from 1983 to 2005 (48 patients) concluded that CIPII improves glycemic control along with less self-reported hypoglycemia in poorly controlled T1D patients. 24 Since the early 1990s there are reports on the use of percutaneous access devices as CIPII delivery mechanism: an initial pilot study on 6 patients 34 as well as a small prospective study 31 reported an improvement in diabetic control but there were some device related complications that needed refinement. In the study, it also was reported that in patients with a clinically proven subcutaneous insulin resistance the daily insulin dose was largely reduced by intraperitoneal delivery. 31 Despite possible complications, case-study reports recount successful implantation and glycemic control in a pregnant patient, 33 in a child with scarce subcutaneous fat tissue and skin infections, 32 and in a patient with inflammation at the insulin injection site. 41 More recently, a prospective, 26-week follow up observational case-control study on more than 180 T1D patients performed a noninferiority analysis of CIPII vs CSII, and reported a noninferior difference in HbA1c levels between both experimental groups. 42
Hypoglycemic event reduction. A number of observational studies, mostly using implantable pumps as CIPII method, also found a lower incidence of hypoglycemic events along with HbA1c reduction.16,19,22,24 Furthermore, an open, randomized, controlled, cross-over, multinational, 12-month study with 60 patients with type 1 diabetes with frequent hypoglycemia and/or HbA1c > 7.0% with CSII, CIPII mediated via an external pump in association with catheter delivery to the portal system showed a reduction of the incidence of severe hypoglycemia to half of that with CSII. 22 A new study has demonstrated a further hypoglycemia reduction up to 83%. 35 The results of long-term studies also corroborate the stabilization of HbA1c levels and the lower occurrence of hypoglycemia in comparison with intensive subcutaneous insulin administration.25,43
Glycemic variation. Glycemic variation is not only supposed to help predict hypoglycemic events and other diabetes-related complications, but it is also a very important aspect of glycemic control, that has been suggested to be a further independent risk factor for diabetes-related complications.44,45 CIPII has been shown superior to subcutaneous insulin administration in several studies, independently of the glucose measurement system employed. Three studies performed before access to continuous glucose monitoring (CGM)16,20,40 and a recent one 46 making use of it, have all demonstrated less glycemic variability with CIPII than with subcutaneous insulin administration (MDI and CSII).
Other physiological effects. Besides its effects on glycemic control, further physiological benefits have been associated with CIPII treatment. The more physiological insulin concentration in portal circulation provided by CIPII could have a positive effect on the GH-IGF-1 axis. In T1D, the lack of endogenous portal insulin circulation leads to insufficient liver insulinization and consequently to a low concentration of IGF-1 and IGF-binding protein-3 (IGFBP-3) and high IGFBP-1 and GH levels. Low IGF-1 levels have been proposed to contribute to increased insulin resistance and an increased risk of long-term diabetes complications by influencing IGF-1 sensitive tissues like the vasculature, bone and muscle.47,48 For instance, a longitudinal study on T1D patients showed higher IGF-1 concentrations with CIPII than with previous CSII. 49 Furthermore, IGFBP-1 levels have been shown to decrease significantly over 6 months of CIPII therapy 50 and, in addition to higher IGF-1 levels, another study found increased IGF-1 bioactivity during CIPII in comparison with CSII treated patients. 51 A collateral effect of low insulin concentration in the portal circulation is a higher production of the hepatic glycoprotein sex hormone-binding globulin (SHBG), which in male T1D patients with normal testosterone levels results in lower free testosterone concentration, even under subcutaneous insulin therapy. 52 CIPII has been shown to significantly decrease SHBG levels in T1D patients that switched from CSII to CIPII, 53 and therefore constitute a potential advantageous alternative for male patients with diabetes. Lipoprotein metabolism, which is also affected by abnormal insulin levels, is improved by CIPII induced lower peripheral circulating insulin, which has been shown to normalize cholesteryl-ester-transferase and lipoprotein lipase (LPL) activity 54 and increase hepatic lipase activity. 55 Despite several studies54-56 that have tried to answer if CIPII produces a benefit or even normalization of lipids/lipoproteins, limitations due to study design make them inconclusive to this effect. Microvascular complications and increased general as well as cardiovascular mortality in T1D patients are related to elevated adiponectin levels, which are also associated with insulin resistance.57-59 Since adiponectin levels, an adipocyte-related peptide hormone, are positively associated with LPL activity and inversely with hepatic lipase activity,60,61 it was expected that CIPII would have a better effect on adiponectin concentration than CSII, however, a small 2-year study on less than 10 patients found no differences between treatments. 62 Another study on differential effects of CIPII versus CSII on metabolism focused on vitamin D, and reported no differences in calcitriol (1,25-dihydroxyvitamin D) levels but a higher plasma concentration of calcidiol (25-hydroxyvitamin D) in CIPII treated individuals, which may be due to the better stimulation of the enzymatic activity of the hepatic 25-hydroxylase which transforms cholecalciferol (vit. D3) and ergocalciferol (vit. D2) to calcidiol. 63
Nonphysiological effects. Other effects, such as QoL have been shown to improve with CIPII. For instance, various cross-over trials showed a significant improvement on self-reported QoL during CIPII treatment in comparison with CSII therapy, the same was true for other randomized trials24,29,30 and several case studies.33,64 Apart from QoL improvement, treatment satisfaction was also higher with CIPII than with CSII.
Potential for Closed-Loop Insulin Delivery Systems (Artificial Pancreas)
Closed-loop insulin delivery systems are based on a continuous glucose monitoring (CGM) system that sends information to a controller which, by running an algorithm, adjusts the insulin output of a pump in an automatic manner, thereby conducing to a better glycemic control.28,65-69 However, insulin delivery via CSII has the problem of the slow insulin absorption and a relatively high concomitant risk for hypoglycemia. 70 CIPII as part of a closed-loop system would potentially imply an improvement on both issues, due to the almost physiological insulin absorption route, which allows a faster blood glucose normalization after a meal 9-12 and the positive results obtained with CIPII for hypoglycemia control.16,19,22,24,25,43 A small study on the use of intraperitoneal insulin delivery as part of a closed-loop system also showed the potential for this combination. 27
Suitability of CIPII Therapy
CIPII is recommended for diabetes patients with the following characteristics:
Frequent severe hypoglycemia during subcutaneous insulin therapy
Hypoglycemia unawareness
Subcutaneous insulin resistance
HbA1c targets not reached (or only at the expense of an increased frequency of hypoglycemic episodes)
High insulin requirements in marked insulin resistance
Lipoatrophy associated with subcutaneous insulin
Insulin-associated lipohypertrophy not controlled by injection site rotation
Skin disorders interfering with subcutaneous insulin administration
Subcutaneous site issues, such as allergic reactions to tapes, nickel or Teflon, as well as insulin absorption issues
Marked fluctuations of glucose levels and insulin requirements during subcutaneous insulin therapy (brittle diabetes)
However, CIPII is not suitable for every diabetes patient. There are a number of contraindications. For example,
Presence of high insulin-antibody levels
Poor therapy compliance
Evidence of psychiatric conditions
Gastrointestinal disorders (colon disease, peritoneal adhesions . . .)
Unsuitability for external pump use in CSII
In addition, there are situations where CIPII might have an increased associated risk. Namely, patients with severe impairment of liver function, severely impaired immune response or those receiving concomitant drugs by intraperitoneal infusion (eg, chemotherapy) or under CAPD. 69
A marked and sustained elevation of anti-insulin antibodies (IAs), possibly due to the use of unstable insulin and consequently, the formation of immunogenic aggregates of insulin has been reported with CIPII. 71 Even when the clinical impact of these circulating anti-IAs is not yet clear, some studies imply a possible retarding effect on insulin action, leading to a worsening of postprandial hyperglycemia and/or to unexpected hypoglycemia. 71 However, another study found no significant effects on metabolic control from the increased presence of anti-IAs, and others consider the clinical effects of reduced impact on glycemic control or diabetes-related complications.71,72
An Improved CIPII System
As mentioned previously, port-mediated systems are an alternative to implantable pumps for CIPII treatment. In summary, this new system facilitates insulin infusion into the peritoneal cavity using the Spirit Combo insulin pump and a special stainless steel ball cannula infusion set. The system involves a titanium port-body with a flexible catheter that is to be placed in the abdomen. The top of the port with the membrane sits above the surface of the skin by approximately 5 millimeters. To help stabilize the port, a flower-shaped plate (Ø26 mm) and a polyester felt band that acts as a microbial barrier, are placed under the skin during a surgical procedure. All system components are depicted in Figure 2.

System components.
Clinical Evidence
Despite reports on earlier percutaneous access devices for CIPII27,32-34 described an improvement in diabetes control, there were also accounts of device-related complications27,32-34,73 that have been recently resolved by the development of the technology. To date, only two clinical trials have employed this system for CIPII treatment and compared it to CSII. The first, a large, open, randomized, controlled, cross-over, multinational, 12-month clinical trial on 60 T1D patients with frequent hypoglycemia and/or HbA1c > 7.0% and previous CSII treatment were assigned either to CIPII therapy with this new system or a continuation of CSII. In T1D, CIPII via this new system was found to reduce the incidence of severe hypoglycemia—34.8 vs 86.1 per 100 patient years. Despite other glycemic control-related parameters like HbA1c, mean blood glucose, and glucose fluctuations were not statistically different between groups, CIPII was reported to improve QoL with no weight gain. As in previous reports of older percutaneous access devices some adverse complications like port infection, insufficient insulin delivery or abdominal pain were reported, yet appropriate control of system functioning should overcome these limitations. 22
A recent 12-month, open, mono-center, single-arm, interventional clinical trial (NCT01483352) on 12 T1D patients unsuccessfully treated with subcutaneous insulin infusion (CSII)—patients with frequent or severe hypoglycemia and/or an HbA1c > 8.5%—evaluated its suitability to perform continuous intraperitoneal insulin delivery. The initial report on the 12-month data found no major issues regarding surgical procedures, tolerability and function of the system. Minor local infections around the port could be easily treated locally and with oral antibiotics. Frequent catheter obstructions were found when in combination with insulin lispro. However, changing to human insulin effectively resolved this issue. The analysis of glycemic outcomes showed a significant improvement of HbA1c after 6 months (7.6% ± 0.6% SD, P = .002), with a similar trend toward improvement at 12 months (8.4% ± 0.2% SD, P = .07). Continuous glucose monitoring (CGM) showed significant improvements in the percentage of interstitial glucose values above 180 mg/dL (53% baseline versus 38% at month 6, P = .036), and in the percentage of glucose values within the target range 70-180 mg/dl (45% vs 58%, P = .027), without increase in hypoglycemia. With respect to hypoglycemic events, the intervention also dramatically reduced the occurrence of severe hypoglycemia, from 12 cases/year before this therapy to two cases afterward. Furthermore, therapy satisfaction was rated high by study participants and so was QoL. 35 Recently published case-study reports also reflect on the benefits both psychological and physiological of this device for diabetes control. 35
In summary, this newly developed system for CIPII represents a valuable treatment alternative for patients where CSII has proven unsuccessful for maintaining an adequate glycemic control.
Advantages Versus Other High-End Insulin Therapy Approaches
Despite the development of new fast-acting insulins like aspart, lispro, and glulisine that can better mimic pancreatic insulin secretion due to a rapid onset and fast reached peak, they are still not as fast and short-acting as needed. 74 Therefore, CIPII stands currently as the best method to achieve a closely resembling physiological insulin delivery.
Another alternative to achieve physiological insulin production are pancreas or islet cell transplants. However, while pancreas transplantation is a treatment of choice for selected T1D patients to provide insulin independence, islet transplantation is, to date, still an experimental procedure aimed to avoid hypoglycemia. 75 Although, if successful, both alternatives represent the only biologic treatment options to prevent long-term hypoglycemia in patients with type 1 diabetes, several considerations make these techniques a less than desired option for many patients, namely the need for immunosuppressive therapy, the high rejection rate, and the need for donors, without mentioning the inherent risk of the surgery. Moreover, the cost of these types of transplants is certainly high. 76 Because of these disadvantages, CIPII stands as a preferable alternative for glycemic control in patients with brittle diabetes.
One of the main advantages of CIPII via this system in comparison with insulin administration via programmable implantable pumps is that it provides intraperitoneal insulin delivery at a lower cost and with higher patient autonomy. The elevated cost of implantable pumps is related not only to the device cost itself, but also to the man-time cost needed to refill the pump reservoir with insulin at hospital every 6-8 weeks and to maintain reliable insulin delivery, as well as the regular need for pump extirpation due to end of battery life. Furthermore, an external pump system allows more flexibility and autonomy to the patient; it is easier to repair/update and offers the possibility of changing to a closed loop approach.27,38
The most reported complications of CIPII via implantable pumps are related to the delivery system. Common complications refer to catheter occlusions (≈30%), pump dysfunction (17.1%), pump replacements due to end-of-battery life and, unfrequently, infections leading to pump removal.19,77,78 In addition, a study reported no pump-related complications in a 15-year period in 80% patients under CIPII. 77 By comparison, the most common treatment-related severe complications of CIPII via this new delivery system were infections at the port site (0.025 events/patient month), replacement of 8 catheters used with fast acting insulin (0.17 events/patient month), and 7 catheter replacements due to catheter occlusion with human insulin (0.02 events/patient month). Only one case report found severe complications associated with an old generation of percutaneous access device for CIPII, namely 3 catheter obstructions and a subcutaneous access that led to removal of the system. 79 Therefore, CIPII via an external pump with direct insulin delivery to the portal circulation represents a safer and more comfortable way of CIPII administration than implantable pumps.
Conclusion
CIPII has achieved better results than subcutaneous insulin delivery (CSII or MDI) in the treatment of T1D in several clinical trials. Despite the invasiveness of the two possible delivery systems, an implantable pump or an external pump connected to direct delivery via catheter, CIPII constitutes a first line treatment option in severe subcutaneous insulin resistance, and it is a preferred alternative for cases of “brittle diabetes”. Based on its low side effects, economic and patient autonomy reasons, Diaport is preferable to implantable pumps as a delivery system for CIPII therapy. Clinical results of the recently optimized version confirm its clinical efficacy as well as a reduction of system-associated complications. Moreover, recent data underline its potential for hypoglycemia reduction and thanks to the unique insulin kinetics provided by the intraperitoneal delivery, stands as an ideal alternative for closed-loop systems.
Footnotes
Abbreviations
AI, anti-insulin antibodies; CAPD, continuous ambulatory peritoneal dialysis; CGM, continuous glucose monitoring; CIPII, continuous intraperitoneal insulin infusion; CSII, continuous subcutaneous insulin infusion; GH, growth hormone; IGFBP, IGF-binding protein; IGF1, (GH)–insulin-like growth hormone-1; LPL, lipoprotein lipase; MDI, multiple daily injections; QoL, quality of life. SD, standard deviation; SHBG, sex hormone-binding globulin; T1D, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Medical writing was supported by an unrestricted educational grant from Roche Diabetes Care.