
Abstract
Finger stick capillary plasma glucose, measured in the clinical biochemistry laboratory, may be used as a comparator glucose value in medical device studies. 1 Capillary samples destined for the laboratory inevitably require blood volumes that are substantially larger than capillary samples collected for glucose meter readings. Using currently available methodology, deep (rather than shallow) lancing is required for larger volume samples but this may increase hemolysis. 2 Diabetes clinicians and scientists will already be aware of the difference between intracellular and extracellular glucose concentration, which necessitates a conversion factor of around 1.11, when converting glucose meter (whole blood) finger stick values to a plasma equivalent. 3 Hemolysis can disrupt this differential glucose concentration, lowering the measured concentration of plasma glucose. 4
One expert stated, “To date, few laboratories have been adventurous enough to attempt measurement of hemolysis rates for capillary blood specimen collection.” 5 Perhaps unsurprisingly, we were unable to find published studies that describe hemolysis rates associated with deep lancing of the finger and subsequent impact on the measurement of laboratory plasma glucose. We therefore report our own experience.
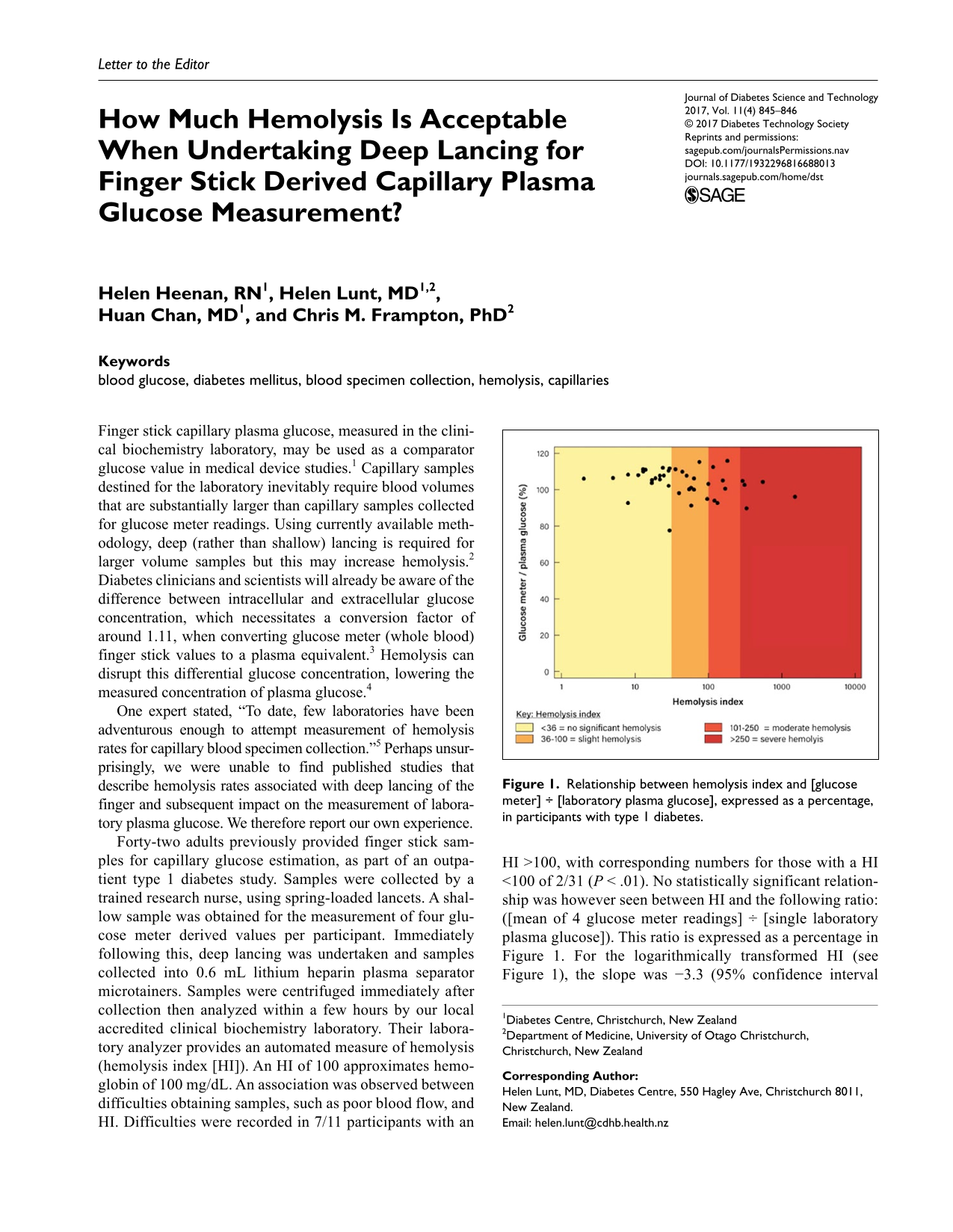
Forty-two adults previously provided finger stick samples for capillary glucose estimation, as part of an outpatient type 1 diabetes study. Samples were collected by a trained research nurse, using spring-loaded lancets. A shallow sample was obtained for the measurement of four glucose meter derived values per participant. Immediately following this, deep lancing was undertaken and samples collected into 0.6 mL lithium heparin plasma separator microtainers. Samples were centrifuged immediately after collection then analyzed within a few hours by our local accredited clinical biochemistry laboratory. Their laboratory analyzer provides an automated measure of hemolysis (hemolysis index [HI]). An HI of 100 approximates hemoglobin of 100 mg/dL. An association was observed between difficulties obtaining samples, such as poor blood flow, and HI. Difficulties were recorded in 7/11 participants with an HI >100, with corresponding numbers for those with a HI <100 of 2/31 (P < .01). No statistically significant relationship was however seen between HI and the following ratio: ([mean of 4 glucose meter readings] ÷ [single laboratory plasma glucose]). This ratio is expressed as a percentage in Figure 1. For the logarithmically transformed HI (see Figure 1), the slope was −3.3 (95% confidence interval −7.5 to +2.1, P = .12). For untransformed values, the corresponding P value remained nonsignificant (P = .19).
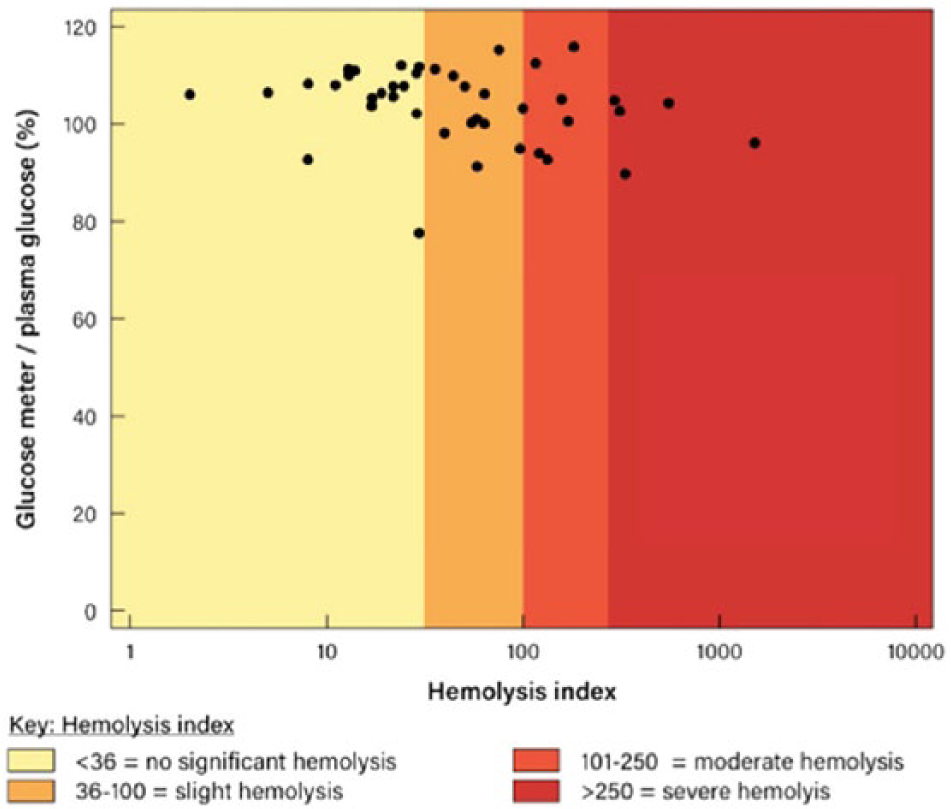
Relationship between hemolysis index and [glucose meter] ÷ [laboratory plasma glucose], expressed as a percentage, in participants with type 1 diabetes.
For glucose-based method comparison studies, it is essential that small measurement biases are identified and minimized. 1 In this exploratory analysis, it was therefore reassuring to observe no major bias in laboratory plasma glucose measurement, despite HI values that might be considered unacceptably high, within other settings. This small study was however powered to detect only major, not minor bias. Given the paucity of publications in this area, we encourage researchers undertaking laboratory measurement of capillary plasma glucose for comparison studies, to report their own HI and associated bias. This will aid discussions about acceptable levels of hemolysis and also how best to minimize hemolysis, when collecting deep finger stick samples for the measurement of glucose.
Footnotes
Acknowledgements
We thank Canterbury Health Laboratories for providing hemolysis results.
Abbreviation
HI, hemolysis index.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HL is on the Speakers Bureau for Sanofi (New Zealand)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.