
Abstract
Background:
Hypoglycemia is associated with increased length of stay in hospital patients, but previous studies have not considered the confounding effect of increased hypoglycemia detection associated with increased capillary blood glucose (CBG) measurement in prolonged admissions. We aimed to determine the effect of recorded hypoglycemia on length of stay of hospital inpatients (LOS) when this mathematical association is subtracted.
Methods:
CBG data were analyzed for inpatients within our health board area (01/2009-01/2015). A simulated CBG data set was generated for each patient with an identical sampling frequency to the measured CBG data set. The mathematical component of increased LOS was determined using the simulated data set. Subtraction of this confounding mathematical association was used to provide measurement of the true clinical association between recorded hypoglycemia (CBG < 4 mmol [< 72mg/dl]) and LOS.
Results:
A total of 196 962 admissions of 52 475 individuals with known diabetes were analyzed. 68 809 admissions of 29 551 individuals had >4 CBG measurements made and were included in analysis. After subtraction of the mathematical association of increased sample number, the clinical effect of recorded hypoglycemia is reduced—but persists—compared to previous studies. 1-2 days with recorded hypoglycemia has a relatively minor effect on LOS. LOS increases rapidly if there are ≥3 days with recorded hypoglycemia, with an increase of 0.75 days LOS per additional day with hypoglycemia.
Conclusions:
This technique increases accuracy of economic modeling of the impact of hypoglycemia on health care systems. This could assist study of the impact of hypoglycemia on other outcomes by factoring for bias of increased sample numbers.
Amongst hospitalized patients, patients with diabetes mellitus are over represented and may account for up to 25% of an inpatient population despite accounting for only 5-8% of the general population.1-3 While complications of glycemic control may have led to hospital admission in these patients, admission is often for other medical or surgical conditions. Aside from the pathology leading to hospitalization, the management of preexisting diabetes is an important consideration in optimal patient management. It has previously been reported that the length of hospital admission and mortality is increased in patients with diabetes.1,2,4,5 These associations have informed guidelines on glycemic targets for inpatients with diabetes in hospital. 6 The economic burden of diabetes care is increasing and was estimated as $245 billion in 2013. The largest proportion (45%) of the medical expenditure making up this cost is attributable to inpatient care. 7
Episodes of hypoglycemia have been demonstrated to be associated with increased mortality, poorer health outcomes and increased length of stay (LOS).1-3 In a frequently cited article, Turchin et al 1 examined the impact of recorded hypoglycemia on the LOS of hospital inpatients and inpatient/outpatient mortality. In this retrospective cohort study, 4368 admissions of 2582 patients with any type of diabetes and on any treatment who were inpatients in their hospital (excluding pregnant women, patients on intensive care units and neonates) were analyzed between January 2003 and August 2004. A threshold of less than or equal to 2.8 mmol/l (50 mg/dl) for a hypoglycemic episode was chosen. The association between number and severity of hypoglycemic episodes and LOS and mortality at 1 year was investigated using a multivariate analysis adjusted for the patients demographics, expected LOS, comorbidity index, diabetes complications, eGFR and mean glucose. Turchin and colleagues concluded that for each day with recorded inpatient hypoglycemia, there was an increased LOS in the region of 2.5 “extra” days and an increase of odds ratio of death by 1 year of 65.8%. They concluded that measures should be taken to decrease the frequency of hypoglycemia. 1 In another paper exploring this relationship McEwan et al 3 used a cohort matched by adjustment for age and Charlson comorbidity score to examine the relationship between episodes of hypoglycemia and LOS in UK hospitals. In this patient group, with a mixture of type 1 and type 2 diabetes, LOS was 11.91 days (95% CI 10.96 to 12.94 days) in inpatients exposed to hypoglycemia (defined by international classification of disease coding) versus 4.80 days (95% CI 4.41 to 5.23) in those not exposed. 3
Mathematically an increased total number of samples of any mathematical distribution is associated with a higher probability of returning more values in any given area of that distribution. In hospital inpatients, with increasing LOS, there will be an increased total number of measurements of capillary blood glucose (CBG) for any given daily frequency of sampling. With this increased number of CBG tests, it is more probable that values defined as in the hypoglycemic range will be detected and recorded. It is possible therefore that an increased total CBG sample number is a confounding factor that may be partly or entirely responsible for the association seen between increased LOS and recorded hypoglycemia described in the literature. This effect may also explain the association of recorded hypoglycemia and excess mortality. Patients who are more severely ill and more frail are likely to need to stay in hospital for longer. Although comorbidity risk scores can be used to mitigate this effect they cannot always accurately predict all patients who will have complicated admissions and poor outcomes. It is therefore possible that increased LOS secondary to morbidity, of whatever cause, could be the main reason for the increased number of hypoglycemic episodes recorded.
This study aims to determine the potentially clinically remediable association between hypoglycemia and LOS by calculating the degree to which mathematically predictable hypoglycemia associated with any given number of recorded CBG samples contributes to the association between LOS and recorded hypoglycemia.
Methods
CBG data obtained from all inpatients (excluding patients on pediatric, obstetric and intensive care units) in the Greater Glasgow and Clyde Health Board for the period January 2009 through to January 2015 were analyzed. Our national diabetes database (SCI-Diabetes) was used to identify individuals with a known diagnosis of diabetes. CBG values for each individual within the data set were identified. Admission episodes were identified using the CBG data set, with periods of inpatient stay defined as groups of contiguous CBG measurements where the interval between each measurement was <5 days. Data from all admissions with >4 CBG measures performed during the admission episode were included.
The distribution of all CBG values within the data set was initially plotted and visualized. It was determined that a gamma distribution provided the best fit to this plot.
For each admission within the data set, a gamma distribution was fitted to CBG values, and a simulated data set of CBG values was generated by sampling the fitted distribution. The simulated data set had an identical sampling frequency to the measured CBG data set, and simulated values were ascribed identical timestamps to observed measured CBG values. Measured and simulated CBG values in the hypoglycemic range were identified. Hypoglycemia was defined in line with local and national guidelines as CBG of less than 4 mmol/l (72 mg/dl). Number of days (a day being defined as 00:00-23:59) within which at least one episode of hypoglycemia occurred was calculated using the CBG timestamp data.
LOS was calculated as interval between first and last recorded CBG value. A two-sample Kolmogorov–Smirnov test was performed to assess whether there was a significant difference between the distribution of durations of admission for all admissions with n days with hypoglycemia in observed and simulated data sets, where n ranged from 0 to 9.
The association between the frequency of hypoglycemia in the measured data set and observed LOS represented the sum of both clinical and mathematical factors. For simulated CBG values, as the association between simulated hypoglycemia and LOS represented only the mathematical association, subtraction of the mathematical association from the sum of clinical and mathematical factors gave a measure of the true clinical association between recorded hypoglycemia and LOS as a hospital inpatient. This was plotted against the number of days with hypoglycemia during admission, and a linear regression was performed.
This study was performed in keeping with declaration of Helsinki. No consent was required for this study.
Results
Measured CBG were obtained from inpatients during the period January 2009 through to January 2015 in the Greater Glasgow and Clyde Health Board. A total of 4 201 428 CBG values were obtained from a total of 196 962 individuals. Our national diabetes database (SCI-Diabetes) was used to identify individuals with a known diagnosis of diabetes. In all, 52 475 individuals were identified as having a known diagnosis of diabetes from the total data set. The analyzed data set taking all admissions with >4 CBG measures consisted of 68 809 admission episodes from 29 551 individuals. Data from individuals with both type 1 and 2 diabetes are presented.
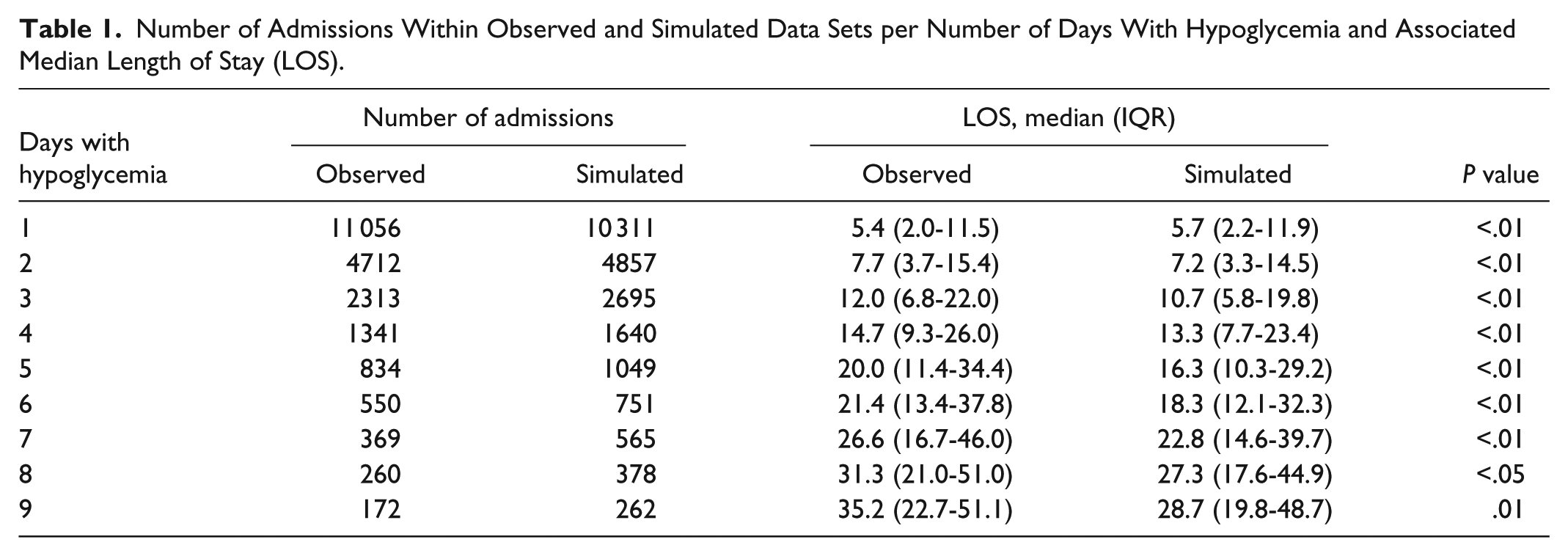
Number of admissions with between 1 and 9 days observed and simulated hypoglycemia are shown in Table 1. Median and interquartile range of duration of admissions per number of days with hypoglycemia is shown, and is plotted in Figure 1.
Number of Admissions Within Observed and Simulated Data Sets per Number of Days With Hypoglycemia and Associated Median Length of Stay (LOS).
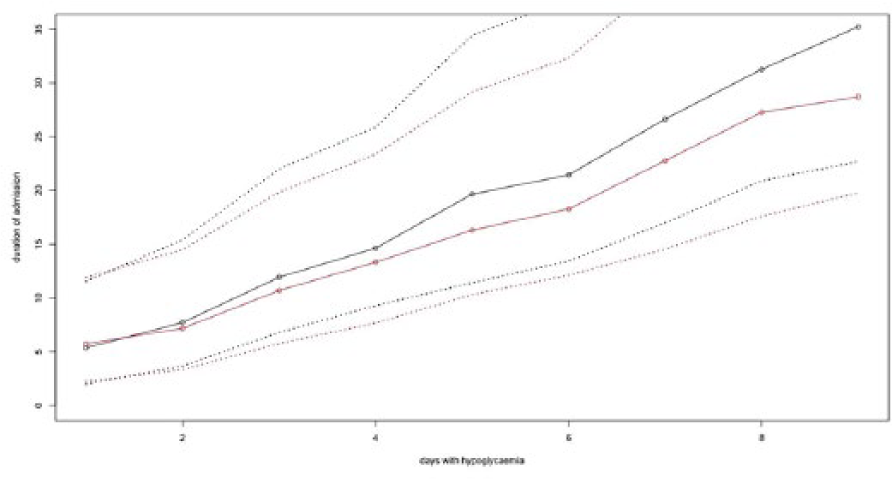
Median and interquartile range of duration of admissions per number of days with hypoglycemia.
The difference between observed and simulated median duration of admission per number of days with hypoglycemia is plotted in Figure 2. A regression line was plotted, with a gradient of 0.75 suggesting an increase of 0.75 days LOS per day with hypoglycemia.
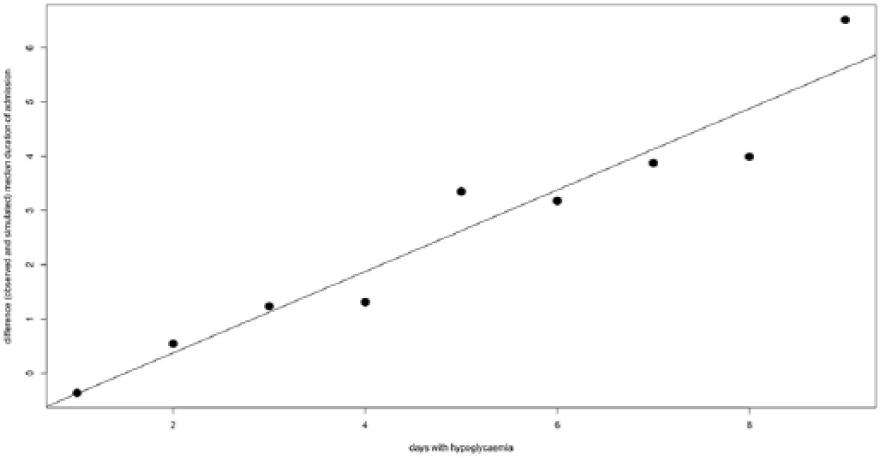
Observed and simulated median duration of admission per number of days with hypoglycemia.
Discussion
As we continue to strive to improve patient outcomes in the context of the economic pressures associated with an aging population, LOS in hospital inpatients has become an important clinical and political topic.5,8 Patients with diabetes are over represented in the hospital inpatient population compared with the general population accounting for up to 1 in 6 patients. 1 Among patients with diabetes treated with insulin or sulphonylurea the risk of hypoglycemia is often an important factor in preventing optimal glycemic control and treating hyperglycemia.2,4 In hospital inpatients hypoglycemia is undoubtedly important as suboptimal management of concurrent diabetes can have a profound impact on patient outcome.1,2,4,5 The UK National Diabetes Inpatient Audit demonstrated that in England around 20 % of inpatients with diabetes experience at least 1 episode of mild biochemical hypoglycemia (>3.0 to <4.0 mmol/l) with 9.9% having severe biochemical hypoglycemia (<3.0 mmol/l) while an inpatient. 9 In Scotland 26.2 % of all admissions were associated with mild hypoglycemia. 10 This highlights the high prevalence and potential importance of hypoglycemia for the inpatient population. Given the potentially large and avoidable impact that hypoglycemia may have on LOS, it is important that an accurate quantification of any association is elucidated. Studies examining association between hypoglycemia and LOS to date have shown a significant increase in hospital stay but have not in our taken into account the potential confounding influence of number of CBG measurements. Turchin et al defined hypoglycemia days as any day with one or more CBG 2.8 mmol/l (<50 mg/dl). This approach is susceptible to bias caused by those patients having longer stays having more opportunities to have low CBGs measured. McEwan et al used clinically coded hypoglycemia events to measure association with LOS. This methodology is likely to include more biochemically severe and clinically impactful episodes of hypoglycemia which possibly explains the larger suggested associated LOS (7.5 extra days compared to 2.5 days in Turchin et al study). This methodology is still potentially susceptible to an ascertainment bias as longer hospital stays will be associated with more CBG tests in total with more opportunity to have hypoglycemia recorded and coded.1,3
The methodology used in our study allows the confounding effect of the mathematical association with increased sample number and recorded hypoglycemia to be identified and accounted for. Using our method to remove the effect of increased sample number as a confounding factor, we propose that although the number of days with recorded hypoglycemia has an impact on LOS, this impact may be lesser than previously proposed. The increased impact on LOS observed previously described is likely to represent the synergistic effect of the true clinical link and the confounding mathematical association with increased sample number. Our study therefore introduces a method of analysis of the clinical association with recorded hypoglycemia and LOS in hospital inpatients which is more representative of the true clinical importance of hypoglycemia.
Our data demonstrate that after subtraction of the influence of sampling number effect, the clinical impact of hypoglycemic days on LOS is reduced but still persists. The clinical impact of 1 or 2 days with hypoglycemia is relatively small, but the impact rises with 3 or more hypoglycemic days, with an increase in LOS of 0.75 days per additional day with hypoglycemia. These results would seem to resonate with clinical experience. Turchin et al in their study of the effect of hypoglycemia on hospital inpatients postulated that each day with recorded hypoglycemia translated into 2.5 further days as a hospital inpatient. The results of our study are in agreement with these findings in that recorded hypoglycemia is associated with an increased LOS. Our data suggest that the impact of recorded hypoglycemia becomes particularly important when it is recorded for 3 or more days in any given admission. In patients with 1 or 2 days of recorded hypoglycemia, there appears to be little impact on the overall LOS. It is likely that patients who have more than 3 days with recorded hypoglycemia represent the most unwell patients and therefore will have a more prolonged inpatient stay. The fact that 1 or 2 days with recorded hypoglycemia doesn’t appear to significantly lengthen inpatient stay may represent patients who are less unwell but may also be due to timely recognition of the problem and preventative steps being taken to avoid further episodes of hypoglycemia. The increased LOS with 3 or more hypoglycemic days emphasizes the need for increased focus on inpatients with recorded hypoglycemia and consideration of accepting less stringent inpatient glycemic control in these patients.
This technique allows more accurate economic modeling of the influence of hypoglycemia on health care systems. Impact of hypoglycemia on other adverse outcomes such as mortality, morbidity, and readmission rates can now also be calculated factoring in the potential influence of LOS and sample number.
Footnotes
Abbreviations
CBG, capillary blood glucose; LOS, length of stay.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.