
Abstract

Previous reports have highlighted concerns about dys-syncrony of diabetes devices,1,2 including hypothetical concerns related to inadvertent transposition of AM/PM settings, 1 but there are few real world descriptions of the clinical effects of dys-syncrony.
A busy working mother with type 1 diabetes, currently on an Animas® Vibe® insulin pump, had been pumping for 7 years. HbA1c was 6.8%. She reported a month of unstable glucose meter levels, including fasting hyperglycemia, prompting a stepwise increase in overnight insulin. In addition, there was problematic daytime hypoglycemia, which was attributed to a recent increase in exercise and decrease in carbohydrate intake. Ongoing hypoglycemia required a decrease in daytime basal insulin and increasingly frequent temporary daytime insulin suspends. The patient undertook manual dosing of bolus insulin.
Insulin dosing history was discordant, when comparing patient history with information uploaded using diasend® software. 3 The patient reported temporary daytime insulin suspends, however diasend® data showed overnight suspends. Running through a pumping troubleshooting checklist, the problem was identified as the pump’s AM/PM clock function being set 12 hours out of phase. The patient had therefore given boluses and temporary suspends in real time (“in phase”), but had delivered preprogrammed basal insulin with a 12-hour phase shift. Basal insulin delivery rates, extrapolated from diasend® data, are summarized in Figure 1.
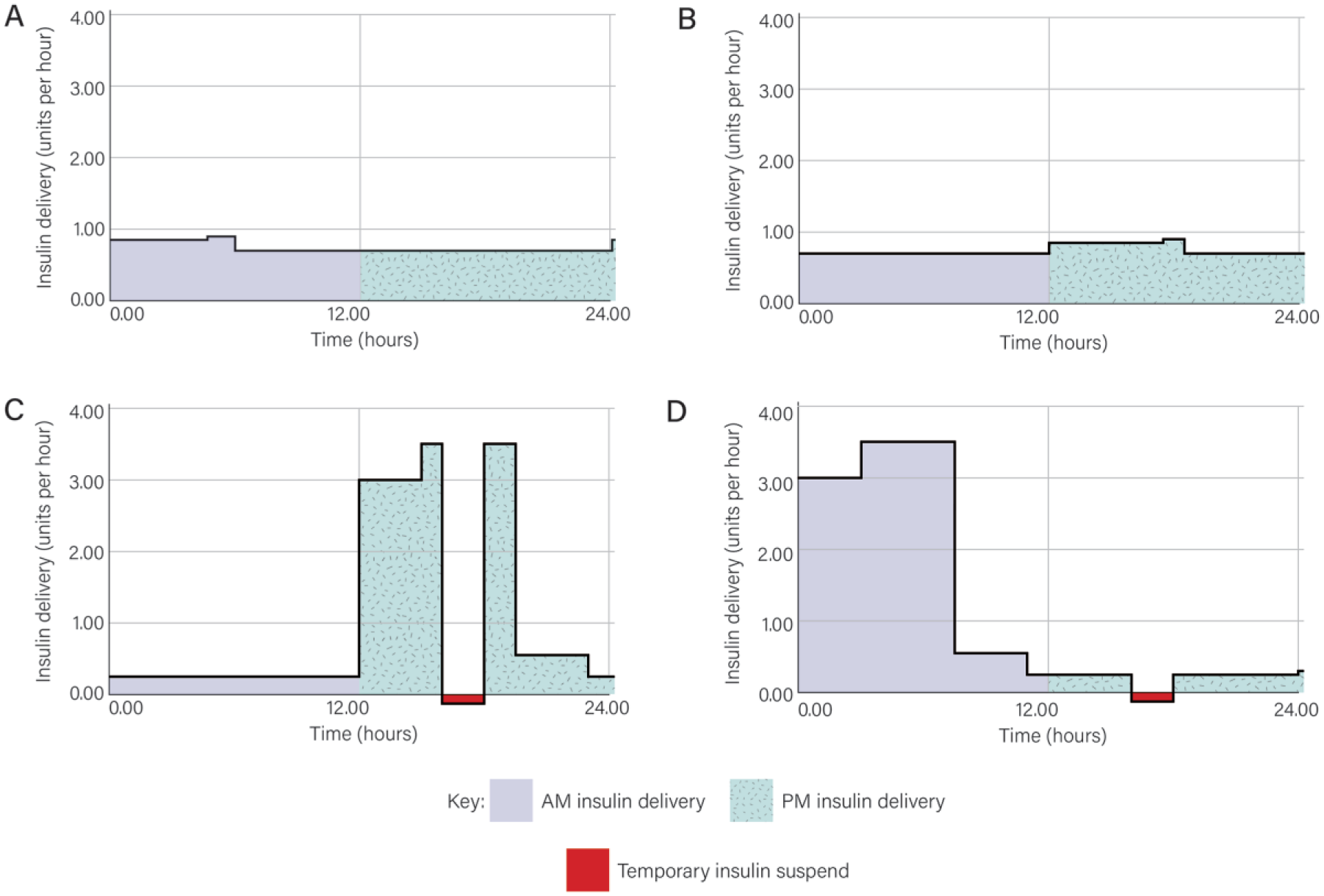
AM-PM basal insulin delivery, before and 1 month after accidental transposition of AM-PM settings. (A) Baseline (usual) insulin delivery. (B) Immediate effect of transposing AM-PM readings on baseline insulin delivery. (C) Effect of stepwise changes in insulin dosing after 1 month; actual dosing. (D) Patient perception of insulin dosing at 1 month, showing a 12-hour phase shift compared to Figure 1C, except for the temporary insulin suspend, which is in phase.
The reason for the incorrect setting of the AM/PM clock was unclear. By default, it was attributed to inadvertent patient error. This AM/PM clock transposition had the effect of causing a positive feedback loop for basal insulin self-adjustment, as follows: Because the baseline (ie, pre-AM/PM transposition) basal insulin delivery was greater overnight than during the day (Figure 1A), a 12-hour time shift in basal insulin delivery (Figure 1B) caused minor waking hyperglycemia. Attempting to correct glucose trends with more “overnight” and less “daytime” basal insulin served only to exacerbate the apparent changes in diurnal insulin sensitivity. The stepwise changes made to basal insulin delivery rates in response to glucose data, fortunately resulted in only partial rather than complete loss of homeostasis. This was because corrections (boluses delivered both during the day and also overnight and also temporary insulin suspends) were given in real time, thereby ameliorating the adverse effects of the 12-hour phase shift in basal insulin delivery (Figure 1D). The patient now uses the pump’s 24-hour clock setting. Glucose stabilized rapidly, on returning to the previous (Figure 1A) insulin regimen.
The above case confirms that accidental pump AM/PM clock transposition has potentially dangerous consequences. This clinical presentation has parallels with the aviation industry’s “system anomaly recognition and recovery techniques.” Teamwork and problem identification using a checklist are keys to correcting such situations. 4
In conclusion, this report highlights the dangers of using the AM/PM pump clock, rather than the 24-hour clock setting. In the absence of global positioning system (GPS)–enabled pumps that show local time, it seems sensible to advise patients who are comfortable with 24-hour (“military”) clocks to use this setting. The report also highlights the utility of including pump clock settings in insulin pump troubleshooting checklists.
Footnotes
Abbreviation
GPS, Global Positioning System.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Helen Lunt is on the Speakers’ Bureau for Sanofi (New Zealand).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.