
Abstract
Aims:
The aim was to evaluate changes in insulin requirements from onset of continuous subcutaneous insulin infusion (CSII) until glucose optimization in type 1 diabetes and to determine patient characteristics to be considered when CSII is implemented.
Materials and methods:
We retrospectively analyzed 74 type 1 diabetic patients over a follow-up of 5 months after starting CSII. Patients without a decrease in HbA1c levels at the end of follow-up were excluded. We compared total daily doses (TDD), basal/bolus distribution, basal diurnal/nocturnal proportion, number of basal segments, and HbA1c levels in relation to sex, age, body mass index (BMI), diabetes duration, and indication for CSII.
Results:
At follow-up, HbA1c decreased by 0.75%, TDD decreased by 18%, basal rate was 60% of TDD, and diurnal basal rate was 60% of total basal rate. Insulin requirements were higher in males and in obese patients. Female patients and patients with longer diabetes duration showed a higher percentage of basal insulin. The number of basal segments was 4.9 ± 2.9. Basal requirements were higher in the second half of the nocturnal period. The dawn phenomenon was more relevant in men. Improvements in glycemic control were more marked in younger patients, in patients with higher HbA1c, in patients using more basal segments, and in patients initiating CSII for glucose control before pregnancy.
Conclusions:
Sex, diabetes duration, and BMI should be considered when initiating CSII. Our findings may help clinicians in clinical decision making regarding CSII therapy.
The number of pump users has increased in the past decades as a consequence of 2 main factors. The first of these is that the technology of insulin pumps has improved significantly, and pumps are now smaller, more reliable, and safer. The second factor is that several studies have demonstrated the superiority of continuous subcutaneous insulin infusion (CSII) over multiple daily injections (MDI) therapy in type 1 diabetic patients in terms of glycemic control, the rate of hypoglycemia, glucose variability, and quality of life.1-5 Nevertheless, there are no clear guidelines or recommendations available for clinicians to facilitate the transition from MDI to CSII.6-8 As a result, glycemic improvement is often delayed because insulin doses need to be adjusted after CSII initiation. CSII is usually started with a reduction of MDI doses of about 20% to 25%, a basal/bolus distribution around 50%/50%, and a flat basal rate. But it is well known that the glucose profile of type 1 diabetic patients depends on many variables, such as diabetes duration, physical activity, and the dawn phenomenon. Short information about the best way to start CSII therapy has been reported in adults. 9 Wider, more useful information about patterns of CSII insulin and patients characteristics is lacking.
Although glucose profiles are intrinsically individual, identifying common patterns could be helpful for decision making, and recommendations for subgroups of type 1 diabetic patients are needed, allowing faster optimization of glycemic control.
The main objective of the present study was to assess the changes in insulin requirements during the transition from MDI to CSII in adults with type 1 diabetes, studying the evolution of insulin requirements, the basal/bolus distribution, the basal rate profile over 24 hours, and the number of basal segments after optimizing glycemic control. In short, we aimed to establish simple guidelines on the basis of patient characteristics that could help clinicians achieve optimal glucose optimization in a shorter period of time.
Methods
The study was approved by local ethics committee and included all patients with type 1 diabetes who started CSII therapy in our department between January 2008 and September 2010. Exclusion criteria were renal failure, medications other from insulin affecting glucose levels, pregnancy, and the absence of reduction in HbA1c levels at the end of the follow-up. Data obtained from the first 5 months post CSII initiation were analyzed in a retrospective study.
Before starting CSII all subjects had been receiving MDI of insulin (≥4 injections/day) for at least 1 year. The MDI regimen included a long-acting insulin analogue once/twice a day (glargine or detemir) in 71 patients and a intermediate insulin (NPH or NPL) 2/3 times per day in the remaining 3 patients, plus a rapid-acting insulin analogue for meals (aspart, lispro, or glulisine). Before starting CSII all patients attended a structured diabetes education program and measured their capillary blood glucose levels at least 4 times a day.
Our educational program for patients beginning CSII included 4 full morning sessions (approximately 15 hours) conducted by a nurse and an endocrinologist. In the 5 months after CSII was started, patients were attended 1 to 4 times by a nurse and at months 1, 3, and 5 by an endocrinologist. Women in preconception care were visited more frequently (monthly). All patients had phone access to the diabetes team around the clock, 365 days a year.
At the start of CSII therapy, the total daily dose (TDD) of insulin was calculated by reducing the TDD used in the MDI regimen by 15% ± 5%. The basal/bolus distribution was 50%/50% in most subjects, except in those who had a proportion in the MDI treatment of basal insulin and premeal insulin higher than 65%/35% or lower than 35%/65%. Basal/bolus distribution was maintained in these patients. Most patients began CSII therapy with only 1 basal rate, but in a few cases this was subdivided into 2 or 3 segments according to previously observed patterns either after self-monitoring blood glucose or with a continuous glucose monitoring system. Patients were encouraged to follow a 3 meal a day diet, but in some cases snacks were included, depending on patient preferences.
We calculated the carbohydrate-to-insulin ratio (from the ratios used on MDI) and the insulin sensitivity factor (1800/TDD), and both were modified along the follow-up separately for breakfast, lunch, and dinner. Pumps used were Medtronic 508 and Paradigm RT, Accu-Chek Spirit, and Animas R2020, and the insulin used was a rapid-acting insulin analogue.
Therapy was modified at each follow-up visit according to glucose measurements (premeals, 2 hours after meals and at bedtime, occasionally at 3-4 hours in the morning). At each visit data from the pump were reviewed and occasionally downloaded to obtain information concerning TDD, the proportion of basal rate and premeal boluses, the proportion of diurnal and nocturnal basal rates (nocturnal period was considered 0-8 hours), and the number of basal segments.
Statistical analyses were performed using SPSS package for Windows version 18. Continuous data were expressed as mean ± standard deviation and categorical variables as percentages. Student’s t test was used to compare quantitative variables, and differences in categorical variables were evaluated using the χ2 test or Fisher’s exact test where appropriate. Groups were compared by 1-way analysis of variance (ANOVA) and correlations between quantitative variables by Pearson’s correlation coefficient. To evaluate changes in variables over time we applied repeated-measures ANOVA. Statistical significance was defined as P < .05.
Results
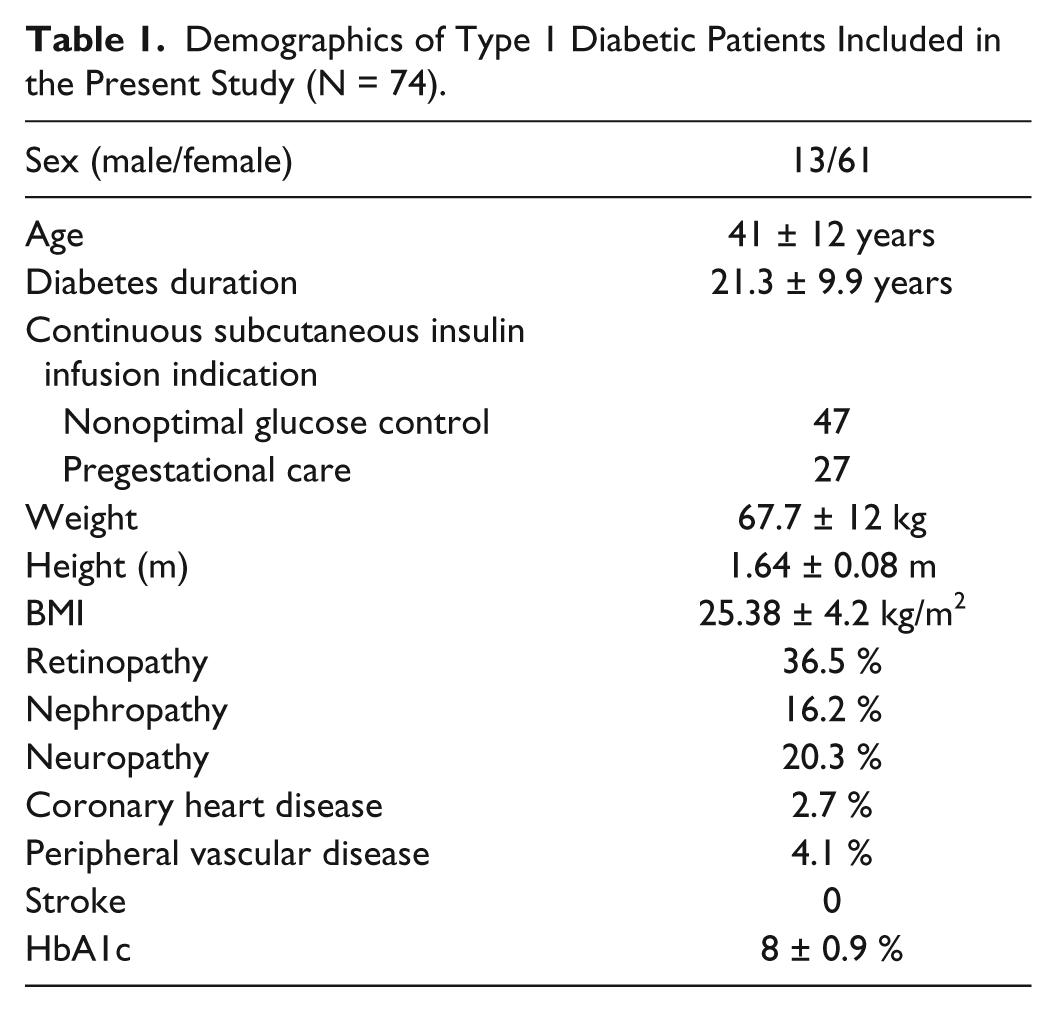
A total of 74 patients with type 1 diabetes were included. Table 1 summarizes clinical features. Table 2 summarizes data from the MDI regimen immediately before starting CSII therapy, data at the beginning of CSII, and data obtained 4 to 6 months later, when glycemic control had improved.
Demographics of Type 1 Diabetic Patients Included in the Present Study (N = 74).
Total Daily Doses of Insulin, Basal/Prandial Distribution, Diurnal/Nocturnal Distribution, Number of Basal Segments, and HbA1c Values Before CSII, at CSII Initiation, and After Optimizing Glycemic Control.
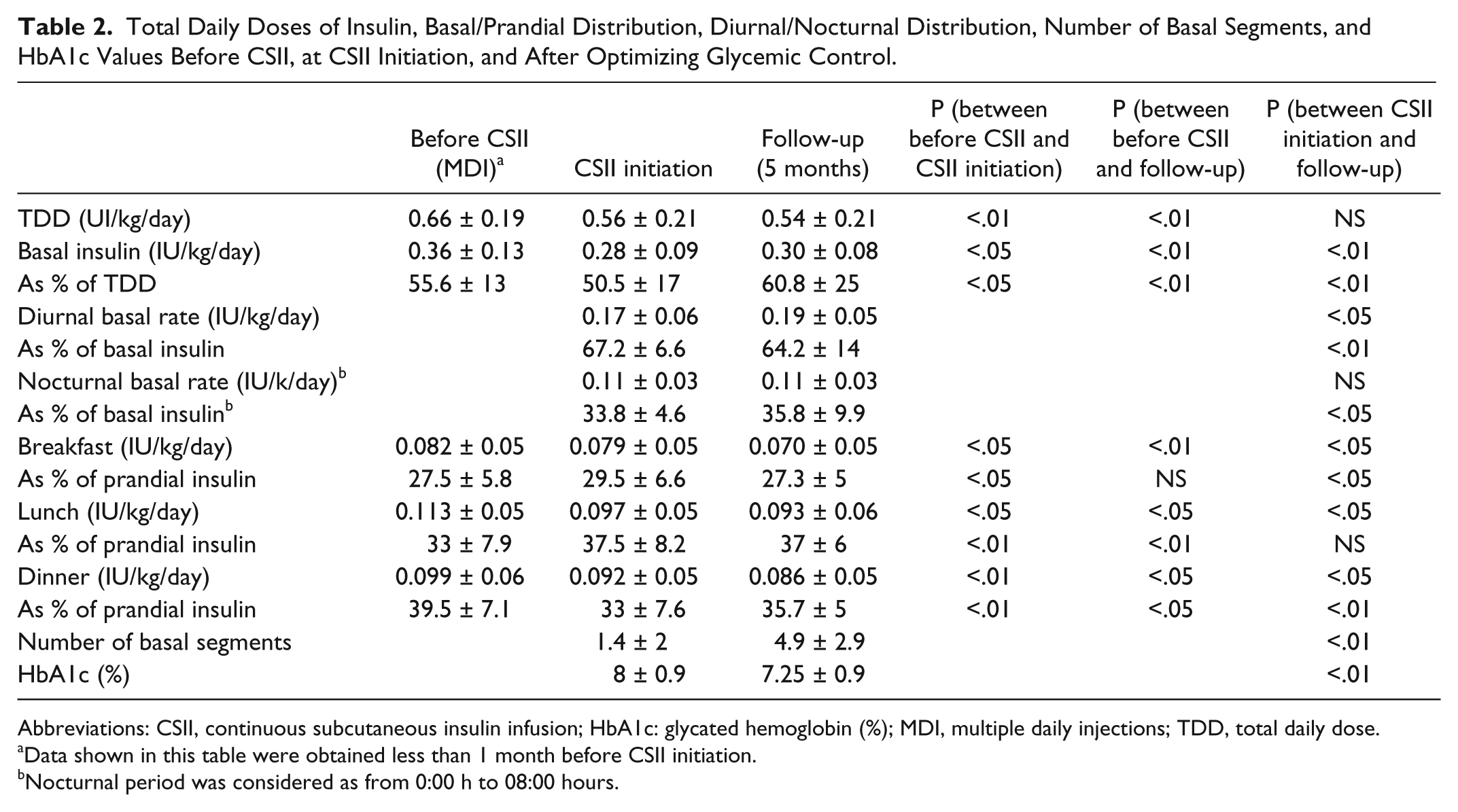
Abbreviations: CSII, continuous subcutaneous insulin infusion; HbA1c: glycated hemoglobin (%); MDI, multiple daily injections; TDD, total daily dose.
Data shown in this table were obtained less than 1 month before CSII initiation.
Nocturnal period was considered as from 0:00 h to 08:00 hours.
Insulin Requirements and Distribution
TDD at the beginning of CSII therapy was reduced by 15 ± 5% (0.66 ± 0.19 IU/kg/day in MDI and 0.56 ± 0.21 IU/kg/day when CSII was initiated; P < .01). At the end of the study the reduction in TDD was 18 ± 5% in comparison with the MDI regimen (0.54 ± 0.21 IU/kg/day; P < .01). TDD at the end of the follow-up correlated positively with TDD prior to CSII (r = .864; P < .001), with diabetes duration (r = .363; P < .01) and also with the proportion of insulin as basal rate (r = .314; P < .05). TDD was higher in men than in women (see below).
Basal insulin requirements comprised 55.6 ± 13% of TDD in MDI, 50.5 ± 17% at the start of CSII (P < .05), and 60.8 ± 25% when glycemic control was improved (P < .01).
The amount of insulin in boluses showed a different distribution between meals before CSII and meals after CSII. Patients on MDI showed the highest proportion of prandial insulin before dinner (39.5 ± 7.1%), but when CSII was started the highest proportion was seen before lunch (37.5 ± 8.2%) and at the end of the study (37 ± 6%; P < .05). Figure 1 shows proportion of basal rate, bolus for breakfast, lunch, and dinner at the beginning of CSII and at the end of follow-up.
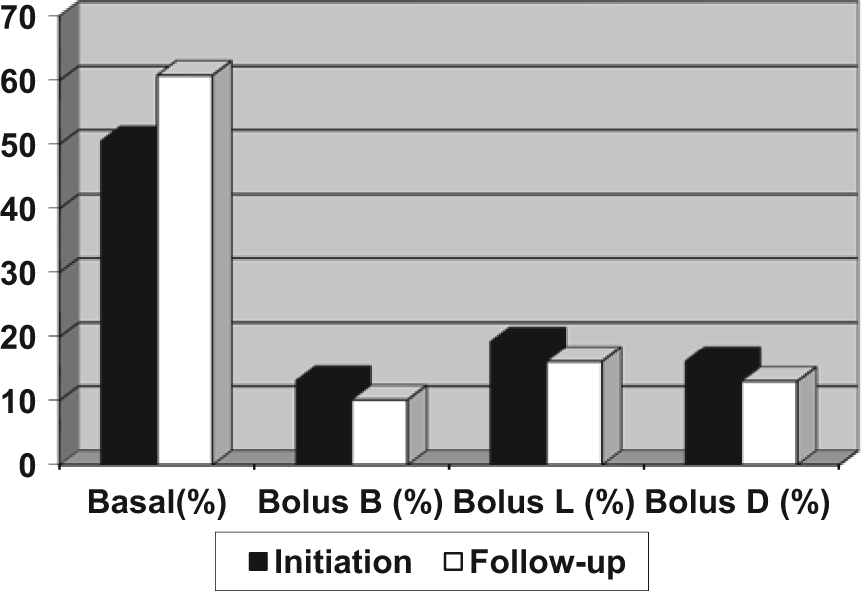
Mean proportion of insulin doses as basal rate and bolus (breakfast, lunch, and dinner) before and at the end of follow-up period in the group of patients studied. Abbreviations: Bolus B, bolus for breakfast; Bolus L, bolus for lunch; Bolus D, bolus for dinner.
The diurnal/nocturnal basal distribution was statistically different at the end of the study when compared to the beginning of CSII. The proportion of the diurnal basal rate decreased significantly (67.2 ± 6.6% vs 64.2 ± 2.9%; P < .01), and the nocturnal basal rate increased accordingly.
The number of basal segments increased significantly from 1.4 ± 2 at the beginning of CSII to 4.9 ± 2.9 at the end of the study (P < .01).
The rate of insulin infusion per hour at the start of CSII was compared with the rate at the end of the study. Insulin requirements were highest in the second half of the nocturnal period and in the evening. However, this distribution was more evident at the end of the study: statistically significant differences were found for the periods 5 to 8 hours and 20 to 24 hours (Figure 2). We found differences according to sex in the rate of insulin infusion per hour at the end of the follow-up period. The rate of insulin infusion was higher in males than in females in the period 4 to 12 hours. The dawn phenomenon was more prevalent in men, with mean insulin requirements >1 IU/hour (Figure 2).
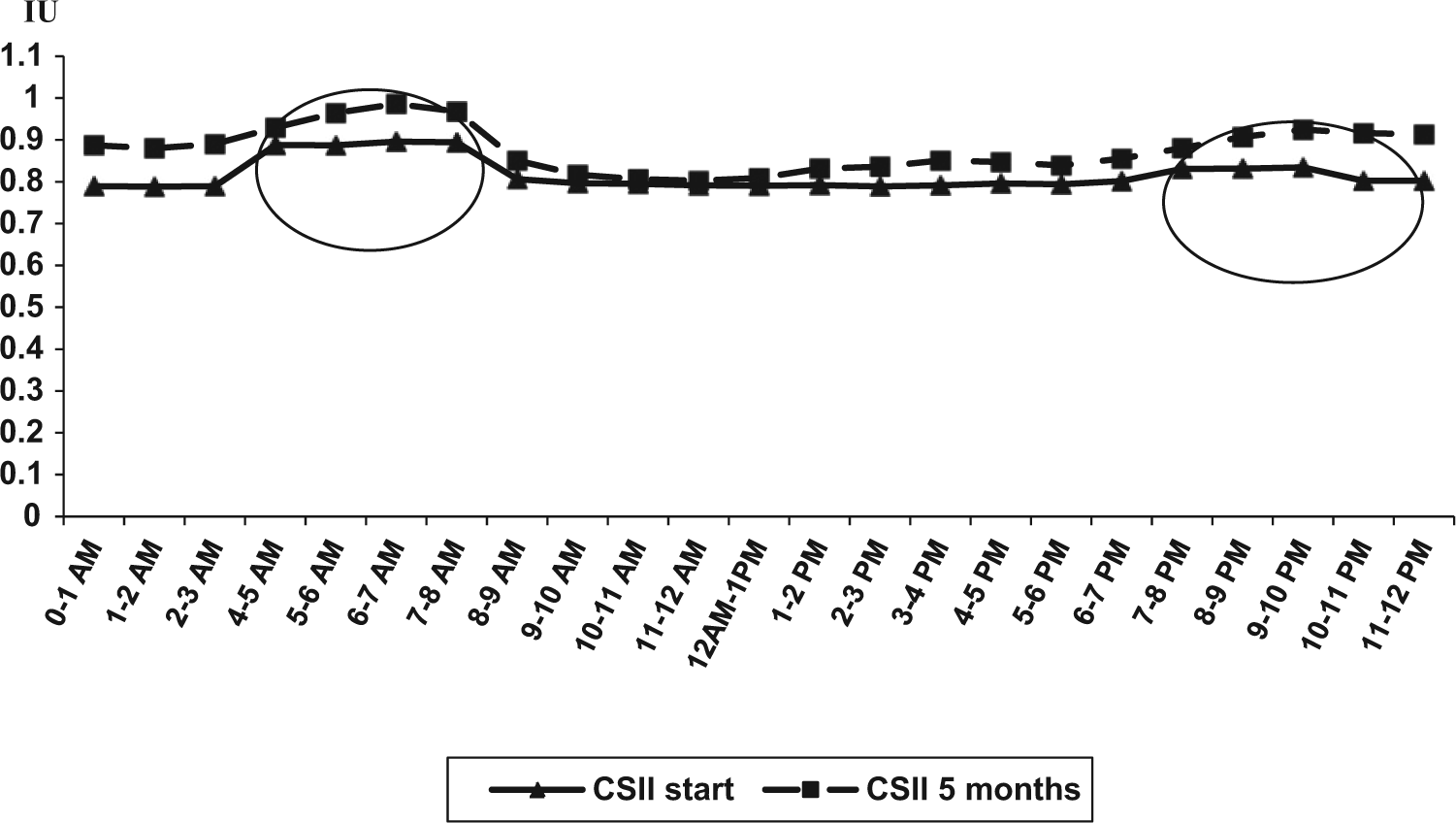
Average insulin infusion rate per hour at the beginning of CSII therapy and at the end of follow-up (5 months later). Differences (P < .05) for the periods 5-8 hours and 20-24 hours were statistically significant.
HbA1c Levels
HbA1c value decreased from 8.0 ± 0.9% to 7.25 ± 0.9% throughout the study (see Table 2). HbA1c levels at the end of the study were positively correlated with HbA1c at the beginning of CSII therapy (r = .680; P < .001) and also with age (r = .385; P < .01). Patients who achieved the objective of HbA1c value <6.5% at the end of the follow-up period were younger (35 ± 7 vs 42 ± 12 years; P < .05) and had a significantly higher number of basal rates per day (7.2 ± 4 vs 4.3 ± 2; P < .05). Women who started CSII therapy to improve metabolic control prior to pregnancy achieved lower levels of HbA1c than the other subjects (6.7 ± 0.7 vs 7.6 ± 0.9%; P < .01). No significant correlations were found between HbA1c levels and diabetes duration, TDD, basal/boluses distribution, or diurnal/nocturnal basal rate.
Diabetes Duration
Subjects with shorter duration of diabetes (<20 years) achieved better glycemic control (HbA1c 7 ± 1 vs 7.5 ± 0.8%; P < .05) than those who had diabetes for a longer time (≥20 years). The reduction in HbA1c levels was also greater in patients with diabetes of more than 20 years than in patients who had the disease for less than 20 years (1% vs 0.4%; P < .05) and the proportion of TDD as basal rate at the end of the study was lower in subjects with shorter diabetes duration (54.3 ± 12 vs 65.8 ± 31%; P < .05). No differences were observed in the number of basal profiles per day in relation to duration of diabetes.
Indication for CSII
Those patients who started CSII therapy to improve metabolic control prior to pregnancy (preconception care) were younger (32.7 ± 4 vs 45.8 ± 12 years; P < .01), they had a shorter diabetes duration (17.8 ± 8.5 vs 23.3 ± 10 years; P < .05), and they achieved lower HbA1c levels at the end of the study than the other patients (6.7 ± 0.7 vs 7.6 ± 0.9%; P < .01). The degree of improvement in HbA1c levels was also higher in patients who started CSII for preconception care than in the other patients (1.4% vs 0.2%; P < .05).
Sex
TDD before CSII therapy (in MDI regimen) was similar in men and women. However, the percentage of basal insulin was lower in men (57.8 ± 13 vs 45.5 ± 10%; P < .01), and the percentage of prandial insulin was higher (42.2 ± 13 vs 54.5 ± 10%; P < .01). These findings were maintained at the end of the study. Again, the percentage of basal insulin was lower in men (49 ± 13 vs 63 ± 23%; P < .05) and the percentage of pandrial insulin was higher (51 ± 11 vs 37 ± 12%; P < .05). TDD was also higher in men (0.63 ± 0.3 vs 0.53 ± 0.2 UI/kg/day; P < .05) at the end of the follow-up (see Figure 3). No other differences between sexes were found in terms of weight, BMI, diabetes duration, diurnal/nocturnal basal rates, or number of basal segments per day.
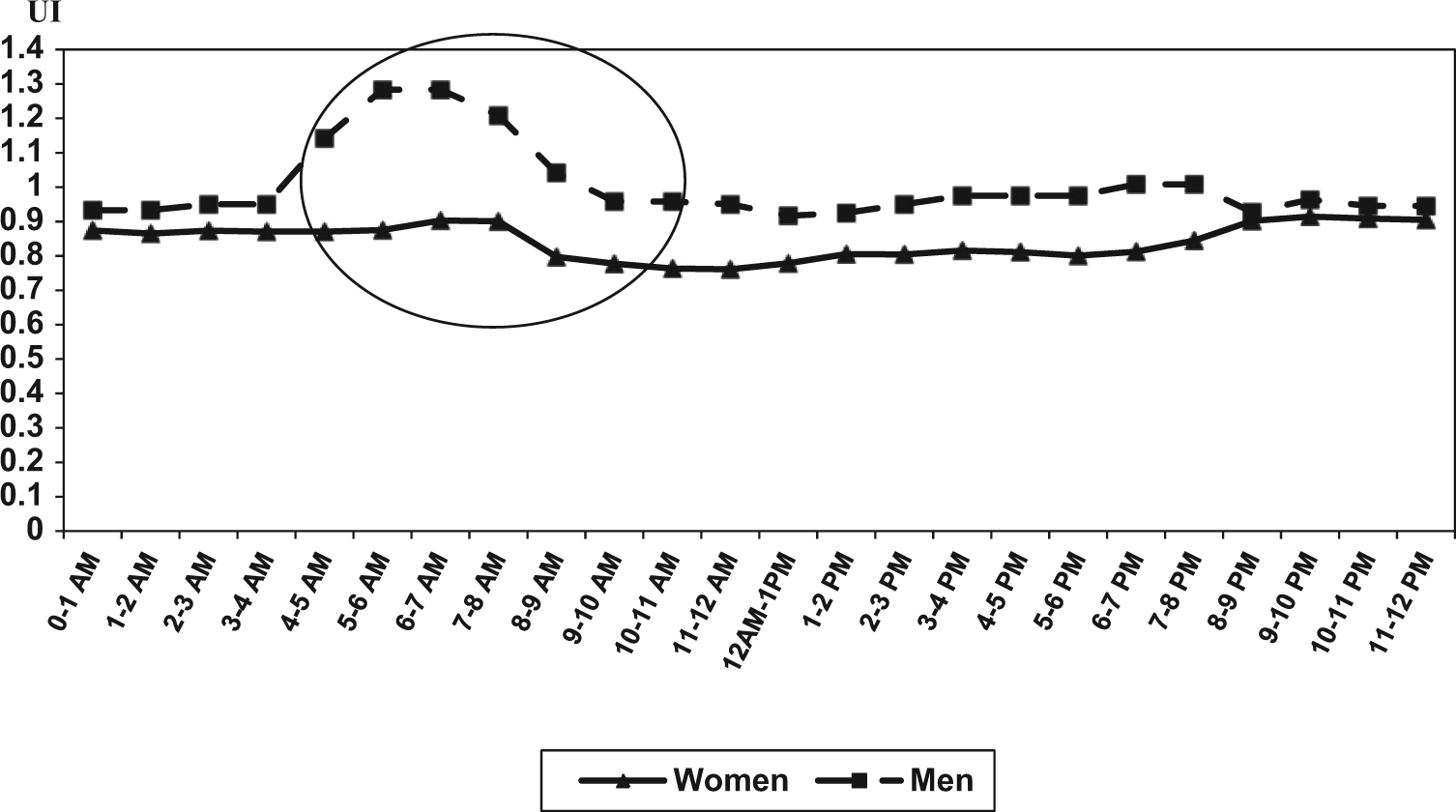
Average 24-hour basal rate profile at the end of the follow-up period (5 months after starting CSII) of the patients included in the study according to sex. Statistically significant differences (P < .05) were found for the period 4-12 hours. In this period of time the doses/hour of insulin were higher in men than in women.
Women achieved better glycemic control than men (7.1 ± 0.9 vs 7.8 ± 0.7%; P < .05) and had a higher reduction in HbA1c levels (0.6% vs 0.3%; P < .05). However, after excluding women starting CSII for pregestational care, the differences in HbA1c values between men and women disappeared.
BMI
No differences were observed in any variables when comparing patients with BMI below or above 25 kg/m2. However, insulin requirements in obese patients (n = 7; BMI ≥30kg/m2) were higher at the end of the study than in those with a BMI <30 kg/m2 (0.72 ± 0.47 UI/kg/day vs 0.54 ± 0.19 UI/kg/day; P < .01). Nevertheless, the basal/bolus distribution, diurnal/nocturnal basal rate, number of basal segments, HbA1c obtained at the end of the study, and decrease in HbA1c levels were similar in obese and nonobese subjects.
Discussion
One of the most important findings in the present study was the high percentage of basal insulin that patients were using at the end of the follow-up. In most publications, authors recommend a basal rate of 40% to 50% of TDD, but most of the published data came from pediatric population and in adults the basal requirements are higher. 10 In our patients, the basal rate increased from 50% at the beginning of CSII to approximately 61% when glucose control was improved. The existence of missed insulin boluses cannot be excluded, in spite of the fact that patients are instructed to measure postprandial glucose levels using the appropriate bolus correction. The distribution of insulin doses throughout the day depends on many factors, such as daily activities, weight, diabetes duration, age, insulin resistance, and diet.11 -13 A basal rate >50% is usually needed in patients with long diabetes duration, during the pubertal development, in patients with low physical activity, and in patients on a low carbohydrate diet. Patients included in the present study had a relatively long diabetes duration (>20 years), and although the amount of physical activity was not recorded, they were encouraged to keep the carbohydrate content of their diet at around 50% of total daily calories.
TDD at the beginning of CSII therapy is usually based on body weight or calculated by reducing insulin requirements in MDI regimen by 10% to 25%. 14 The final reduction needed in TDD in our patients was 18%. TDD was correlated with TDD used in MDI and also with diabetes duration, indicating the progressive decline in beta cell function. TDD was higher in males than in females independently of the body weight.
During follow-up, basal diurnal insulin decreased, and rates were comparable with previously published data (approximately 60/30%). 15 The number of basal segments per day was almost 5 at the end of the follow-up period, also in accordance with the literature. 16 The hourly basal rate was highest late in the evening and in the second half of the nocturnal period when insulin requirements are physiologically higher (dawn phenomenon). This dawn phenomenon was higher and lasted longer in males than in females. Some research has described circadian basal rate profiles in both adult and pediatric type 1 diabetic subjects, and more recently in type 2 diabetic pump users.17-19
In terms of metabolic control, at the end of follow-up HbA1c levels in our patients had decreased by 0.75% after CSII therapy. This reduction is higher than those observed in most series of patients and in a recent meta-analyses, which reported reductions around 0.5%. 2 The greater reduction of HbA1c levels observed in our population could be explained by the fact that subjects who didn’t improve metabolic control at follow-up were not included in the study. Patients who achieved better glycemic control were those initiating CSII for pregestational care. A higher frequency of visits and higher motivation may explain this difference. Higher number of basal segments per day was also associated with better glycemic control, probably because the insulin pattern was more adequately adjusted to the patients’ glycemic profile. Younger patients and those with lower diabetes duration also achieved lower HbA1c levels, in this case probably because the management of diabetes is usually less complicated at the first stages of the disease. 20 We also observed a negative relationship between diabetes duration and HbA1c levels achieved.
We found some interesting findings related to sex in the present study. Not only was TDD significantly higher in males than in females, but the proportion of basal rate was significantly lower. This finding has been previously reported in type 1 diabetic patients. 17 A possible explanation could be that diet in males had higher carbohydrate content.
Obese patients had higher insulin requirements than nonobese patients, but we did not detect any differences in insulin patterns. A correlation between body weight and insulin requirements has been previously described in type 1 diabetic subjects starting CSII immediately after the diagnosis, but not in a recent study of type 2 diabetic subjects after a short time CSII treatment.13,18
On the basis of these findings, we suggest the following: CSII should be started using higher doses of insulin per kg of body weight in males and obese patients; the basal rate of insulin should be at least 60% of TDD, especially in women and patients with longer diabetes duration; at least 3 basal segments per day should be used, administering higher doses of insulin in the evening and in the second half of the night; and this dose in the second part of the night should be higher in men.
Conclusions
In conclusion, characteristics such as sex, diabetes duration, and BMI may help clinicians establish TDD, basal/bolus distribution, and circadian basal rate profile more efficiently. Results from the present study support that the main predictors of glucose optimization in CSII therapy are high HbA1c levels before CSII, pregestational care as the indication for CSII, younger age, and the use of more basal segments.
Footnotes
Abbreviations
BMI, body mass index; CSII, continuous subcutaneous insulin infusion; MDI, multiple daily injections; TDD, total daily dose.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Research Grant from the Spanish Ministry of Health (FIS PI 080669).