
Abstract
Aims:
The goals were to analyze prescription patterns and the cost of antihyperglycemic drugs in patients with type 2 diabetes (T2DM) treated in Germany in 2015.
Methods:
This study included 36382 patients aged 40 years or over treated in general practices (GPs) and diabetologist practices who were diagnosed with T2DM in 2015. Nine different families of antihyperglycemic therapy were included in the analysis. Demographic data included age, gender, and type of health insurance coverage. Clinical data included HbA1c level, body mass index (BMI), and the number of T2DM complications. The annual antihyperglycemic treatment cost per patient was calculated based on pharmacy retail prices. The multivariate regression analysis was fitted to estimate the adjusted treatment cost differences.
Results:
The percentage of T2DM patients receiving antihyperglycemic treatments was 87.6. This share was slightly higher in men than in women (89.1% vs 86.0%). Interestingly, the share of people treated with antihyperglycemic drugs decreased with age yet increased with HbA1c levels, BMI, and the number of complications. The average annual cost of antihyperglycemic drugs amounted to €498. It was significantly higher in men than in women (difference of €22). It was also significantly higher in individuals with private health insurance coverage than in people with public health insurance coverage (difference of €153). The annual cost decreased with age. It is compelling to note that this cost increased with HbA1c levels and BMI. Finally, the annual cost also increased with the number of complications.
Conclusions:
The share and the cost of antihyperglycemic treatments vary with gender, age, type of health insurance coverage, HbA1c levels, BMI, and the number of complications.
Diabetes is a chronic disease which affects around 8.3% of the worldwide population.1,2 It is estimated that 1 in every 13 persons in Germany has diabetes. 3 Type 2 diabetes mellitus (T2DM) is found in 90% of individuals with diabetes. 4 The current annual German cost associated with T2DM of approximately €11.8 billion in 2010 will exceed €21 billion in 2040, underscoring the major burden of diabetes in this country. 5
Reduction of blood glucose levels in T2DM patients is important since it can prevent microvascular and macrovascular complications.6-8 If these levels remain high despite the introduction of lifestyle measures such as weight control and physical activity, oral antihyperglycemic medications and insulin treatments can be used in people with T2DM. Several studies have targeted the prescription of antihyperglycemic drugs and the cost of these medications in Germany.9-10 In 2007, Rathmann and colleagues discovered that there had been a 100% increase in the average cost for antidiabetic medication between 1994 (€86.7) and 2004 (€172.1). 9 More recently, Tamayo et al further found regional and individual social disparities in the cost of overall and newer antihyperglycemic medications unexplained by other confounders. 10 Although these works have shed light on medical and economic aspects of the treatment of T2DM in Germany in the past decades, they may be obsolete and may not reflect the status of current antihyperglycemics prescriptions in this country.
Consequently, the goal of the present study was to analyze prescription patterns and the cost of antihyperglycemic drugs in T2DM patients treated in German general and diabetologist practices in 2015.
Methods
Database
The Disease Analyzer database (IMS HEALTH) compiles drug prescription, diagnosis, basic medical, and demographic data obtained directly and in anonymous format from computer systems used in the practices of general practitioners. Diagnoses (ICD-10), prescriptions (Anatomical Therapeutic Chemical [ATC] Classification System), and the quality of reported data have been monitored by IMS based on a number of criteria (eg, completeness of documentation, linkage between diagnoses and prescriptions).
In Germany, the sampling methods used for the selection of physicians’ practices were appropriate to obtain a representative database of primary care practices. 11 Prescription statistics for several drugs were very similar to data available from pharmaceutical prescription reports. 12 The age groups for given diagnoses in Disease Analyzer also agreed well with those in corresponding disease registries. 11
Finally, this database has already been used in several studies focusing on diabetes.2,12-14
Study Population
The present study included 36382 patients aged 40 years or over with a T2DM diagnosis in 2015. In all, 29779 patients were treated by GPs and 6603 by diabetologists. Nine different families of antihyperglycemic therapy were included in the analysis: human insulins and analogues (ATC: A10C), sulphonylureas (A10H), biguanides (A10J), glitazones (A10K), alpha-glucosidase inhibitors (A10L), glinides (A10M), dipeptidyl peptidase-4 (DPP-4) inhibitors (A10N), sodium-glucose cotransporter 2 (SGLT-2) inhibitors (A10P), and glucagon-like peptide 1 (GLP-1) agonists (A10S). Demographic data included age, gender, and type of health insurance coverage (public or private). Clinical data included HbA1c levels, body mass index (BMI), and the number of T2DM complications, which comprised coronary heart disease (CHD, ICD 10: I24-25), myocardial infarction (I21-23), stroke/transient ischemic attack (I63-64, G45), peripheral arterial disease (PAD, I73.9, E11.5), polyneuropathy (E11.4), retinopathy (E11.3), and renal complication (N18-19, E11.2). BMI and HBA1c were estimated based on the last documented value in 2014.
Statistical Analyses
The study sample was stratified by age, gender, type of health insurance coverage, HBA1c levels, BMI, and the number of T2DM complications. The share of patients who received antihyperglycemic treatments was further estimated. The annual antihyperglycemic treatment cost per patient was calculated based on pharmacy retail prices. The multivariate regression analysis was fitted with the annual antihyperglycemic medication cost as dependent variable, and age, gender, type of health insurance coverage, HBA1c levels, BMI, and number of complications were used as predictor variables to estimate the adjusted treatment cost differences. An additional regression model included antihyperglycemic drug classes as dependent variables to estimate the cost changes depending on the therapy received. Analyses were carried out using SAS version 9.3.
Results
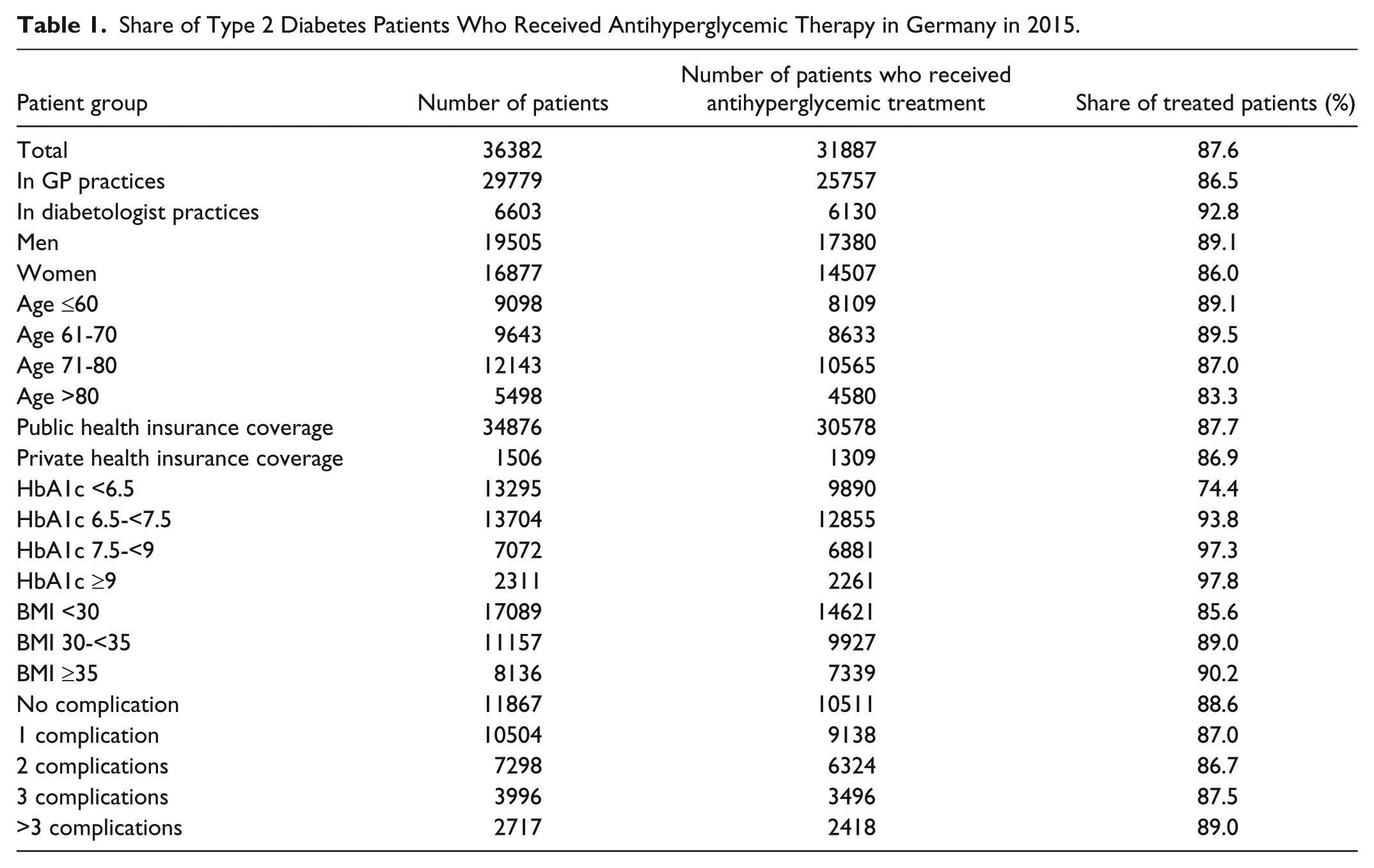
In 2015, 87.6% of T2DM patients received antihyperglycemic treatments (Table 1). This share was slightly higher in men than in women (89.1% vs 86.0%). It is interesting to note that the share of people who received antihyperglycemic drugs decreased with age (≤60 years: 89.1% vs >80 years: 83.3%) yet increased with HbA1c levels (<6.5%: 74.4% vs ≥9%: 97.8%), BMI (<30: 85.6% vs ≥35: 90.2%), and the number of complications (0: 88.6% vs >3: >89.0%). Table 2 displays the average cost of antihyperglycemic medications per patient in 2015 and the results of the regression model. This cost amounted to €498 (SD €590) for the overall population. It was significantly higher in men than in women (adjusted difference of €22). It was also significantly higher in individuals with private health insurance coverage than in people with public health insurance coverage (adjusted difference of €153). The annual cost decreased with age, from €548 in patients aged 60 years or younger to €388 in patients aged over 80 years (adjusted difference of €168). Interestingly, the cost increased with HbA1c levels and BMI (HbA1c<6.5% vs HbA1c ≥9%: adjusted difference €502; BMI <30 vs BMI ≥35: adjusted difference €228). The annual cost also increased with the number of complications, from €389 when there was no complication to €753 when there were more than 3 complications (adjusted difference of €365). Finally, therapy with metformin or sulfonylurea was associated with lower annual medication costs since DPP-4, GLP-1, SGLT-2 and insulin were linked with increasing costs (Table 3).
Share of Type 2 Diabetes Patients Who Received Antihyperglycemic Therapy in Germany in 2015.
Annual Antihyperglycemic Treatment Cost per Patient in 2015.
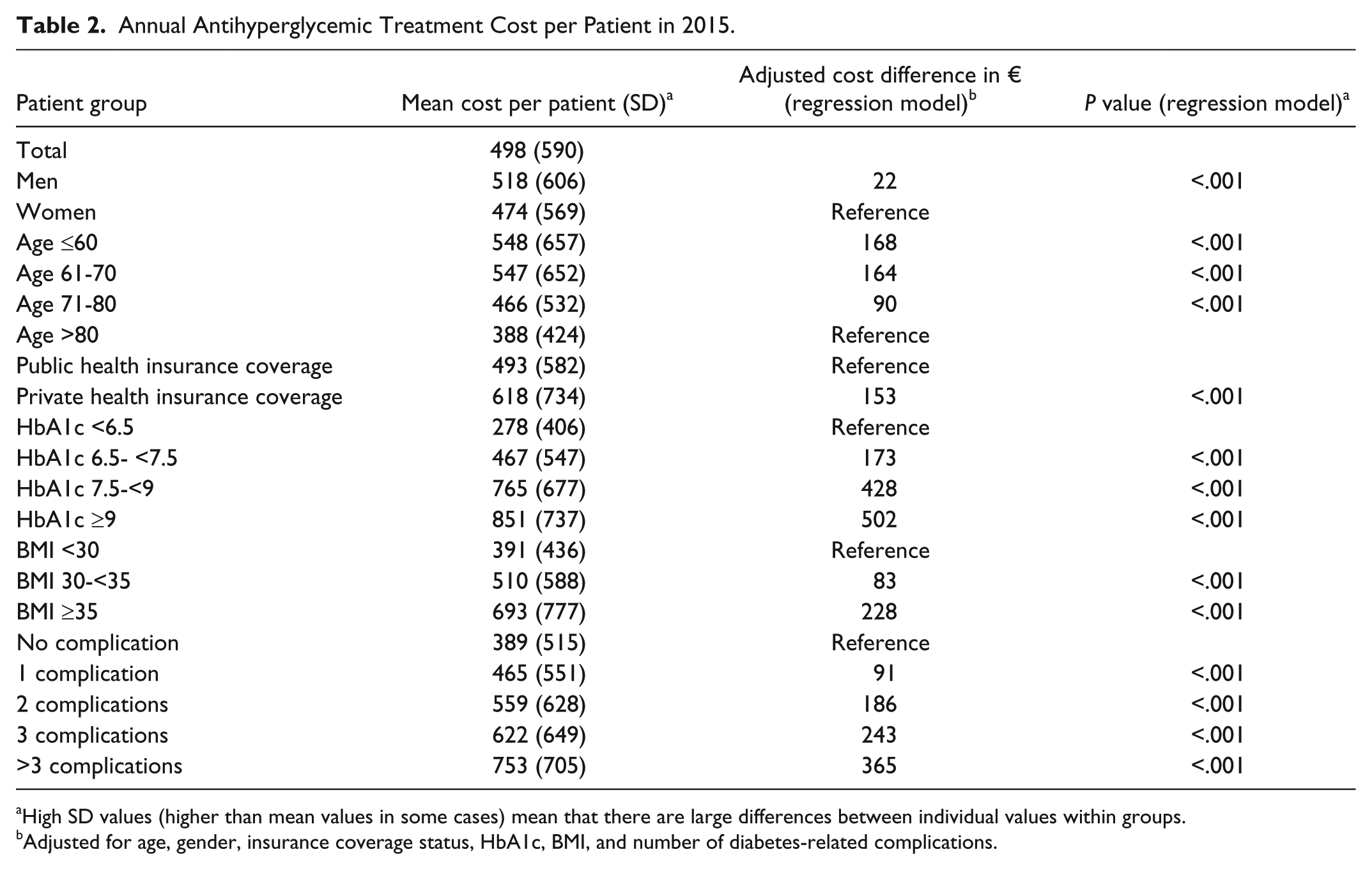
High SD values (higher than mean values in some cases) mean that there are large differences between individual values within groups.
Adjusted for age, gender, insurance coverage status, HbA1c, BMI, and number of diabetes-related complications.
Annual Antihyperglycemic Treatment Cost per Patient Depending on Therapy Class in 2015.
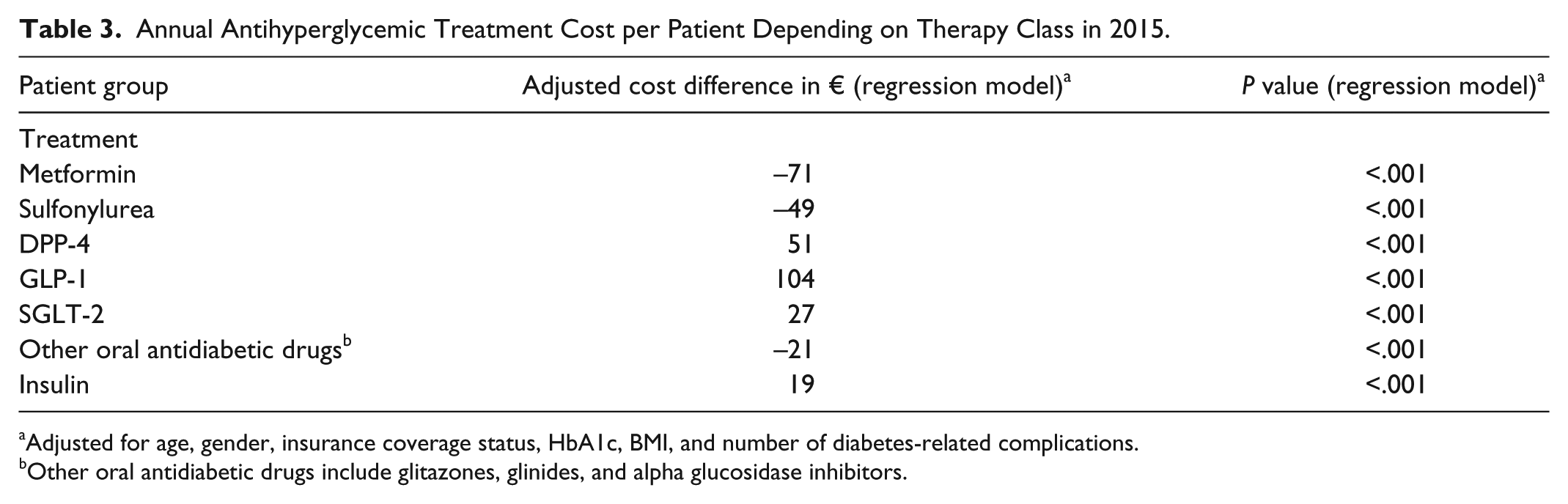
Adjusted for age, gender, insurance coverage status, HbA1c, BMI, and number of diabetes-related complications.
Other oral antidiabetic drugs include glitazones, glinides, and alpha glucosidase inhibitors.
Discussion
The present retrospective study showed that the share and the cost of antihyperglycemic treatments were higher in men than in women. Notably, the cost of such drugs was also higher in individuals with private health insurance coverage than in individuals with public health insurance coverage, although the proportion of patients who received antidiabetics was nearly identical between the 2 groups. Finally, both the share and the cost of antihyperglycemic medications decreased with age and increased with HbA1c levels, BMI, and the number of complications.
Prescription patterns and the cost of antidiabetic medications in Europe have been the focus of several studies. In 2006, a study conducted by Melander and colleagues in 10 European countries, including Germany, revealed that the use of metformin and other antihyperglycemic drugs had increased since the 1990s, reflecting the growing prevalence of T2DM in this area of the world. 15 However, there were large differences in prescription patterns, suggesting that the screening and the management of T2DM varied between countries. The evolution of these patterns was of particular interest in Germany and was characterized by an increase in the use of insulin and metformin as well as a decrease in the utilization of sulfonylureas. 15 In Germany, there is also 1 more source presenting yearly therapy costs. 16 Although each antihyperglycemic class is presented in this book, no direct comparison with the present work is possible due to differences in the cost estimation methods used in each text. 16
It was subsequently discovered in Germany that new oral antidiabetic drugs were prescribed to 17.6% of patients with T2DM treated in GPs/diabetologists in 2014 and that the associated cost was €144.6. 2 By contrast, previous oral antidiabetic drugs, which were prescribed to more than 44% of patients, had a cost of only €45.6 per individual. 2 With the exception of sulfonylureas, the other antidiabetic medications are much more costly than metformin and sulfonylurea. Thus, it is logical that in the present study, therapy with newer antidiabetic drugs (ie, DPP-4 inhibitors, glinides or GLP-1 agonists) is associated with higher yearly medication costs among those suffering from diabetes. It can explain 2 other important findings of the present work. In point of fact, it was demonstrated that this cost increased with HbA1c levels and BMI. Since high concentrations of glycated hemoglobin indirectly reflect poor glycemic control, individuals with high HbA1c levels are more likely to receive multiple antihyperglycemic drugs compared to individuals with low levels of HbA1c who may receive only 1 drug. Another explanation is that patients with high HbA1c values switch from metformin to second-line treatments which are more expensive. 17 In the case of BMI, one must consider that GLP-1 agonists, which have a positive impact on weight loss, are often given to patients who exhibit both T2DM and obesity, 18 emphasizing the fact that the cost of antihyperglycemic treatments increased with BMI in this work. It was also found that the cost of these drugs was higher in individuals with private health insurance coverage than in patients with public health insurance coverage, indicating that the first group has a higher chance of receiving DPP-4 inhibitors or GLP-1 agonists than the second group. 19 Finally, the total cost of antihyperglycemic treatments was lower in this work (€498) than in a study conducted in 2010 (€633). 20 This slight discrepancy between the findings of the 2 studies may be due to annual variations in the cost of antihyperglycemic drugs in Germany but may also be due to the difference in study methods.
As the relatively high costs of new antidiabetic therapies have already been discussed, the efficacy of these treatments should also be mentioned. Several studies have demonstrated that the use of DPP-4 inhibitors, 21 GLP-1 receptor agonists, 21 and SGLT2 inhibitors 22 is associated with consequent decreases in HbA1c levels. In addition, the use of GLP-1 receptor agonists leads to weight loss. 21
Retrospective primary care database analyses are generally limited by the validity and completeness of the data on which they are based. The present study included several limitations, which should be mentioned. First, no valid information was provided on diabetes duration. In addition, the assessment of complications and comorbidity relied solely on ICD codes entered by primary care physicians. Data on socioeconomic status (eg, education, income) and lifestyle-related risk factors (eg, smoking, alcohol, physical activity) were also lacking. Unfortunately, the documentation of hypoglycemia was also insufficient and could not be used, although hypoglycemia may have an impact on antihyperglycemic treatments. Therapy costs were estimated based on the sum of pharmacy retail prices, which can differ significantly from the actual reimbursed prices due to contracts between statutory sickness funds and manufacturers, resulting in lower costs. Finally, the cost associated with the management of diabetes complications was not analyzed. The main strengths of this work are the number of patients and the various families of antidiabetic drugs considered for analysis.
In conclusion, the findings of this German study suggest that the share and the cost of antihyperglycemic treatments vary with gender, age, type of health insurance coverage, HbA1c levels, BMI, and the number of complications. Further analyses are needed to gain a better understanding of the share and the cost of each family of antidiabetic drugs.
Footnotes
Abbreviations
ATC, Anatomical Therapeutic Chemical Classification System; BMI, body mass index; CHD, coronary heart disease; DPP4i, dipeptidyl peptidase-4 inhibitors; GLP-1, glucagon-like Peptid 1; GP, general practitioner; HbA1c, hemoglobin A1c; ICD, International Classification of Diseases; PAD, peripheral arterial disease; SD, standard deviation; SGLT-2, sodium dependent glucose transporter; T2DM, type 2 diabetes mellitus.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.