
Abstract
Aim:
The aim was to review studies examining the effectiveness, acceptability, and feasibility of mobile-based technology for promoting active lifestyles in people with type 2 diabetes (T2D).
Background:
Benefits of leading an active lifestyle following a diagnosis of T2D, including improved glycemic control, have been reported. Studies examining the specific use of mobile-based technologies to promote an active lifestyle in T2D have not previously been reviewed.
Methods:
Research studies examining effectiveness, feasibility or acceptability of mobile-based technology for active lifestyle promotion for T2D management were included (n = 9). The databases searched included PubMed, Medline, ScienceDirect, and ACM Digital Library (January 2005 to October 2015). Studies were categorized as (1) informing, (2) monitoring, (3) provoking, or (4) sustaining behavior change.
Results:
Technologies used included smartphone or tablet apps, diabetes personal digital assistant, continuous glucose monitor and accelerometer, pedometer, and a website delivered by a smartphone. No articles examined the effectiveness of mobile-based technology in monitoring health behaviors and behavior change. Four of the studies found mobile-based technology to be motivational and supportive for behavior change. The visual reinforcement was identified as motivational. The feasibility and acceptability of using mobile-based technology to provide sustained lifestyle change and the effectiveness of mobile-based technology in monitoring health behaviors and behavior change have not been investigated. No studies examined all 3 of the outcomes or focused decreasing the participants’ sedentary behavior.
Conclusions:
Limited research has examined the feasibility, acceptability, and effectiveness of mobile-based technology to promote active lifestyles and subsequently good diabetes management in people with T2D.
Several studies have reported the substantial benefits of leading an active lifestyle following a diagnosis of type 2 diabetes.1-3 Research has reported significant improvements in glycemic control in addition to numerous other physical, mental and social health benefits.1-3 More recently, reduced sedentary time has also been shown to be effective in the lowering of blood glucose levels irrespective of physical activity levels in obese nondiabetic adults. 4 Sedentary behavior has been defined by the Sedentary Behaviour Research Network 5 as any waking activity in a sitting or reclining position with an energy expenditure of ≤1.5 metabolic equivalents. This is important as high levels of sedentary behavior may negate acceptable levels of physical activity. 6 Thus current guidelines for an active lifestyle include recommended levels of both physical activity and sedentary time. 7
A systematic review and meta-analysis of 17 studies examining the effect of physical activity interventions on glycemic control in people with type 2 diabetes was conducted by Avery and colleagues. 1 Behavioral interventions were shown to significantly increase objective and subjectively measured physical activity, in addition to clinically significant improvements in HbA1c levels. 1 While this review demonstrates the potential for behavioral interventions to have a positive impact on glycemic control in the context of physical activity however; most interventions are delivered face to face which limits the opportunity for widespread implementation.
Technology is becoming increasingly a part of people’s everyday lives, in particular mobile-based technology. It is estimated that almost 2 billion people in the world own a smartphone giving them instant access to a variety of technology applications. 8 Mobile applications have been developed as an aid to improve almost every aspect of life, such as activity levels, diet and sleep patterns. Technology, such as computer programs and wearable devices, is similarly being used more as a means of monitoring and managing conditions like diabetes. Studies have examined the use of a variety of technologies as a method of increasing physical activity in those with type 2 diabetes, such as telephone counseling 9 and personal data assistant-based self-monitoring. 10 Given the global increasing prevalence of diabetes technology offers a means of delivering interventions on a much larger scale and could potentially have a significant impact on diabetes management.
To gain knowledge and understanding of the topic area and the research conducted thus far, an integrative literature review approach was adopted. The integrated method has a systematic approach consisting of 5 stages: (1) problem formulation, (2) literature search, (3) evaluation of data, (4) data analysis, and (5) interpretation and presentation of results. This method allows for the inclusion of both empirical and theoretical literature, meaning the literature used is not restricted to a specific study design, such as randomized control studies. 11 This allows for an increased number of studies to be included in the review and a combination of diverse study methodologies to be examined 12 to give a more thorough understanding of the research conducted so far.
Methods
Aims
This systematic, integrated literature review aimed to identify the mobile-based technologies that have been used in previous studies to promote active living in those with type 2 diabetes. The review focused on research examining the effectiveness, feasibility and acceptability of these technologies to identify gaps in the research and directions for future work.
Design
The integrated review was conducted using a modified methodological framework developed by Whittemore and Knafl. 11 This methodology has been successfully used in previous reviews in related areas, such as nursing. 13 The framework focused on 5 key phases: problem identification, literature search, data evaluation, data analysis, and presentation of the findings. 11
In addition, the research articles identified were categorized based on the objective/function of the mobile-based technology; this systematic presentation of the current evidence was used to illustrate specific gaps. The categories used were as follows: (1) inform—mobile-based technology used to provide health information to participants; (2) monitor—mobile-based technology used to monitor health behaviors and behavior change; (3) provoke—mobile-based technology used to initiate behavior change (over a period of less than 6 months); or (4) sustain—mobile-based technology used to support maintenance of behavior change (over a period of 6 months or longer).
Inclusion and Exclusion Criteria
The inclusion and exclusion criteria for the literature search was developed using the PICOS framework for systematic reviews and is illustrated in Table 1.
PICOS Framework.
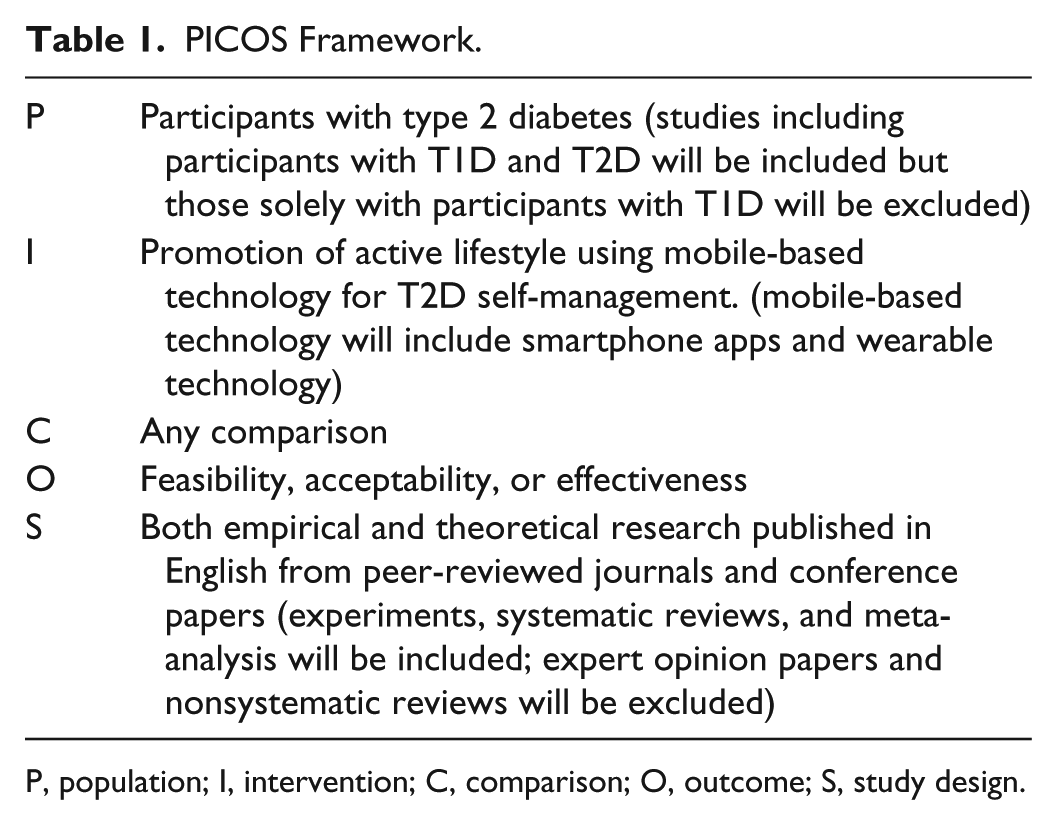
P, population; I, intervention; C, comparison; O, outcome; S, study design.
Search strategy
The following electronic databases were searched: PubMed, Medline, ScienceDirect, and ACM Digital Library. A total of 13 keywords and phrases were used in the literature search. These were mobile-based, technology, active living, physical activity, sedentary behavior, sitting time/bouts/periods, lifestyle change, type 2 diabetes, blood glucose control/management, glycemic control, effective, feasible, acceptable. Reference lists were also reviewed to identify articles not found in the database search.
Search Outcome
Figure 1 illustrates the stages of the literature search. A total of 7662 articles were identified in the initial search of the online databases. Following the implementation of the inclusion criteria to the titles, 72 articles remained. The abstracts of the remaining articles were evaluated, leaving 13 studies. A total of 4 articles were removed following an evaluation of the full texts using the inclusion criteria, leaving 9 articles identified as suitable for review. To ensure that the most relevant articles were included in the review and to reduce author bias, the first author reviewed the titles, abstracts and full articles using the inclusion criteria and the selected articles were crosschecked and agreed on by the second and third authors.
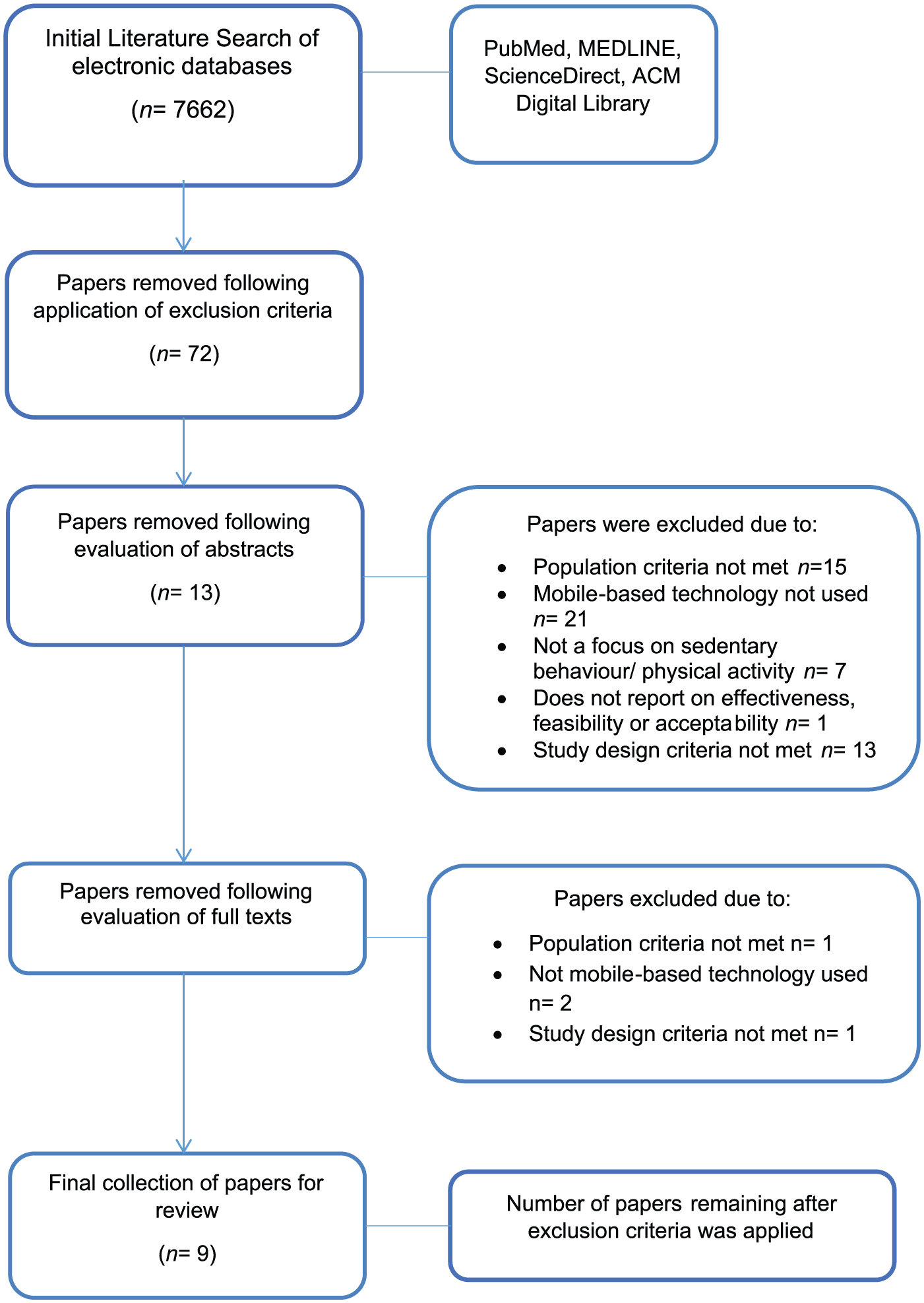
Literature search exclusion chart.
Data Extraction
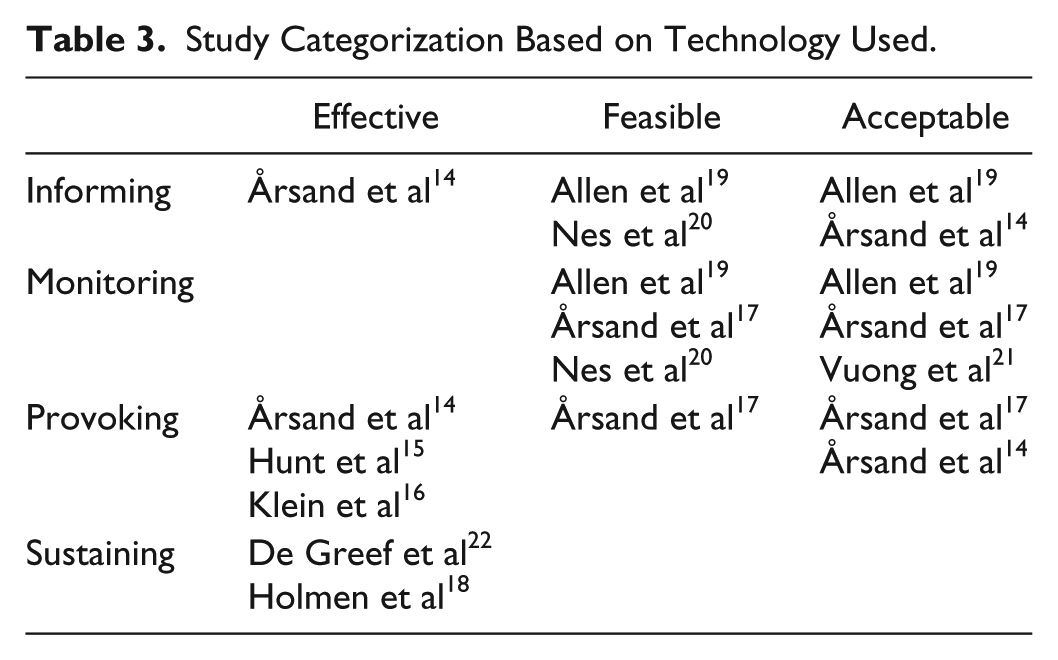
Each article was reviewed and information extracted including study design, sample size, mean age and HbA1c of participants, measurement of diabetes self-management, technology used, outcome measured (effectiveness, feasibility, acceptability), and key study findings. This information is presented in Table 2. Articles were further collated and categorized into technologies that (1) inform, (2) monitor, (3) provoke, or (4) sustain behavior change. This information is presented in Table 3.
A Summary of Research Studies Included in the Review.
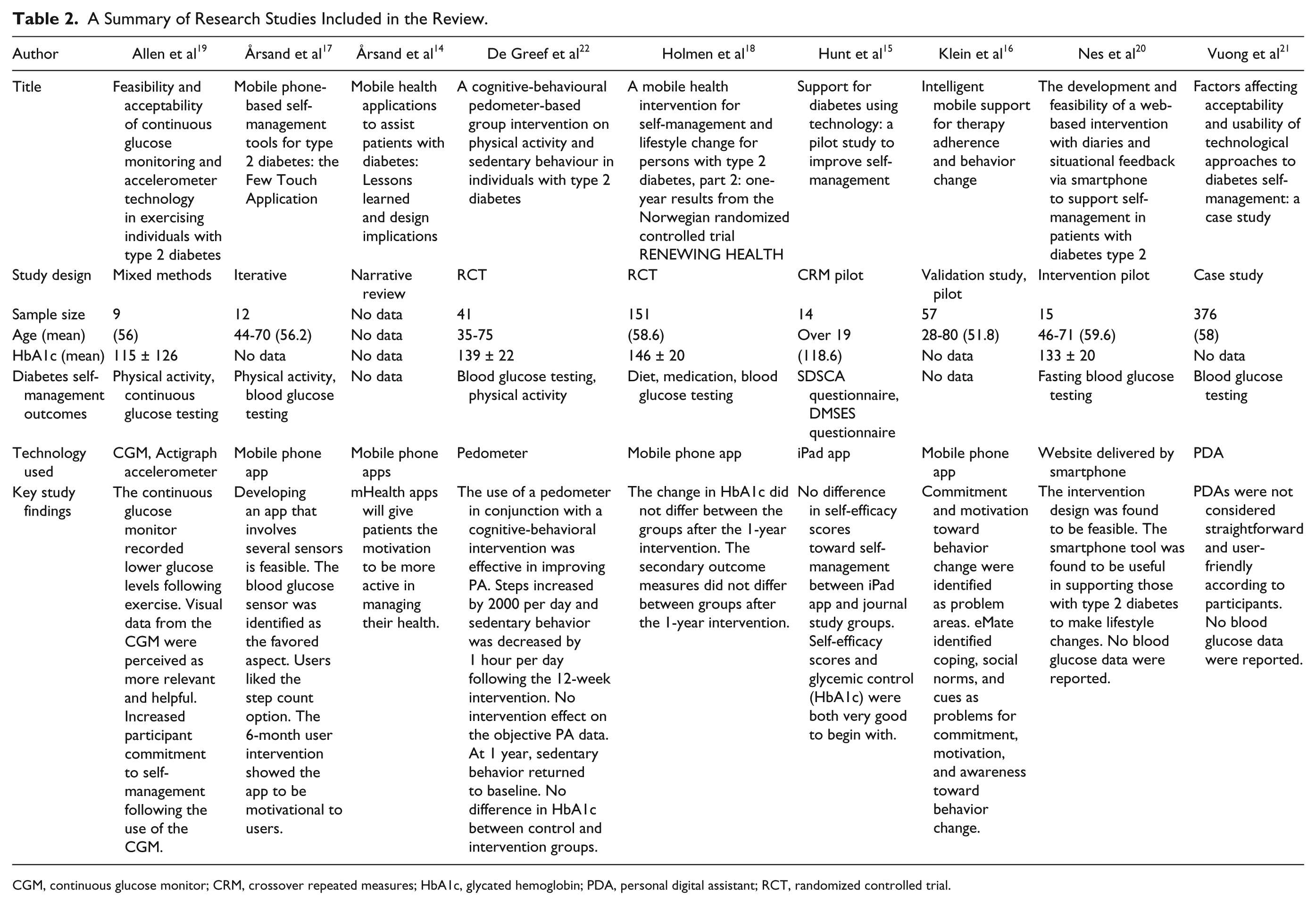
CGM, continuous glucose monitor; CRM, crossover repeated measures; HbA1c, glycated hemoglobin; PDA, personal digital assistant; RCT, randomized controlled trial.
Study Categorization Based on Technology Used.
Quality Assessment
There is no gold standard for assessing quality in an integrated review. 11 Quality assessment was conducted using an adapted tool developed by Guo et al, 13 and the results are presented in Table 4.
Study Quality Assessment.
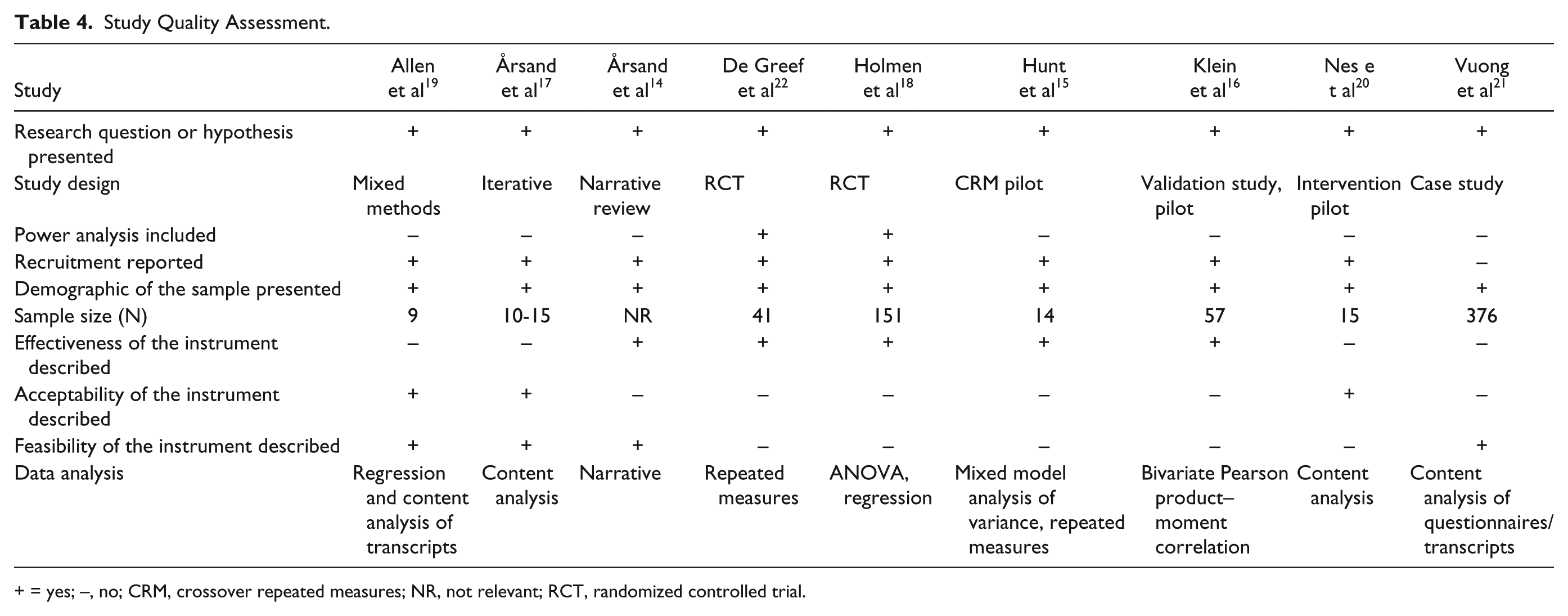
+ = yes; –, no; CRM, crossover repeated measures; NR, not relevant; RCT, randomized controlled trial.
Results
A total of 9 articles were identified as suitable for review. Table 2 shows a summary of the information extracted from the articles. Of the 9 articles, 5 studies used smartphone or tablet apps, 1 used a diabetes personal digital assistant (PDA), 1 used a combination of continuous glucose monitor and accelerometer, 1 used a pedometer, and 1 used a website delivered by a smartphone. All studies were focused on those with type 2 diabetes and samples size ranged from 9 to 376 participants. Methods used to measure self-management included diet, physical activity, blood glucose testing, the Summary of Diabetes Self-Care Awareness (SDSCA) questionnaire and the Diabetes Management Self-Efficacy Scale (DMSES) questionnaire. The effectiveness of the technology was assessed in 6 studies while feasibility was examined in 3 of the studies. The acceptability of technology was examined in 4 studies and 3 studies examined more than 1 of these variables.
From the studies which used mobile phone or iPad apps, a variety of study designs were used and outcome variables measured. Three studies examined the effectiveness of mobile phone or iPad apps to provoke behavior change.14-16 Klein et al 16 conducted a pilot study and developed an app for those with chronic illness, including those with type 2 diabetes, based on behavior change theories. Similarly, Hunt et al 15 conducted a pilot study examining the participant’s self-efficacy toward self-management and found no statistically significant difference in outcome variables between the group who were asked to complete journals first and the group using the iPad app first. Authors acknowledged self-efficacy scores were high at baseline and mean HbA1c for the whole sample was 6.5%, which indicates good glycemic control, leaving little room for improvement. The study conducted by Årsand et al 14 differed slightly as it was a review of previous studies examining the effectiveness of mobile phone apps to assist diabetes patients. Årsand et al 14 concluded that mobile phone apps increase motivation in those with diabetes to manage their health. The remaining 2 studies that used mobile phone apps were conducted by Årsand et al, 17 who used an iterative approach to develop an app focused on self-management tools for those with type 2 diabetes and Holmen et al 18 who reported on the 1-year follow up results of a randomized controlled trial. From user feedback from a 6-month intervention through focus groups and interviews it was concluded that the app designed by Årsand et al 17 had resulted in some participants changing their medication and physical activity habits and the app had a motivational effect on those who had used it. Holmen et al 18 found that those ≥63 years used the app more than the younger participants (P = .045) but there was no significant difference in HbA1c levels between the control group and the intervention groups after 1 year. Although all studies here used an app, it is difficult to compare results as the apps developed and the outcome measures included were different across the studies.
Allen et al, 19 Nes et al, 20 and Vuong et al 21 all used technology that is categorized as monitoring in their studies. Allen et al 19 used a combination of continuous glucose monitoring and an accelerometer to examine whether the combined visual feedback from the devices would motivate participants to change their behavior. The data from the glucose monitor and accelerometer showed moderate intensity physical activity lowered glucose levels by a mean of 63 (SD = 38) mg/dl (range = 0-160 mg/dl) within 5 hours (range = 0-12 hours); however it was not reported whether these findings were statistically significant. Results from the focus groups found participants felt the visual feedback from the devices increased their commitment to using physical activity for self-management. Nes et al 20 conducted a pilot intervention using a website delivered through a smartphone. Authors reported the intervention design to be feasible and most participants reported positive lifestyle changes and found the smartphone tool useful and supportive toward self-management. Vuong et al 21 examined factors which impact on acceptability and usability of technology in diabetes management using a PDA. Participants felt the PDAs were difficult and complicated to use and were not user-friendly. Vuong et al 21 concluded that it is important to take individual perception into consideration and not develop a one-size-fits-all approach to using technology. In addition, using more popular devices, such as smartphones, would improve acceptability.
The final study included in this review was a randomized controlled trial examining the effectiveness of a cognitive behavior and pedometer intervention at sustained behavior change in those with type 2 diabetes. 22 After the 12-week intervention, the intervention groups daily steps increased by 2000 more than the control group (P < .05), however, after a year, steps per day in the intervention group had decreased significantly (P < .01) showing the intervention was successful at increasing physical activity in the short term but not long term. Similar results were described for time spent inactive per day. The intervention group significantly reduced inactivity in the 12 weeks (P < .05) but returned to baseline levels by 1 year.
Gaps in the literature are identified in Table 3. Of the studies reviewed, none of the articles examined the effectiveness of mobile-based technology in monitoring health behaviors and behavior change. Similarly, the feasibility and acceptability of using mobile-based technology to provide sustained lifestyle change has not been investigated. Most of the research (n = 5) focused on the effectiveness of using mobile-based technology to provoke lifestyle change.
Table 4 presents the results of the quality assessment of articles using an adapted tool developed by Guo et al. 13 All 9 studies presented a research question or hypothesis. Recruitment, demographics and sample size, where relevant, were reported in all 9 studies. Power analysis was included for the 2 randomized controlled trials.18,22 Five articles investigated effectiveness,14-16,18,22 3 examined the acceptability,17,19,20 and 3 examined the feasibility.14,17,19 A range of study designs and data analysis methods were included in this review.
Discussion
The main purpose of this systematic, integrated literature review was to examine published research for the use of mobile-based technology to promote active lifestyles in those with type 2 diabetes. The integrated framework allowed for a broad range of study design and methods to be included in the review, including quantitative and qualitative research. However, a total of only 9 articles met the inclusion criteria for the review highlighting the need for more research to focus on this topic.
The 2 areas where most research has been conducted are the feasibility and acceptability of mobile-based technology when used to monitor behavior.17,19-21 To achieve sustained behavior change, it is important to address the acceptability and feasibility of using technology to promote active living. Some studies have addressed this and the successful aspects from these studies could be used to inform a more effective and sustainable intervention to promote active living in the future. The overall limitations of the current literature, however, is the failure to examine the effectiveness, acceptability and feasibility of mobile-based technology together, as part of 1 study.
All the research that was included in this review focused on 1 or 2 of the outcome measures, none of the studies looked at the effectiveness, feasibility and acceptability of the mobile-based technology across all the categories. This is important to acknowledge as by not considering all 3 outcomes simultaneously in research design, fails to address the question as to whether the technology and methods used to enhance active living would really be suitable or successful.
Identified Gaps in the Literature
We have illustrated 3 key gaps in the current literature: None of the articles included in this review explored the effectiveness of using mobile-based technology to monitor physical activity or sedentary behavior and better diabetes management. Similarly, none of the research thus far has examined how feasible or acceptable it would be to use mobile-based technology to promote sustained behavior change. This is the most important gap in the current research as prolonged, sustained behavior change is the ideal outcome. To achieve this outcome, it is important to fully understand how mobile-based technology can be used in this area. None of the research has been conducted to specifically examine the use of technology when trying to change a person’s sedentary behavior. As aforementioned, it is important to examine physical activity and sedentary behavior as 2 individual constructs as they are not influenced by the same variables and different methods may be required to change these behaviors. 8
This is particularly important when promoting sustained behavior change as the technology may be effective in changing participant behavior during an intervention but if it is not acceptable in terms of design, usability or cost to the individual, further use of the technology will not be sustained with the risk of reversion to a less active lifestyle.
Limitations of the Review
The main limitation of this review is that an adapted version of a quality assessment was completed rather than a validated quality assessment. The Cochrane Collaboration’s risk of bias tool and the Effective Public Health Practice Project’s quality assessment tool for quantitative studies were considered but ruled out as they were only suitable for quality assessment in intervention studies. Furthermore, a method developed by Nowlin and colleagues 23 was considered as an appropriate form of quality assessment as it does not measure quality based on study design but rather whether the study fulfils expectations. It was decided, however, that this method was too subjective to be used in the current review. This is due to the different study designs and there not being a suitable quality assessment tool available. This has been addressed in Table 4, where the data are presented in the context of the review research question and the main study outcomes allowing the reader to judge the quality of the articles reviewed. Furthermore, the integrated methodology of the review allowed for a broad range of research to be included, and this could be seen as a limitation as the varying study designs, technology used, and outcomes measured made it difficult to compare studies.
Future Research Recommendations
Mobile-based technologies are increasingly being used for health monitoring and health improvement. Future interventions should be informed by research that has examined all 3 variables to identify the most effective, feasible and acceptable mobile-technology methods in promoting and sustaining active lifestyles in those with type 2 diabetes. From the research in this review it is clear that technology should be tailored to the individual using it 21 and ideally include visual feedback of glucose and activity data to increase motivation toward self-management in those with type 2 diabetes. 19 The integration of behavior change theories within mobile-based technologies may prove more effective in promoting active lifestyles than mobile-based technology alone. 20
Conclusion
Limited research has examined the feasibility, acceptability and effectiveness of mobile-based technology to promote active lifestyles and consequently good diabetes management in people with type 2 diabetes. Future research should examine the most effective, feasible, and acceptable mobile-technology methods in promoting sustained active lifestyles in those with type 2 diabetes.
Footnotes
Abbreviations
CGM, continuous glucose monitor; CRM, crossover repeated measures; DMSES, Diabetes Management Self-Efficacy Scale; HbA1c, glycated hemoglobin; PDA, personal digital assistant; RCT, randomized controlled trial; SDSCA, Summary of Diabetes Self-Care Awareness.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PhD project was funded through a contribution from PAL Technologies and the Partnership Contribution Fund, which is a joint fund created by Capita IT Enterprise Services and the University of Strathclyde to provide education and employment benefits to students and graduates.