
Abstract
The health care industry is undergoing a major transformation. Despite spending more on health care than any other country, the United States has not seen a commensurate improvement in the quality of care. Chronic disease management puts the greatest burden on the health care system with estimates suggesting that 3 of 4 health care dollars are spent on managing chronic disease. Moreover, the number of older patients with chronic conditions, like diabetes, is rising as expected, which only serves to worsen the physician shortage problem we are currently experiencing, and further increase health care costs. Unless new models of health care are established for these patients, they simply will not be served. Consistent with the message above, there are generally 3 universal health care needs, (1) improved outcomes, (2) expanded access, and (3) optimized cost and efficiency. It is likely the future state will involve value-based health care, with payment based on outcomes, not services rendered, and incentives tied more directly to the value delivered. Medical device providers will be held more accountable for positive outcomes, and to ensure success, they will need to create better solutions with their therapies. Instead of the touch point with patients being solely at the time of a procedure or sale of the device, it is likely companies will need to drive toward a more comprehensive partnership with patients, providers, and payers, extending the scope of services and interactions to provide a continuum of care. In general, companies will need to start to think of their most important customers as people living with a condition, as opposed to patients needing immediate medical devices. In this article, I discuss the challenges of health care today and present some of the opportunities to revamp health care delivery in diabetes by leveraging the pervasive use of mobile technologies and digital data.
Health care costs continue to rise at rates outpacing increases in the GDP, such that health care expenditures will go from 18% of the GDP in 2010 to a projected 20% in 2021 and 26% in 2035, due in part to an aging US population and emergence of costly new technologies and treatments to extend life. 1 This trajectory is not sustainable, and many experts believe the health care industry needs to reinvent itself to ease this burden. Beyond reducing administrative waste in the system, remote monitoring and the appropriate use of “big data” hold the promise of changing the way health care is delivered to provide more effective, cost-saving solutions. 2 The ultimate goal is to enable personalized and patient-centered care, where treatments are tuned to match the patient’s individual needs. To accomplish this task, a holistic view of the patient, which aggregates and interprets all the relevant information that impacts patient care must be considered—whether that information comes from a medical device, hospital or physician electronic medical record (EMR), health/wellness device, or physician- and patient-entered notes. This holistic view of the patient can be correlated with population information and other analytics to provide insights and therapy recommendations based on an assessment of previously collected data from similar patients. Ideally, ongoing management can transition out of the physician’s office and into the person’s home, office or wherever they may be. When interventions are required, physicians have all the information they need to provide the next level of care.
Certainly, this utopia is not easily obtainable, and many changes to the health care system need to accompany this effort, including legislative reforms, data standardization guidances, privacy laws, reimbursement, and incentive schemes. However, there are small steps toward this goal being made every day. Many companies are now leveraging mobile health initiatives to take the ongoing care and therapy management of people to their homes. Companies are striving to monitor a person’s well-being on a day-to-day basis, improve their adherence to therapy, and provide modifications to therapy on an exception basis, when the patient’s health status begins to deteriorate, but prior to a more costly event. The common theme of these programs is to reduce expensive health care interventions by avoidance. Also, routine interactions are moving from the doctor’s office to the person’s home. This certainly eases the burden of both the patient and provider, as these interactions can often be automated, and/or streamlined based on key insights from comprehensive data.
Several groups have started leveraging home care solutions. For example, the Scripps Translational Science Institute Wired for Health Study is evaluating whether the integration of wireless technologies and online social networks can have a beneficial impact on health care spending and outcomes. The initiative is focused on many chronic conditions, including diabetes, where active remote monitoring using the iBGStar BG meter and Qualcomm Life’s 2net Hub will allow ongoing patient care and support. 3 DexCom has recently gained FDA approval for the Share™, which transmits continuous glucose monitoring (CGM) data to the cloud and provides a real-time notification system for up to 5 people, and Medtronic also gained approval for the MiniMed© Connect, which provides similar functionality. WellDoc has developed BlueStar®, an integrated system for type 2 diabetes management and support that is an FDA-approved app that physicians can prescribe to their patients. The WellDoc platform was evaluated in a clinical trial which demonstrated improved outcomes with a statistically significant reduction in HbA1c. 4 TelCare has a cellular enabled BG meter which sends personalized messages to patients immediately following each BG test. Lower health care expenditures were reported when using their system. 5 Tidepool is developing a cloud-based platform to aggregate diabetes device data in real-time and make the data available to patients and providers. They will then provide programming interfaces to developers so they might create tools to simplify and ease the burden of diabetes management. 6 Glooko has developed tools to aggregate health and wellness data with diabetes device data. 7 Glooko is partnering with the Joslin Diabetes Center to create algorithms to avoid exercise-induced hypoglycemia and has launched a web-based system to provide payers and health systems with a dashboard to identify patients who are experiencing hypo- and hyperglycemia beyond certain prescribed thresholds. 8 Livongo Health strives to ease the burden of diabetes management with real-time information. 9 Each of these companies are developing data driven solutions to reduce patient burden and health care costs.
As will be described in more detail later, companies developing diabetes care solutions should tailor them to meet the unique needs of their customers. In intensive diabetes management for insulin dependent people, there is a tremendous opportunity to take real-time CGM and pump information and aggregate and analyze it with other data sources to offer recommendations to improve health outcomes. In type 2 or nonintensive groups, remote monitoring of blood glucose, weight, blood pressure, activity, food intake, and so on, with algorithms to provide insights based on the data collected, can positively affect outcomes by recommending appropriate therapy and behavior modifications.
In this new paradigm of disease management, we need to stop thinking of people as patients, but rather think of these patients as people—people who happen to have diabetes or other chronic conditions. They also happen to have a family; they jog, attend school, work at a job with varying responsibilities and stressors, and have a noisy neighbor at night, bills to pay, errands to run, events to attend, meals to eat, and so on. Each of these seemingly routine daily events can have a profound impact on a person’s health status. Ideally, to best serve these people, we need to develop solutions that not only recognize and account for these events, but also dovetail nicely into their daily activities, and not create unnecessary burden or become disruptive to their already hectic lives.
Concurrently, other global trends are supportive of customer service and support offerings. Data are becoming more accessible and mobile, able to travel with a person versus being solely located in the offices of each individual provider. The involvement of people in their own health care is expanding, as is the use of mobile apps and call centers for support. Interactions with people will become more frequent and automated, with live support when warranted. As personalized data become more accessible and integrated, so too will the therapy recommendations start to match the individual needs of a person.
Against this macroeconomic landscape is the promise of big data. The fundamental goal is the same “seeking to glean intelligence from data and translate that into health care advantage.” Many people have different definitions of big data, but most agree that it involves large complex databases, often too big and diverse to interrogate using traditional tools. Others add the caveat that the data comes from multiple sources and needs to be integrated prior to use with analytical tools which extract information from it. Big data are useless until they are analyzed and converted into information. Information provides insights. These insights can help us design better products, identify patients who could benefit from our therapies, identify product issues before they become serious, promptly investigate and respond to customer complaints and/or concerns, improve patient outcomes, keep patients out of the hospital, inform providers of product safety and efficacy, and provide valuable real-world information to regulators. In many ways, the current health care trends and changing regulatory environment are prompting us to develop mechanisms to aggregate and monitor patient data throughout the care continuum and certainly at a minimum for an extended follow up period until stability is achieved. In the context of diabetes management, the promise of big data is that they will slow the rising costs of health care, help providers practice more effective medicine, empower patients and caregivers, support preventative health care, and ultimately provide personalized medicine.
There are challenges however with this new paradigm of diabetes care. Often remote monitoring programs require users to wear extra devices, perform home tests, access an app or web portal, and so on. Many people will opt out of programs due to these requirements. Others will opt in initially, but usage will wane over time. In the most basic sense, consumers’ perception of the value the system provides must outweigh the perceived burden of its use. Therefore, ease of use and simplicity of operation are paramount to the success of these programs. Beyond the user challenges, there are hurdles related to the accuracy, completeness, and time stamping of data collected from multiple sources. The reliability of connectivity, usability of the reported data, and ability to distill the information into understandable actions are critical as well. Last, a sound business model that addresses all stakeholder concerns must be created. Ideally, value creation must exist for the user and his or her family, health care team, and payer. Understanding the ideal cohort of patients who may realize the most benefit is critical in early evaluations. Randomized trials and observational studies demonstrating the economic value of the service will help drive adoption from providers and reimbursement from payers. Only when all of these issues are dealt with in an effective way will the service or solution be successful.
Much of this article focuses on a hybrid model incorporating the use of both devices and ongoing support based on various data elements transmitted from devices, primarily due to the proposition that sensor and device information can have great value in monitoring a patient’s well-being. Therefore, when assessing the clinical utility of these new models, the improved outcomes should be based on a control group of device users without the added service element. Also, although not a specific area of focus, a service model not relying heavily on devices may be of tremendous value if it solely focuses on improved adherence to medication and/or lifestyle modification.
Transparency of outcomes, not treatments, will have major implications to the use of our medical devices. On one hand, if the economic value of a therapy is shown to be cost effective, there is tremendous upside for this therapy to become the standard of care. Conversely, if outcomes are not universally beneficial, we may see segmentation effects, where products are prescribed to a segment of the population with appropriate cost benefits from the therapy. Companies working in the diabetes space should consider making a commitment to leverage ongoing service and support programs to better understand people’s health, and use these interactions to improve outcomes, thereby ensuring the vast majority of people receiving their products have outcomes with demonstrated economic value spanning both the immediate period after an intervention, as well as in the long term follow-up period.
Heart failure is 1 example of a condition that is amenable to leveraging remote monitoring to impact patient outcomes and lower health care costs by reducing hospital admissions/readmissions. Approximately 25% of people with heart failure are readmitted to the hospital within 30 days of their discharge. 10 Hospitals are held accountable and financially penalized for higher than anticipated heart failure readmissions, and have recently implemented home health monitoring programs to reduce associated readmission rates. Such programs, private and public, have instituted patient management services that engage with patients postdischarge with the goal of making the home the preferred site of care. One company, CardioCom, partners with patients who are asked to use an electronic scale, blood pressure cuff, and fill out a daily web-based survey. All of these data are collected on a dedicated server at their facility, where algorithms monitor patient parameters daily. If a patient’s situation begins to deteriorate based on tracking the collected signals, the patient is flagged. A representative from the call center contacts the patient and may make a physician preapproved modification to the therapy. In some cases, the situation may require physician intervention. When this happens, all data is accessible by the physician in an easy visual format. Results from small client studies have shown that readmission rates are significantly reduced, and the avoided readmission costs are far greater than the total costs of the service. Therefore, patients experience better outcomes and less hospitalizations; total health care costs are reduced. 11
In this article, the use of big data in diabetes is presented. The implications to outcomes of person-centered care are discussed, and a recommended course of action describing where medical device companies can play a vital role, and how the community can benefit from this future health care environment is described. Although there will be tremendous value generated from customized services for typical diabetes management as described in this article, it is a step short of the ultimate goal of a quantified self, where wisdom in the moment is seamlessly conveyed to a person, regardless of the type of action to be taken, diabetes-related or otherwise.
Methods
There are several opportunities to leverage big data to reduce the costs and burden of disease, while improving outcomes. Driving health care delivery to the patient’s home and minimizing hospitalizations will greatly reduce the burden on the health care system as illustrated in Figure 1. Ideally, more costly and intensive interventions can be avoided by monitoring and supporting disease management in the patient’s home and using predictive analytics to identify potential risks and mitigate them before they become more severe. Essentially, by driving interactions to left in the figure, all stakeholders benefit to the extent that costly exacerbations and ER visits can be avoided.
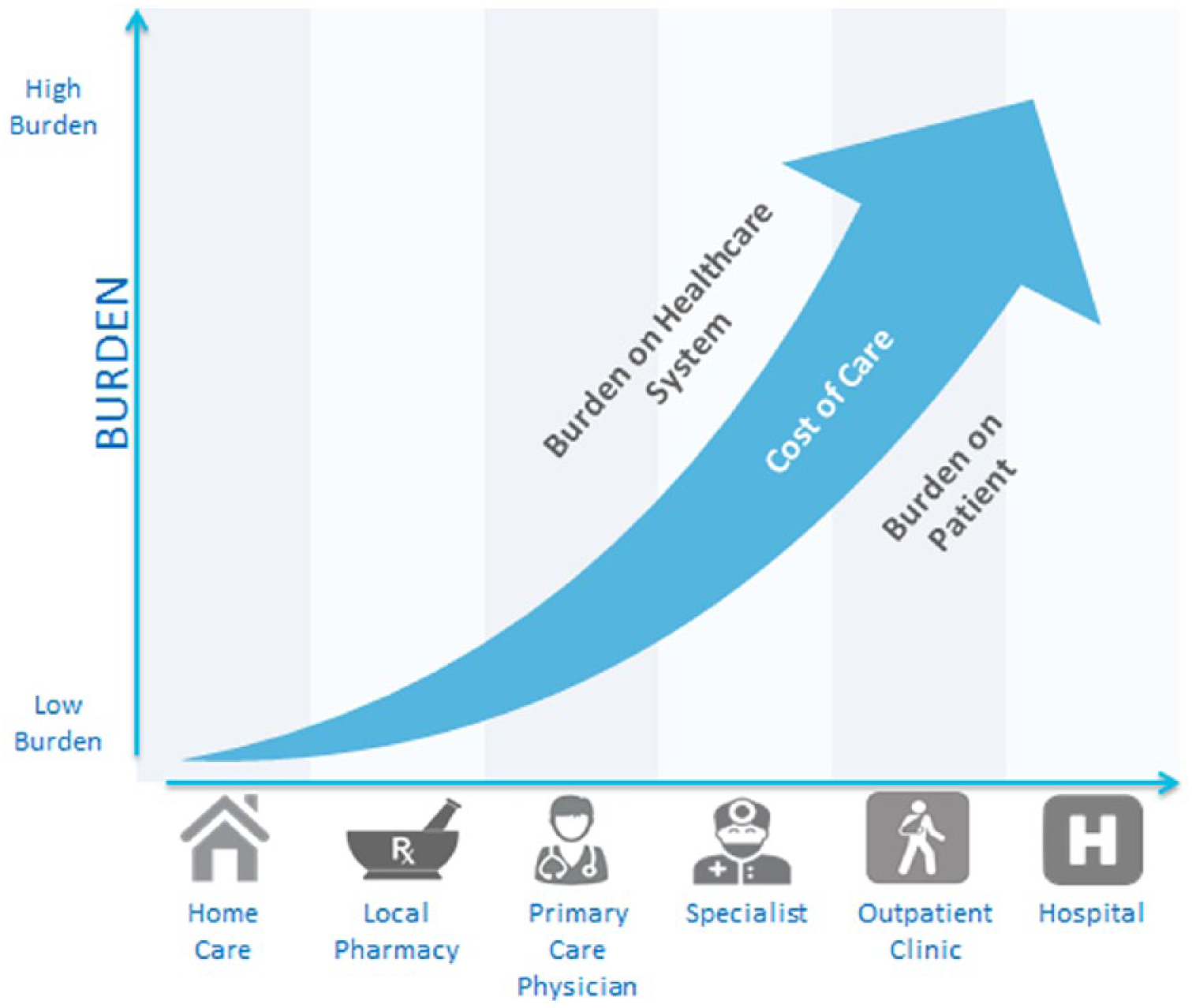
Illustration of how costs of care, burden to the health care system, and burden to the patient increase as care moves from the patient’s home to increasingly intensive service and support.
In addition, big data allow device data to be monitored during clinical trials and postlaunch and provide information to assess product performance as well as offer insights to improve future-generation systems.
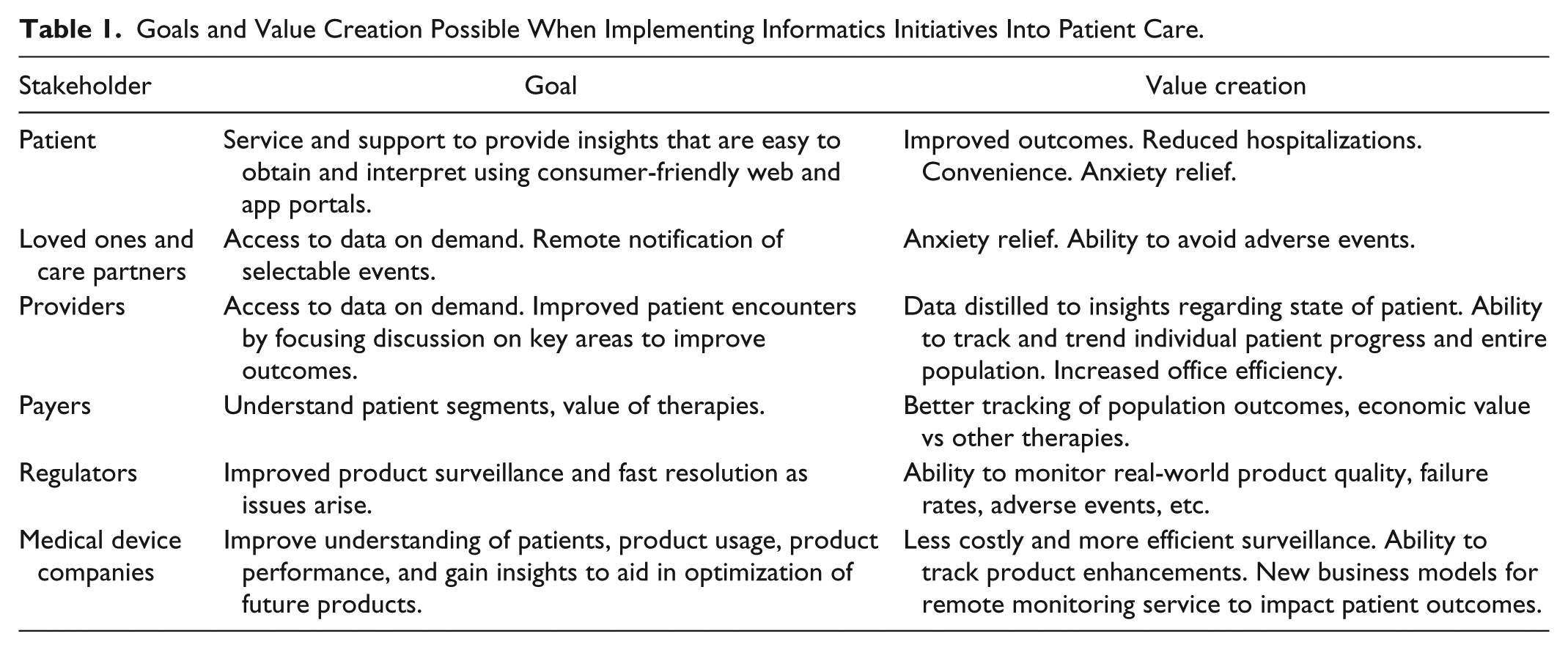
There are many beneficiaries of big data, with specific goals and benefits for various stakeholders (Table 1). The most successful solutions will provide clear value to each of the stakeholders. 12 For patients, they involve easily obtained, consumer-friendly, customized support with exceptional value. For providers, they allow for real-time access to error-free, critical information at the time it’s needed. They also help reduce hospitalization rates, which are impacted today by lack of follow-up and may support preventative care programs. For payers, they improve their understanding of patient populations and market segments and provide the right offerings tailored to patients based on population statistics. Big data will support longitudinal analysis of care across patients, and clinical outcomes can be integrated with financial analysis to understand economic value. For regulators, they allow for improved product surveillance and tracking. For medical device companies, they hold the promise of better understanding our customers, their needs, product performance, and opportunities to improve the design of future products and enhance patient outcomes by partnering with them through their lives with diabetes.
Goals and Value Creation Possible When Implementing Informatics Initiatives Into Patient Care.
Examples of Big Data Value Creation
Making patient data accessible to appropriate stakeholders at the appropriate time
Example for pediatric patients using CGM
Providing a text message notification to the parents of child or adolescent with diabetes who is currently experiencing a hypoglycemia event and not responding to the system’s alert. The historical rate of severe hypoglycemia necessitating the help of another person or a possible ER visit was over 30 events/100 patient years at the time of the DCCT study. 13 With sensor augmented pump platforms, the rate was reduced to 13 events per 100 patient years, 14 and with the MiniMed 530G system, the rate is further reduced to the point where users of the system’s Threshold Suspend feature experienced no severe hypoglycemic events in the 3-month ASPIRE In-Home study. 15 However, in real-world situations, severe hypoglycemia is still a significant issue for many patients, and remote monitoring can provide additional protection against the likelihood of severe hypoglycemia. The recently FDA-approved DexCom Share and Medtronic MiniMed Connect are designed to help mitigate this risk by informing others in real-time of potentially dangerous low glucose events. It should not be understated the value these systems bring in providing peace of mind to patients, their caregivers, and loved ones.
Mining integrated health/wellness data with device data to understand the true status of a patient
This can also provide therapy support in customized patient segments, and replace or augment human decision making with automated algorithms
Example for a person with Type 2 diabetes on oral medications
Monitor health status with activity, food, and vital signs monitoring (weight, BG, blood pressure, heart rate, etc) on a daily basis with algorithms to inform of patient well-being on therapy. Analytics can provide a more detailed understanding of factors such as diet, exercise, stress, and sleep, which can impact glycemic control and lead to hyper- and hypoglycemia (Figure 2). Algorithms can also isolate periods of intense exercise and evaluate the likelihood of hypoglycemia immediately following or during the subsequent night. Aggregation of various data elements allows one to calibrate an individual’s sensitivity of diet, exercise, stress, and other factors on his or her glucose levels. Often data analytics can produce insights that become apparent with a high degree of reliability as many similar events result in consistent glycemic outcomes. Simple summaries of minor adjustments, per physician’s order, can be recommended if warranted.
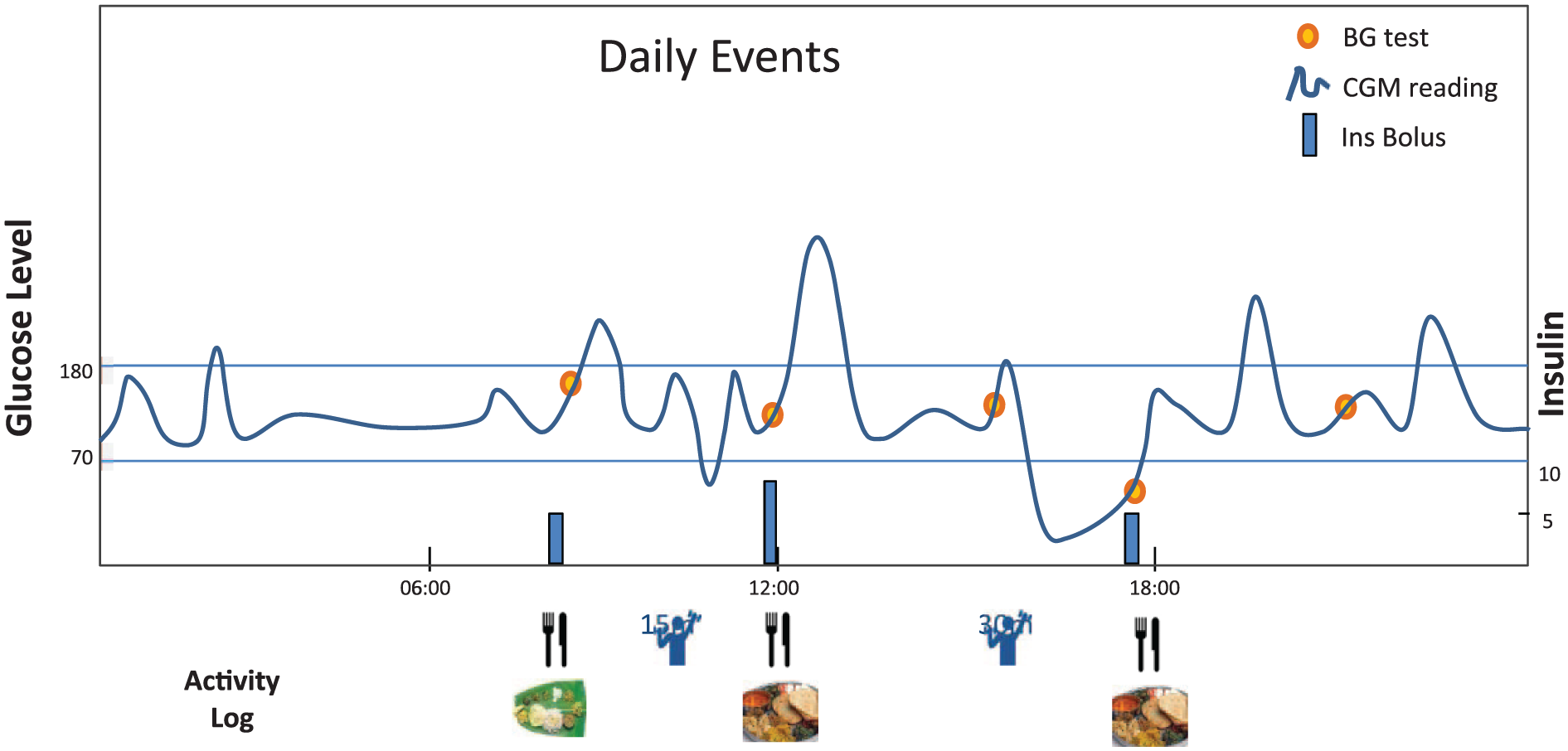
Illustration of daily event log for person with diabetes. Meals, insulin boluses, activity, blood glucose tests (BG), and continuous glucose monitoring (CGM) data are shown. Analytics can summarize effects of diet, exercise, and insulin on glucose levels.
In addition, access and interrogation of device data can allow us to better understand product quality, and validate the utility of product enhancements through the product lifecycle. It can also inform us of patient outcomes, health care provider proficiency, usage of various features, and so on, allowing us to optimize future generations of products.
Most platforms of person-centered services and solutions have a common theme: aggregate patient data from multiple sources to obtain a more comprehensive view of the patient, use analytics to evaluate patient status, intervene when warranted, track health outcomes following interventions, and monitor product performance. Through this process, the economic value of products and services can be demonstrated in support of them becoming the new standard of care.
To achieve these goals, a real-time triage system must be created. As people struggle with certain elements of their diabetes management, the first level of support should be delivered automatically with educational tools and minor therapy adjustments falling within physician prescribed guidelines. Level 2 may require technical support from a call center. In level 3, more serious health issues would require intervention from a health care professional, and last, the most serious situations may necessitate an ER visit. The goal, of course, is to drive issue resolution toward the lowest tier of support that is the least burdensome to both the patient and the health care system. By predicting harmful situations in advance, therapy and behavior modifications can reduce the likelihood of more serious and costly events. Ideally, any new service model should demonstrate improved clinical outcomes and a reduction in the total costs of care. Short of this outcome, an improvement in either area without adversely impacting the other is also acceptable.
Practical Considerations for Service and Solutions in Action
As a starting point in the management of diabetes, it’s important to first segment the population into groups where a certain portfolio of offerings makes practical sense. A typical starting point may be to consider type 1 and type 2 diabetes separately. Another option is to consider the intensity of the required or desired service. This consideration takes into account the fact that many people with type 2 diabetes may be on insulin and desire or require the same level of intensive management as a typical person with type 1 diabetes. Conversely, some people with type 1 diabetes do extremely well, and are completely satisfied with a few standardized injections per day. In addition, cultural, environmental, economic, and psychological factors will also play a role in the level of care. Therefore, for the purposes of this review, intensive and a nonintensive diabetes treatment groups are considered separately.
Intensive diabetes management focuses on sensor-augmented pumps with the vision of commercializing the artificial pancreas and providing new levels of service and support. The goal is to capture important data in real time and disseminate information when it’s needed. In the near future, devices will be connected to transmit all data automatically to the cloud in quasi real-time. As stated earlier, both the DexCom Share and Medtronic Connect support this functionality and were recently approved by the FDA. Two important by-products of this capability allow loved ones the ability (1) to check the status of another on demand through a web app or web portal and (2) to be proactively notified through text messaging of a potential issue such as a low glucose event not acknowledged by the user. In addition, analytics running in the background of the device or in the cloud can look for patterns, and interrogate various low and high glucose events, identify actions in the hours preceding the event which may have contributed to it, and inform the user through educational materials, and other means of avoiding these issues in the future. Moreover, by looking at population data, insights into optimal settings and use of the devices can be obtained and shared among users, physicians, and essentially all stakeholders. As more real-time data from sensors and other factors are added in the future, the opportunity to interact with people is enhanced, and direct moment-to-moment service and support is possible.
The role of services and solutions in the nonintensive group, primarily focused on type 2 diabetes, is very different. Simplicity is paramount, as is minimal intervention with devices and tools. Much thought is focused on the subsegments within the type 2 population, including insulin dependence, oral medications, and diet and exercise. Comorbidities will also be a critically important factor. Within any subgroup, behavior modification tools play a key role to impact diet and exercise. Although the likelihood of positively affecting behaviors in everyone is low, there are opportunities to impact outcomes with more thoughtful solutions. The most effective programs to support people with type 2 diabetes who are not meeting goal with their current therapy of oral medications, may universally include periodic short-term CGM evaluations or BG test schemes, activity monitoring, and knowledge of meal intake, but they will also need to be tailored to the person’s lifestyle. Various tools can be utilized to aid in adherence to therapy. Electronic pill boxes can monitor medication intake. Clearly, diet and exercise are important. A program for Latinos in Southern California may be very different than that for people in the southeastern states. Personalized meal planning and education to reduce caloric intake with better choices within their typical meal options is necessary. Specialty meal apps are already being created for different ethnic foods to address this need. Understanding daily schedules, and where opportunities to improve activity levels exist, is necessary.
Yet in some ways, this is only the tip of the iceberg. We need to better understand the cultural and demographic environment where these people reside. We also need to better understand their overall physical and mental status. Do they have other chronic conditions? Are they suffering from depression, that may have worsened over time due to additional chronic illnesses, the passing of loved-ones, etc? What is their financial situation? What is their primary spoken language? A comprehensive understanding of the person’s medical and mental health is paramount for creating the best solutions for these people. Personalized support to encourage subtle adjustments in not only the health related aspects of care, but also lifestyle may be possible if all factors are considered versus a focus solely on the direct medical condition or employing a one-size-fits-all mentality.
Furthermore, algorithms used for patient interaction should be learning algorithms which adapt as a person progresses through their disease. For example, in a newly diagnosed Type 2, early interactions may focus education on the impact of taking medications as prescribed; then, basic information on how lifestyle modifications can improve their health. Later, more detail about a balanced diet, carb counting, and exercise could be presented. As people become more comfortable with these concepts, other educational modules may be added. If people are faltering in a certain area, new options should be considered. These challenges in therapy and lifestyle management have spawned an emerging focus on techniques to improve learning and adherence to treatment regimens, as well as advanced behavior modification techniques.
Infrastructure
Information Technology needs to provide leading edge technology to store, integrate, analyze, compute/model, and visualize data. Regarding external data, arrangements to share or gain access to data from third parties such as hospital and physician EMRs, payers, and consumers will be necessary to achieve the greatest value. Some of the required capabilities include physical data warehouses for storage, data integration for both retrospective and in some cases for real-time usage, analytical tools such as IBM’s Watson for statistical modeling, and visualization methods delivered through the web, traditional reporting files, or mobile applications on iPhone and Android platforms. Most important, the infrastructure must support regulations pertaining to data security, privacy, and compliance. Fortunately, the infrastructure costs of servers, data aggregation systems, data marts, analytics tools, and so on continue to fall; there are many vendors with solutions in all these areas, and most platforms are easily scaled. Also, for large companies, the IT infrastructure can be leveraged to support all their informatics needs which not only include services and solutions described in this article, but also needs in operations, quality, clinical, human resources, and so on. Almost every department has opportunities to leverage data and informatics to improve efficiencies, reduce costs, and uncover valuable insights.
Conclusion
New service and solutions models leveraging remote monitoring, telehealth, and informatics are already starting to play a major role in the future of health care delivery, and this trend will continue. Real-time data integration and analytics will facilitate/address important health care needs including opportunities to improve patient outcomes and avoid costly interventions, thus improving economic value of therapies, enhanced partnership with payers/providers/patients through ongoing interaction and support, and broader postmarket surveillance to satisfy growing regulatory concerns and better understand the risks and benefits of therapies. As we make further progress in capturing all the real-time information regarding the status of a person and the environment in which they reside to achieve the quantified self, the opportunity exists to deliver moment-to-moment wisdom to people so they may achieve optimal outcomes. Perhaps in diabetes more than any other disease, ongoing service and support can provide huge benefits in allowing people to navigate the challenging course of daily treatment to achieve and sustain euglycemia.
Footnotes
Acknowledgements
I’d like to thank John Welsh and Scott Lee of Medtronic Diabetes and Neal Kaufman from Canary Health for their valuable insights in the preparation of this manuscript.
Abbreviations
BG, blood glucose; CGM, continuous glucose monitoring; EMR, electronic medical record.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JJM is an employee of Medtronic plc.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JJM is a salaried employee of Medtronic plc.