
Abstract
Purpose:
This feasibility study was designed to examine if remote communication technology can be used in the technical training of an insulin pump in adults with diabetes who were familiar with insulin pump therapy.
Methods:
Surveys were emailed to 69 individuals who purchased an insulin pump and had been trained by the manufacturer’s diabetes educators. In consultation with providers, participants were given the choice of receiving training in a face-to-face meeting or via remote communication technology. The survey consisted of 27 questions asking participants’ characteristics, device proficiency, confidence, and their satisfaction with the insulin pump and the training method. Differences between the 2 groups were examined using bivariate analyses.
Results:
There were 17 participants in the remote group and 20 participants in the face-to-face group. Participants had a mean age of 40.9 ± 14.3 years, had diabetes for 24.3 ± 13.8 years, and used an insulin pump for 9.8 ± 4.9 years. The participants in both groups were not statistically different in age, diabetes history, years on insulin pump, device proficiency, confidence, or satisfaction with the training method. The remote group reported less graduate-level education (P < .05) and higher satisfaction scores with the insulin pump training (P < .05).
Conclusion:
Although this study has limitations associated with the small sample size and self-selection bias, the results suggest that remote communication technology may be an effective tool to provide technical training to adults who are familiar with insulin pump therapy. Additional research is required to determine the effectiveness of the remote insulin pump training.
Of approximately 29 million people with diabetes mellitus in the United States, 10% administer insulin to manage their blood glucose levels. 1 Insulin can be delivered subcutaneously by multiple injections per day using a syringe/pen device or continuous subcutaneous insulin infusion (CSII) via an insulin pump. Research has shown that those who use CSII can attain a decrease in hypoglycemic events, better nocturnal blood glucose control, improved metabolic control, and enhancement in quality of life as compared to those who use multiple injection therapy. 2
The actual number of people using insulin pumps in the United States is not known, however estimated ranges are 350 000 to 515 000. 3 There are 7 manufacturers of insulin pumps with the US Food and Drug Administration (FDA) clearance to market their devices. The warranty period for this prescription device is 4 years, which offers people an opportunity to change their insulin pump after that period and, if eligible, receive insurance reimbursement. Although insulin pumps have become smaller and more user-friendly overtime, an intensive 2-part training—(1) diabetes self-management using insulin pump therapy and (2) technical training of the insulin pump—is still required to initiate insulin pump therapy.3,4 The first part of the training focuses on self-management of advanced insulin therapy, including carbohydrate counting, infusion site management, hypoglycemia prevention and management, and prevention of diabetic ketoacidosis. 4 This initial training takes place over several sessions. Once a person is determined to be an insulin pump candidate and has acquired sufficient self-management knowledge of insulin pump therapy, a prescription will be written for the device, provided the health care team has the resources to manage the patient. 3 The second part of the training involves education on the technical aspects of the particular insulin pump.
Traditionally, technical aspects of pump trainings have included a training checklist that would be used in a face-to-face manner by specially trained diabetes educators who are employed or contracted by the insulin pump manufacturer. Delays could occur in the scheduling of these training sessions due to logistical factors such as availability of the diabetes educator, location of the customer, and coordination of the necessary paperwork, which could lead to frustration and dissatisfaction. Accordingly, it is crucial to look for new means of providing person-centered training given the recent advancement and availability of health care technologies. Telehealth using remote communication technology interventions are promising in diabetes care, especially in enhancing individuals’ satisfaction and self-efficacy as well as metabolic outcomes (eg, improved glycated hemoglobin or HbA1C, lowered blood pressure and postprandial blood glucose).5,6
Two recent reviews of telehealth programs for diabetes management clearly indicate that remote communication technology can be used as an alternative to conventional face-to-face education in adult populations.7,8 Types of remote telecommunication technology include teleconferencing, mobile phone applications, computer assisted education, and telephone support. Education content could be delivered via real-time teleconferencing (or synchronous) and asynchronous methods with computer-assisted modules or telemonitoring-based feedback. 9 A recent review of 90 publications addresses that each method resulted in different benefits. 9 That is, groups that used synchronous telecommunication more often reported ease in using the technology and cost reductions due to decreased travel and related expenses. On the other hand, asynchronous methods allowed for more frequent interactions with the diabetes educators, reinforcing the person’s decision-making skills in the self-management of their diabetes. The combination of using both methods, however, resulted in the best improvement in quality of life and health status due to increased feedback and ease of use. 9
While it is promising to use remote communication technology in enhancing one’s knowledge for diabetes self-management,10-12 there are few studies that examined the efficacy of using these technologies for insulin pump training. Thus, the purpose of this study was to examine whether a teleconferencing method could be used effectively in delivering the technical aspects of insulin pump training in adults.
Methods
This feasibility study, employing a cross-sectional survey design, was conducted between July and December 2013. The study protocol was exempted by the University of California, Davis Institutional Review Board.
Study Participants
This study used a convenience sample and included individuals who were age 18 or older, had purchased a t:slim® insulin pump from Tandem Diabetes Care, Inc (San Diego, CA) between July and October 2013, and had been trained by the manufacturer’s diabetes educator. Participation in the study was completely voluntary.
Procedures
An insulin pump is a prescription item and requires specific training on its technical aspects to properly use the device. Depending on the health care provider and customer’s preference, training can be offered by the manufacturer’s diabetes educators via either a face-to-face meeting or remote communication technologies. In accordance with the manufacturer’s policy, the choice for a remote training session was only offered to customers who were over 18 years old and switching from another brand of insulin pump. The reason for these restrictions is that an upgrade training is not as extensive as it would be for someone who is new to an insulin pump, nor is there a need for parental consent.
Both face-to-face and remote training sessions were provided by a Tandem employed diabetes educator who had extensive experience in insulin pump therapy and had been trained on the use of the insulin pump using a checklist. The face-to-face trainings occurred in several settings: the provider’s office, a public gathering spot that offered some privacy (ie, library room or conference room), or the customer’s home. The remote trainings typically occurred in the customer’s home using his or her own personal computer or mobile device with internet access. The remote technologies used were Skype™, FaceTime®, and FuzeBox® for synchronous teleconferencing. It is noted that the company did not provide equipment for the remote training session.
Both training sessions were identical in content and utilized the same training checklist. After the insulin pump training was completed, potential participants provided the diabetes educator an email address. The diabetes educator sent an email message containing a brief description of the study and a link to the questionnaire that was located on the SurveyMonkey® website. 13 Potential participants were asked to complete the survey within a 7-day period on the receipt of the email. The diabetes educator did not send a follow-up reminder email nor collected demographic information of potential participants to ensure the protection of human subjects.
Measures
The survey questionnaire consisting of 27 items was adapted from existing tools and then reviewed by 3 diabetes experts for content and relevance prior to distribution. Four major constructs included participants’ characteristics, as well as post-training device proficiency, confidence, and satisfaction of the individuals.
Participants’ Characteristics
Three demographic questions included age (years), residence (state), and level of education (high school, some college, bachelor’s degree, or graduate degree). Participant’s history of diabetes was assessed with 4 questions: (1) type (type 1 or 2), (2) duration of having diabetes (years), (3) type of insulin pump used (manufacturer), and (4) duration of insulin pump usage (years). In addition, 2 questions were included to gauge the participants’ comfort with touch screen technology (yes or no) and to determine the amount of time they spent per week on a computer (none, 1-5 hours, 6-10 hours, or >10 hours).
Training Preference
Since the authors were not involved in the technical training, 2 questions asked the type of training chosen (ie, face-to-face training vs remote training) and reasons for choosing the training method. The second question required a free-form answer to address the reason why the participant chose the specific training type.
Device Proficiency and Confidence
Five questions focused on the specific knowledge attained from the training with the emphasis on the features and functionality of the insulin pump. These questions were taken directly from the knowledge assessment test that the diabetes educators were required to pass to train customers on the use of the insulin pump. The questions measured specific features of the insulin pump, such as how to stop a bolus, information on Personal Profiles, using the touch screen and loading a cartridge. One point for each correct answer was given, resulting in a total score ranging from 0 to 5. In addition, the participant’s confidence in using the insulin pump was measured using a question with a 6-point Likert-type scale (1 = strongly disagree to 6 = strongly agree).
Satisfaction
Of the remaining 10 questions, the first 6 questions measured satisfaction with the insulin pump using a 6-point Likert-type scale, which resulted in a total score ranging from 5 to 30. These questions were adapted from a subset of the Insulin Delivery System Rating Questionnaire (IDSRQ).14-17 The last 4 questions were adapted from the Telemedicine Patient Satisfaction Survey 18 used to assess satisfaction of teleconferencing training in diabetes education.6,19 The questions centered around the participants’ satisfaction level with the training method itself, and if they would recommend it to another person. It also included questions about the time frame of the training and if it was sufficient to be able to use the insulin pump. A 5-point Likert-type scale (1 = strongly disagree to 5 = agree) was used to measure the level of agreement with each item, yielding a total score ranging from 5 to 20.
Analysis
Survey data downloaded from SurveyMonkey were analyzed using the IBM statistical software package (SPSS version 20). Descriptive statistics were used to calculate means, standard deviations, and ranges for continuous variables, as well as frequencies and percentages for categorical variables. Reasons for choosing the training method with short descriptions were coded into thematic categories. Independent t tests and chi-square or Fisher’s exact tests were used to examine group differences in participants’ characteristics, device proficiency, confidence, and satisfaction with the insulin pump and training method. The level of statistical significance was set at P < .05.
Results
Of 69 survey links emailed to potential study participants, 38 surveys were returned, yielding 55.1% of the response rate. Excluding 1 respondent with incomplete data, 37 surveys were the target of the analysis. Of the surveys, 54% (n = 20) were from the face-to-face training group and 46% (n = 17) from the remote training group.
Participants’ Characteristics
As shown in Table 1, the mean age of the participants was 40.9 ± 14.3 years, ranging from 18 to 69 years old. The majority of the participants completed more than high school education (73.8%; n = 31) and used computers more than 10 hours per week (56.8%; n = 21). All but 2 indicated they were familiar with touch screen technology. In relation to their diabetes history, 90% had type 1 diabetes for an average of 24.3 ± 13.8 years (range: 5-58 years) and used an insulin pump on average of 9.8 ± 4.9 years (range: 2-22 years). When running independent t tests for continuous variables, the Fisher’s exact tests, and Likelihood ratio chi-square tests for categorical variables, there was no significant difference in participant characteristics between the face-to-face meeting and remote training groups (Table 1). The only exception was in the level of education. That is, participants with advanced degrees (ie, graduate-level education) were likely to choose face-to-face education sessions while participants with a bachelor’s degree were likely to select remote training (P < .05).
Participants’ Characteristics.
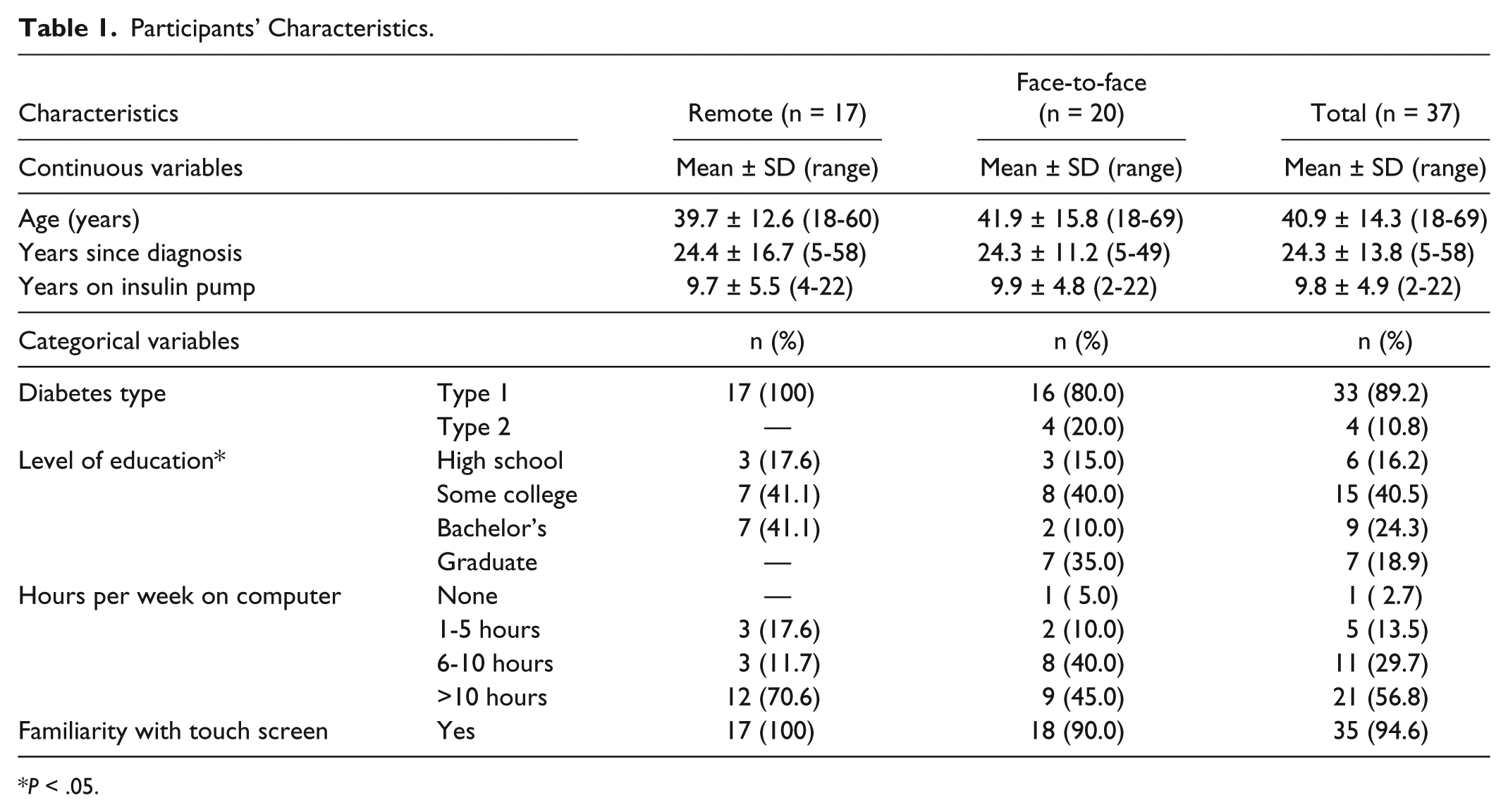
P < .05.
Training Preference
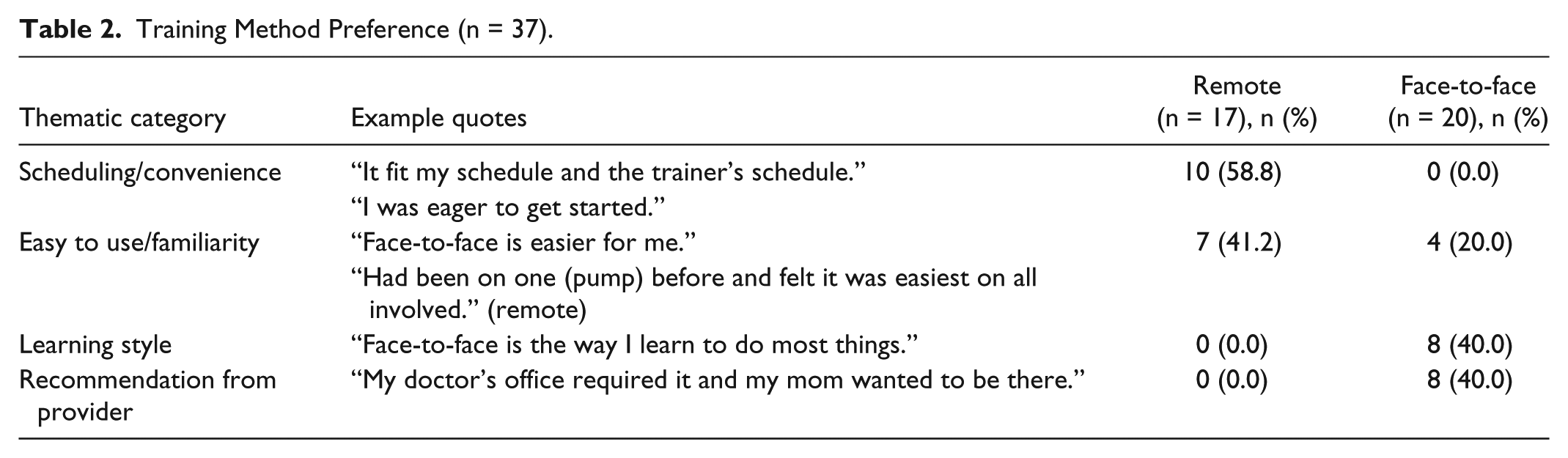
When the study participants were asked to describe in a few words why they chose the type of training, 4 thematic categories were identified: (1) scheduling convenience, (2) easy to use and familiarity, (3) learning style preference, and (4) recommendation from the health care provider (Table 2). The majority of face-to-face training participants addressed that this type of training matched their learning preference (40%) and was recommended by their health care providers (40%). Not surprisingly, a major reason for choosing the remote training method was due to scheduling convenience (58.8%) and easy to use/familiarity (41.2%).
Training Method Preference (n = 37).
Device Proficiency and Confidence
When measuring the participants’ knowledge of the insulin pump features and functionality, both groups presented high device proficiency as the mean scores with the remote group reporting 4.6 ± 0.7 and the face-to-face group with 4.5 ± 0.6. Likewise, the level of confidence in using the insulin pump after the training was similar in the 2 training groups. The remote group had a mean score of 5.5 ± 1.2 and the face-to-face group showed a mean score of 5.2 ± 1.5. There was no statistical difference in device proficiency and confidence across the groups when running independent t tests.
Satisfaction With the Device
As shown in Table 3, the majority of people (70.3%; n = 26) were satisfied with the insulin pump’s touch screen technology as they agreed to the 6 items asking the usability of the insulin pump. Although the overall satisfaction score was high, the score of the remote training group (32.9 ± 2.5) was higher than that of the face-to-face training group (30.8 ± 3.6). This mean difference was statistically significant, t(35) = 2.10, P < .05, and represented a medium-sized effect (d = 0.67), suggesting the remote training group was more satisfied with the device and the training method presented a fairly substantial effect.
Insulin Pump Satisfaction (n = 37).
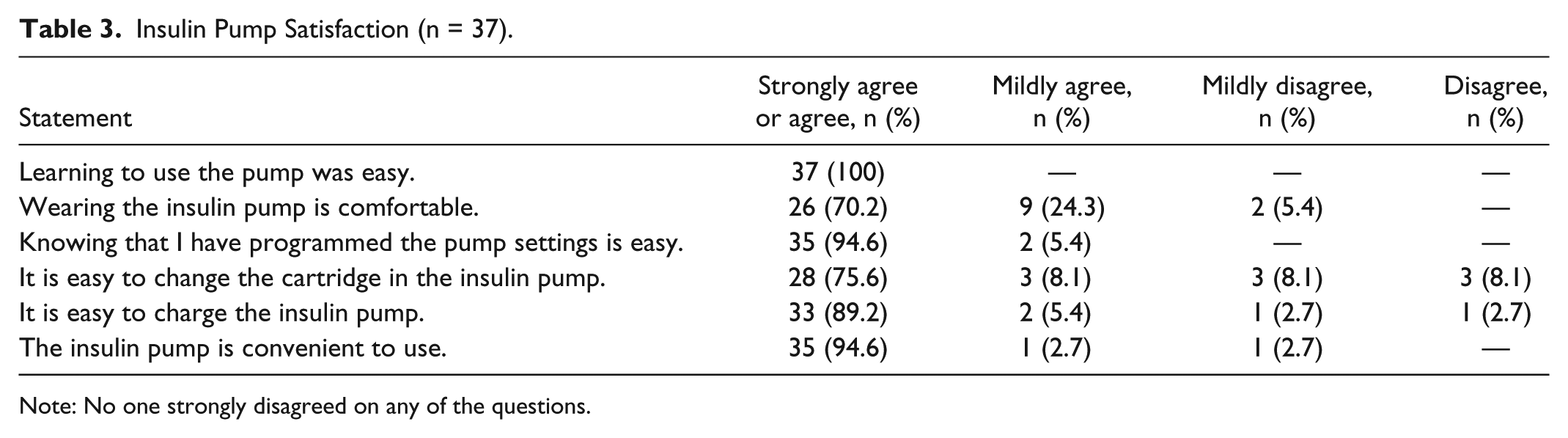
Note: No one strongly disagreed on any of the questions.
Satisfaction With the Training Method Chosen
Four questions asked specifically about their satisfaction levels with the method of training, time to complete the training and whether they would recommend this type of training to someone else. The overall satisfaction score of 19.7 ± 1.4 was close to the maximum score of 20, indicating they were highly satisfied with the method chosen. No statistical difference in the face-to-face (19.6 ± 1.8) and remote (19.8 ± 0.5) groups was found (t = 0.61, df = 35, p = .22).
Discussion
Using remote communication strategies in diabetes self-management education has been shown to be effective and satisfying for patients when compared with face-to-face interactions.6,8 With the increasing needs for education due to epidemic levels of diabetes cases and the relatively small number of diabetes educators, innovative and alternative ways of patient education are essential. Insulin pump training is an area that needs more research to show effective knowledge attainment and satisfaction with synchronous communication methods.
Although this study adopted a cross-sectional survey involving a small number of participants, study findings are consistent with the literature that demonstrates the utility and acceptance of remote communication technologies as an effective, alternative solution for diabetes education and training. Overall device proficiency, confidence, and satisfaction of the study participants were high in both face-to-face and remote groups. This is possibly due to the training checklist that was used in both groups to ensure completeness of training in a logical work flow, as well as the competence of the diabetes educators who performed the training. Furthermore, all the participants were switching from another brand of insulin pump; therefore their prior familiarity with this therapy could have affected their overall satisfaction with the device. The area that received the least favorable scores was in changing the insulin cartridge. Of the face-to-face group, 13.5% reported they disagreed or mildly disagreed in response to “It is easy to change the cartridge in the insulin pump,” and 2.7% of the remote training group reported mild disagreement. Since this process of changing the cartridge is different from other insulin pumps, it may take longer time to become proficient in the procedure.
While each group reported high satisfaction levels with its chosen method of training, the remote training method contributed to higher device satisfaction scores (P < .05) with a medium effect (d = 0.67). It could be assumed that the high scores could have been influenced by giving them a choice in training method. An interesting finding was that the reasons for their choice of training were clearly different between the 2 groups. The group that chose the face-to-face method explained that it was more suited to their learning style or that their health care provider recommended this type of training. In contrast, the participants who chose the remote training method stated it was due to scheduling convenience or familiarity with teleconferencing methods which made this an easy way to learn. The success of using new and alternative ways to deliver training appears to lie with the familiarity and acceptance from both the health care provider and the person using the device. For this reason, offering a choice in training method will continue to be a necessary component for successful learning and high satisfaction.
When assessing the participants’ characteristics in the 2 training groups, there was little dissimilarity in age or duration of diabetes and insulin pump therapy. An unexplained difference was identified in education levels and the choice of training mode, with the face-to-face training group reporting more graduate-level education and recommendation from providers. It is not clear how much providers preferred the traditional face-to-face training against the remote training, and further influenced the participant’s choice. Or there might be a simple reason as remote training requires additional communication tools (ie, computer, smartphone, or tablet) to complete. This dynamic decision-making process might have affected participants’ satisfaction with the device and training method chosen. In light of this, this study presents a limitation but also suggests an opportunity for further research to better understand why certain providers are reluctant or receptive to use remote communication technology for insulin pump training.
In addition, this feasibility study design might have introduced self-selection bias in relation to a convenience sample with a small number of participants. It may be possible that only individuals who were confident with the insulin pump therapy participated in this study, resulting in the high proficiency and satisfaction scores. To ensure the protection of human subjects, we also did not collect demographic characteristics of nonparticipants and thus no comparison between study participants and nonparticipants was possible.
Though this study did not examine the impact of the training mode chosen on metabolic outcomes and quality of life, utilizing remote technologies for patient education has potential to open new doors for delivering care and education. Diabetes educators are the cornerstone of self-management education and training, 20 and need to be able to deliver education effectively and efficiently. With the projected shortage of diabetes educators and the increasing incidence of diabetes, using different technologies is critical to meet educational needs. Not only is the technical portion of insulin pump education ripe for technology to support patient training, but using remote technology to educate patient about the basic components of insulin pump therapy should also be considered. Many hours of advanced insulin therapy education as well as insulin pump troubleshooting sessions need to be delivered to prospective insulin pump candidates to be successful in using this new insulin delivery system.
Currently, education is fragmented in diabetes offices and clinics between the health care providers and the insulin pump manufacturers’ diabetes educators. Diabetes educators should take the lead to standardize an insulin pump therapy curriculum that can be implemented across all insulin pump trainings, to ensure adequate preparation for the insulin pump users and consistent follow-up care through the diabetes offices and centers. Utilizing remote communication technologies could increase the access to standardized education and facilitate more frequent and efficient interactions between patients and their health care providers in the management of this chronic condition. As health care becomes a reality for more people, education in all of its myriad forms has a vital role to play in improving their day-to-day lives.
Conclusion
This study was designed to explore the feasibility of remote communication technology in the technical portion of insulin pump training sessions. Although the sample was too small to deliver conclusive results, it adds to a growing body of evidence that demonstrates positive outcomes and satisfaction with this method of education. Diabetes educators are clearly the drivers of comprehensive education and self-care management of this chronic illness and could be delivering these needed components of care in more efficient ways, to a greater number of people. As the world becomes more mobile and technologies become more accessible and easier to use, it is imperative to explore alternative methods to deliver education and training using teleconferencing technology.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions from the Tandem Certified Diabetes Educators in collecting data and from Dr Deborah Ward and Ms Maureen McGrath in reviewing an initial draft of this manuscript. In addition, the authors would like to acknowledge Susan Morrison, Bob Anacone, and Noel Schaeffer for their guidance and support throughout the whole project.
Abbreviations
CSII, continuous subcutaneous insulin infusion; FDA, Food and Drug Administration; HbA1C, hemoglobin A1C; IDSRQ, Insulin Delivery System Rating Questionnaire.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LP is a full-time employee of Tandem Diabetes Care, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.