
Abstract
Because of its ease and simplicity of its measurement, the morning fasting plasma glucose (FPG), has been as used a surrogate marker for the entire basal day when titrating once-nightly basal insulin. Common in obese insulin-treated patients with type 2 diabetes, late and large evening meals elevate the FPG. This has led to dosing of basal insulin well beyond the basal requirements and contributes to hypoglycemia and weight gain seen with this therapy. It is recommended that during basal insulin titration, the evening meal be limited and hypoglycemia be monitored early in the morning, that bewitching time when the “peakless” basal insulin’s action is peaking and the predawn phenomenon insulin sensitivity is higher.
The morning “fasting” plasma glucose (FPG) is the target of once-nightly basal insulin titration in treat-to-target (TTT) trials and in clinical practice. The components of titration include the initial dose, the frequency and the amount of upward titration, the frequency and content of contact with the patient, and the FPG goal. 1 This goal is usually the average of 2 to 3 consecutive FPGs falling within a range, for example, 70-90 mg/dl. Whenever the goal is exceeded, the dose is increased. In TTT trials this continues until the end of the trial, but in clinical practice it may be forever. In the presence of late-night eating, we believe this titration approach has led to excessive basal insulin dosing. The resulting weight gain and hypoglycemia may be wrongly attributed to the use of insulin rather than its excessive use.
How Much Is Too Much?
Monnier and Colette 2 reviewed 6 treat-to-target (TTT) trials and concluded that titrating basal insulin beyond 0.5 U/kg/d resulted in a disproportionate increase in weight compared to the reduction in HgA1c. In confirmation, 17 arms of 11 TTT trials in which NPH and/or insulin glargine were titrated against a FPG goal were analyzed. 3 A significant correlation was demonstrated by comparing the final mean FPG to the final meal insulin dosage in each arm. At a final mean FPG of 110 mg/dl, the extrapolated final mean basal insulin dose was 0.6 U/kg/d. It is therefore understandable that the American Diabetes Association and the European Association for the Study of Diabetes jointly stated that the maximum benefit from basal insulin has been achieved and bolus insulin be considered when the basal dose is 0.5 U/kg/d or higher. 4 In none of these studies was there control of the evening eating.
In a study of 30 subjects with type 2 diabetes, 10 each on no insulin, basal insulin, or basal-bolus insulin, were initiated on an insulin pump and eating control. 5 The diet was isocaloric (50% carbohydrate, 30% fat and 20% protein) and 1 meal a day was omitted to titrate the basal insulin during the omitted meal time. Titration was guided using continuous glucose monitoring (CGM). The CGM was downloaded and insulin adjustments made during daily weekday clinic visits. A mean basal glucose of 99.9 ± 4.9 mg/dl was achieved, with only 0.226 U/kg/d for the total basal dose.
In another study, subjects with type 2 diabetes previously treated with once-nightly basal insulin were titrated with once-nightly insulin glargine or detemir to a CGM basal glucose goal of 70-120 md/dl between 00:00 and 06:00 hours. 6 The only diet restriction was not eating after 18:00 hours. Of 36 subjects, 4 were found to achieve the basal glucose goal without their previous basal insulin. The 29 subjects completing the study achieved a mean basal glucose of ~100 mg/dl with a mean basal insulin analog dosage of only 0.27 U/kg/d.
Patients previously titrated on once nightly basal insulin but without night eating restriction were recruited for a study if their average FPG was <110 mg/dl and they did not have any self-reported hypoglycemia. 7 Their mean dosage of basal insulin was similar to prior TTT trials, 0.52 ± 0.24 U/kg/d. For 3 days the subjects were monitored by CGM without altering their eating pattern. CGM recorded <70 mg/dl glucose for about 1 hour per 24 hours per person. The average time the subjects started their last meal was about 20:00 hours. For the next 3 consecutive days, they started their last meal at 18:00 instead of their usual time of 20:00 hours. The duration of hypoglycemia by CGM then doubled in all categories, <70, <60, <50, and 40 mg/dl. These results emphasize the impact of late eating on the traditional basal insulin titration.
Why Not More Hypoglycemia?
If more than twice the dosage of basal insulin is used in TTT trials than is needed, why is not more hypoglycemia reported? One reason, the hypoglycemia occurs during sleep.
Once-nightly insulin glargine was titrated by Riddle et al 8 to a mean FPG of 117 mg/dl in a large TTT study of insulin-naive uncontrolled type 2 subjects. Nearly half the self-reported hypoglycemia for the 24 hour period occurred between the hours of 00:00 and 06:00. This was confirmed in another study of 20 once-nightly basal insulin-treated subjects. 7 By restricting their last meal to 18:00 hour, nearly half of the hypoglycemia in these patients also occurred during the 6-hour interval between 00:00 and 06:00 hours. Since most subjects would be sleeping during these hours, hypoglycemia may not be recognized.
Another explanation could be that excess basal insulin may have induced insulin resistance and therefore raised the amount of insulin necessary to produce hypoglycemia. The concept of excess insulin causing insulin resistance has been reviewed by Shanik et al. 9 An illustration of this phenomenon was seen when we attempted much higher initial doses of basal insulin to reach the FPG goal (the mean of 3 FPGs < 110 mg/dl) sooner but avoiding hypoglycemia. 10 We reasoned that this may be possible if the initial dose was matched to the subject’s pretreatment insulin sensitivity. In 20 subjects with uncontrolled insulin-naive type 2 diabetes, the insulin sensitivity was estimated from the decrement of plasma glucose 4 hours following the injection of 0.1 U/kg/d of insulin aspart. The group was then randomized to either once-nightly insulin detemir on a standard initial dose, 0.1 U/kg/d (11.0 ± 2.4 U/d) or a larger dose (60.7 ± 23.6 U/d) as determined by their insulin sensitivity. The larger initial dose group reached the goal sooner (27.8 ± 23.7 days vs 38.2 ± 25.6 days, respectively, P = .186) without an increase in hypoglycemia. However the dose required to achieve the FPG goal was nearly twice that of the traditional starting dose group (79.0 ± 35.7 U vs 45.0 ± 25.9 U, respectively, P = .0142). The larger initial dose appeared to have increased insulin resistance
How Does Traditional Titration Lead to Higher Doses?
Late-night eating is common in obese adults with type 2 diabetes. If one defines eating late and large meals as consuming >25% of daily total calories after supper, the incidence from self-reported questionnaires was 42% in Pakistanis 11 but only 3.8% in those in the Look AHEAD Study in United States. 12 When late eating was documented by computerized vending machines rather than by self-reporting, the incidence was 36% of obese Pima Indians and whites living in Arizona. 13 Reutrakul et al 14 found that late and large meals were common in type 2 diabetes subjects who attended a Chicago diabetes clinic. They identified those patients as “Late Chronotypes.” They tended to be more obese, require insulin treatment, and have poorer glycemic control.
In controlled studies a large dinner meal had only a modest effect on the following day’s FPG.15,16 However there were few subjects in each study, and the dinner was consumed at 18:00 and 19:00 hours, earlier than in our subjects who started their last meal at 20:00 hours. Selecting a high fat and carbohydrate meal, for example, pizza, will lead to hyperglycemia for up to 9 hours later. 17 Doing so, for example, at midnight, one would expect the next morning FPG would be elevated.
Episodic FPG Elevations
The manner in which the titration method is structured also leads to overdosing. Titration is driven by the average of 2 to 3 consecutive FPG levels. A single increase, for example, due to the late-large meal, will elevate the mean FPG and trigger the upward titration.
A hypothetical TTT trial graph comparing the mean FPG, mg/dl, to mean basal insulin dosage, U/d, is shown in Figure 1. After the initial improvement, the mean FPG decreases no further. However, the mean insulin dosage continues to rise. Why? It is possible that some subjects will take much longer to reach goal due to their marked insulin resistance.
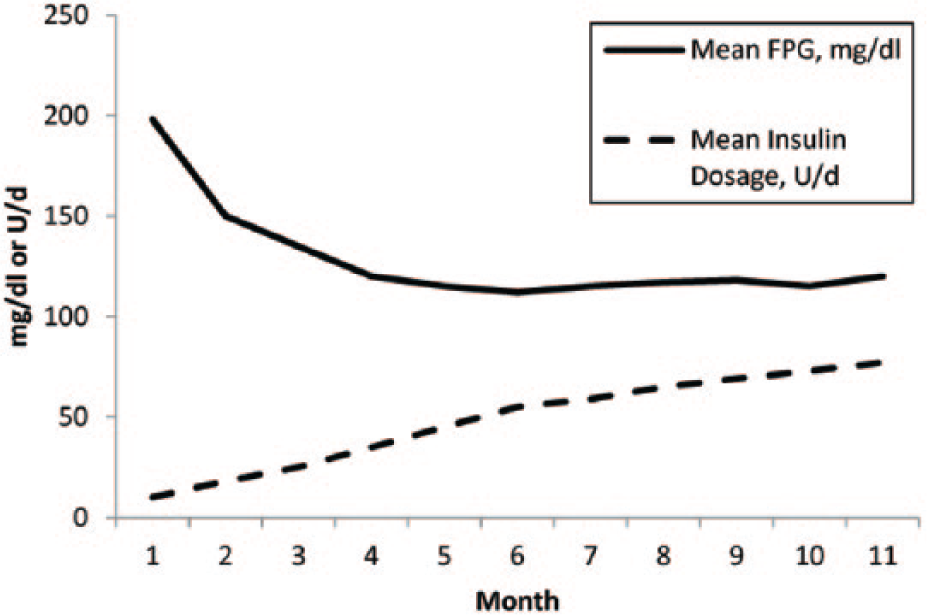
The mean dosage of basal insulin (U/kg/d) is compared to the mean fasting plasma glucose (FPG, mg/dl) in a hypothetical 12-month treat-to-target trial of basal insulin.
An alternative explanation was demonstrated in a study of 20 subjects with type 2 diabetes who were titrated with once-nightly insulin detemir to goal (3-day average FPG of <110 mg/dl). 18 There was no eating control. As in keeping with TTT trials, the dose was increased every time the goal was again exceeded, to the end of the 12-week study. Fifteen subjects reached their goal initially at least 28 days before study’s end. Continuing the titration algorithm, the group’s average dose continued to increased 34.4% yet the mean FPG did not change (actually it increased, 97 ± 11 mg/dl to 105 ± 29 mg/dl). A closer inspection revealed that about half the subjects had no increase in their dose, but half had a dramatic increase dosage, up to 53 U. Figures 2 and 3 depict the daily FPG over the 28-day period for 5 subjects with no dosage increase and 5 subjects with the greatest increase. It can readily be appreciated that there were few variations in the day-to-day FPG in the former group but large episodic increases in those with the largest increase in insulin. These FPG spikes increased the mean FPG and lead to the upward titration in the insulin dose. The standard deviation of the subject’s FPG during this period was highly correlated to the increase in the individual’s insulin dose during this 28-day period (r = .623, P < .01).
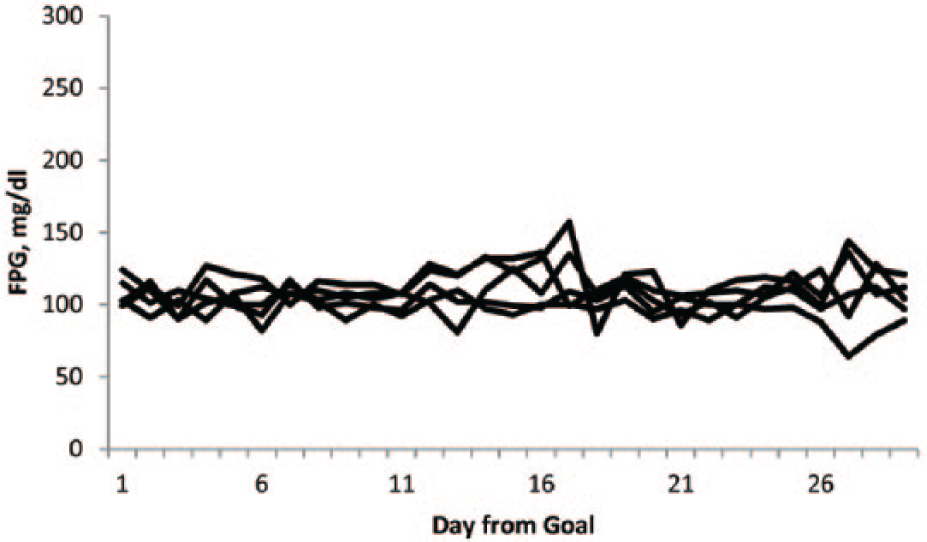
The daily self-monitored fasting plasma glucose 28 days before the end of the 12-week trial but after initially reaching the FPG goal (mean of 3 consecutive FPG < 110 mg/dl) is demonstrated in 5 subjects who did not require further upward titration of basal insulin during this period.
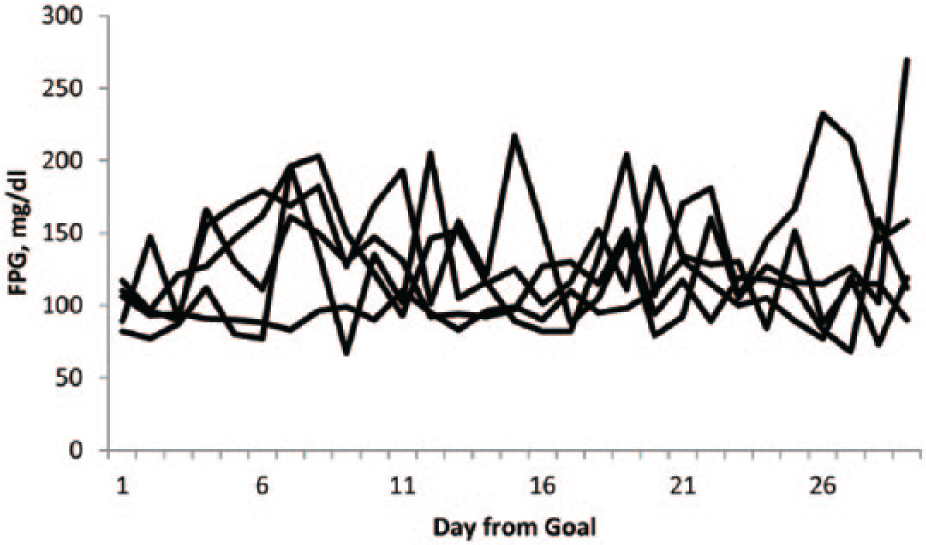
The daily self-monitored fasting plasma glucose 28 days before the end of the 12-week trial but after initially reaching the FPG goal (mean of 3 consecutive FPG < 110 mg/dl) is demonstrated in 5 subjects with the greatest upward titration in basal insulin during this period.
The variability of the day-to-day FPG in insulin treated type 2 diabetes has been related to the basal dosage increase in TTT trials after reaching goal,18,19 hypoglycemia19,20 and weight gain. 19 Interestingly, the variability after first reaching goal is also positively correlated to that variability when basal insulin is first initiated but before upward titration.18-20 This suggests that variability or episodic morning hyperglycemia is a trait of some patients and if detected early may lead to corrective treatment.
Although we believe that late large meals are the major contributor to the FPG variability, we must consider other causes such as the patient’s omission or reduction of insulin dose, 21 blood glucose meter error, 22 variations in insulin action, 23 and sleep dysfunction. 24
Conclusions
When the evening eating is controlled in once-nightly basal insulin treated type 2 diabetes, the basal dose is about half that seen in studies with uncontrolled night eating. The night eating may contribute to a high FPG by raising the next-morning FPG. Night eating can be episodic in some and will lead to upward titration aided by the manner in which titration is done, that is, using the average FPG and continuing the titration beyond first achieving the FPG goal. Perhaps the side effects attributable to basal insulin, hypoglycemia, and weight gained are a product of inappropriate titration and not insulin itself.
Until confirmation by multicenter studies with a larger study population, we recommend that only those FPGs in which the evening meal has been controlled be used for the titration guide. Hypoglycemia with basal insulin may occur during sleep, that bewitching time of peaking of the “peakless” basal insulins’ action 25 and the increased insulin sensitivity prior to the dawn phenomenon. 26 Therefore we would also recommend that the glucose be checked early in the morning. We should not let the morning “fasting” glucose delude us into following the path of excessive basal insulin, weight gain, and hypoglycemia.
Footnotes
Acknowledgements
Part of this material was presented at the 2013 Diabetes Technology and Therapeutic Meeting. The author acknowledges the editorial assistance of Dr Stacey Condren, MD, FACE.
Abbreviations
CGM, continuous glucose monitoring; FPG, fasting plasma glucose; TTT, treat-to-target.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.