
Abstract
Keywords
The carbohydrate-to-insulin ratio (CIR) is used to estimate the grams of carbohydrate that are covered by 1 unit of insulin. Intensive insulin therapy and accurate carbohydrate counting improve glycemic control.1-3 Nevertheless, up to 64% of patients miscalculate their prandial insulin doses. These miscalculations are mostly due to carbohydrate underestimation and may lead to postprandial hyperglycemia.4,5 Corrective insulin boluses are frequently overestimated in this scenario, consequently increasing the risk of hypoglycemia. To avoid these miscalculations and consequent risks, tools have been developed to ease the process of bolus calculation. Current continuous subcutaneous insulin infusion (CSII) systems have incorporated bolus calculators, and some devices have been developed for patients using multiple daily insulin injection therapy (MDI). Even though there is still insufficient evidence regarding improvement in glycemic control, most studies show high patient motivation and satisfaction with these devices.6-8 To perform accurate calculations, these devices require that insulin sensitivity factor and CIR are appropriate for the patient.
Several formulas have been developed to calculate CIR. The “450 rule” was introduced by Walsh and Roberts to calculate CIR in patients using CSII therapy or MDI. Based on their clinical experience, they estimated CIR by dividing 450 by the total daily dose (TDID) of insulin. 9 However, CIR as well as TDID are related to insulin sensitivity. Therefore, this formula can loose its accuracy in certain situations when insulin sensitivity changes, such as with important weight variations. To overcome this limitation, Davidson and colleagues developed new formulas taking patient weight into account. 10 Several authors have proposed further adjustments to these formulas and developed dosing charts based on their population studies.11-14
Differences in dietary composition and meal schedules between populations likely lead to differences in CIR. Nevertheless, little information is available about these differences, and to our knowledge there is no information regarding the Mediterranean population. At the same time, while dietary composition, weight, and insulin sensitivity are believed to influence the accuracy of CIR calculation, some authors also report important variations in CIR according to the time of day.15,16
The formula 500 divided by TDID is commonly used for the initial calculation of CIR in T1DM patients under CSII therapy in our setting. Several authors have shown that this formula underestimates prandial insulin requirements for their populations and CIR may have diurnal variations, which are unaccounted for using this formula.15,16 Therefore, we investigated the CIR used by T1DM patients on CSII therapy in our area to evaluate possible intraday variations, to compare this CIR to that calculated by the 500/TDID formula, and to adjust this formula for our population.
Subjects and Methods
This was a retrospective study. Inclusion criteria were T1DM duration of more than 1 year and CSII therapy duration of more than 6 months. Exclusion criteria were pregnancy, glucocorticoid therapy, and impaired renal function. From a total of 248 patients, 170 type 1 diabetic patients attended at our center were included. Clinical data including anthropometric information, diabetes history, insulin doses, and CIR used by patients were obtained from the clinical database of the Spanish National Registry of CSII Therapy (SNR-CSII). The local ethics committee approved the study, and all subjects provided their written informed consent.
The real CIR was determined for each patient in individual sessions with a diabetes nurse educator. In these sessions patients reviewed carbohydrate counting and insulin bolus calculation. The real CIR was adjusted in a lapse of a week to improve postprandial glucose control and reduce hypoglycemia risk using pre- and postprandial glucose self-monitorization data. Glucose targets were set following the American Diabetes Association recommendations for nonpregnant adults: 70-130 mg/dL (3.9-7.2 mmol/L) for preprandial glucose, and <180 mg/dL (< 10.0 mmol/L) for postprandial glucose. 17 Individualized targets were set for selected patients depending on their specific needs. Each patient’s insulin pump settings were configured with these data for bolus calculation. The insulin pump setting data were then introduced in the SNR-CSII.
We calculated the theoretical CIR using the 500/TDID formula. The theoretical CIR was then compared to the real CIR. The real CIR was also compared between main meals. Patients with optimal glycemic control (HbA1c < 7%) were analyzed as a subgroup because we considered them as a reference group for accurate bolus calculation. Based on the real CIR used, we derived adjusted formulas.
SPSS v19 was used for statistical analysis. Continuous data were expressed as mean ± standard deviation when normal distribution and categorical variables as percentages. The t Student test was used to compare quantitative variables. Differences in categorical variables were evaluated using the χ2 test or Fisher’s exact test when appropriate. Groups were compared by 1-way analysis of variance (ANOVA) and correlations between quantitative variables by Pearson’s correlation coefficient. Statistical significance was defined as P < .05.
Results
One hundred seventy patients met the inclusion criteria. Table 1 shows the population characteristics. Mean HbA1c was 7.6 ± 0.8% for the whole group, and 44 patients had an optimal glycemic control with HbA1c < 7%.
Patient Characteristics, n = 170.
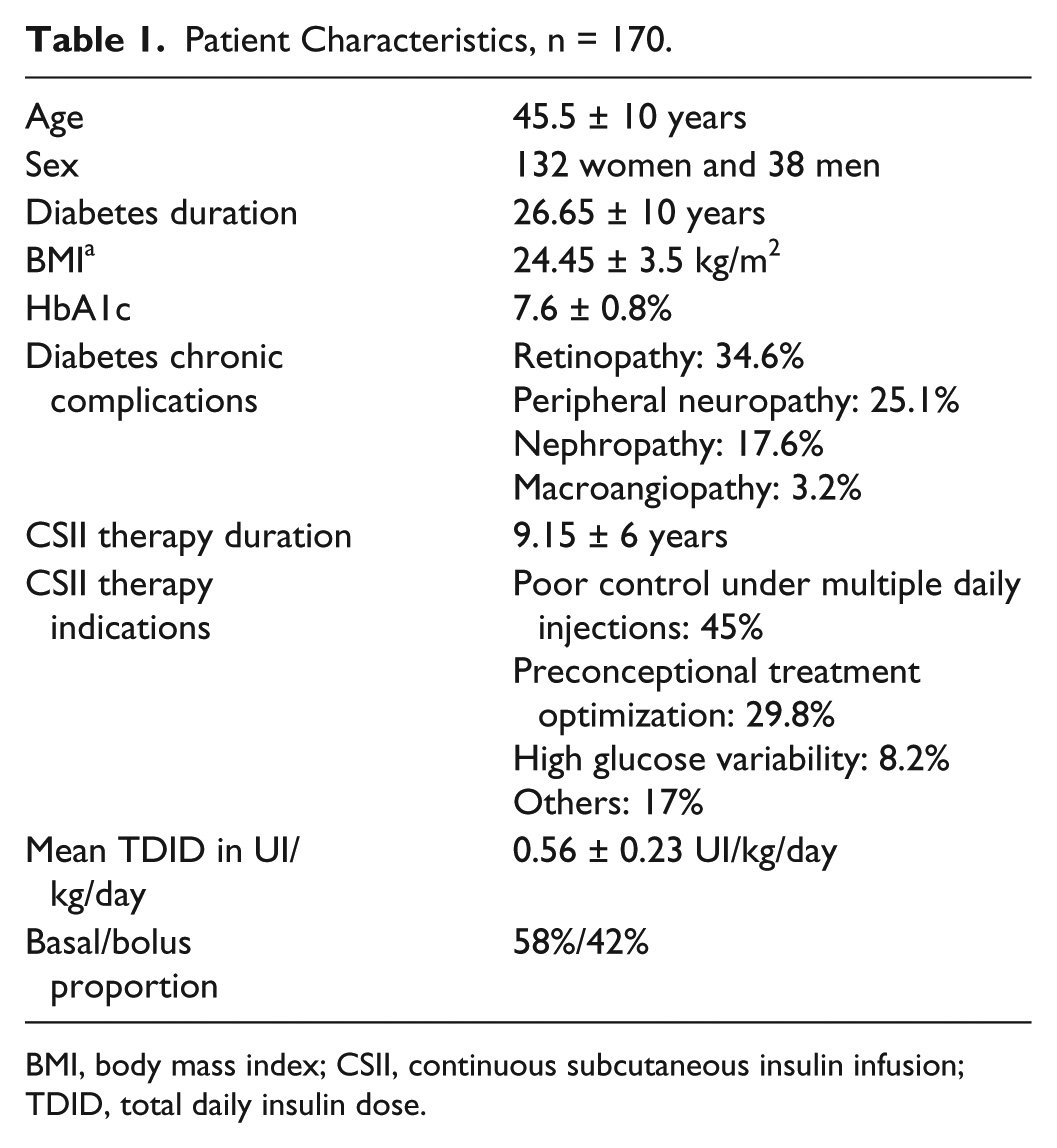
BMI, body mass index; CSII, continuous subcutaneous insulin infusion; TDID, total daily insulin dose.
Figure 1 shows the real CIR compared to that obtained by the 500/TDD formula for both groups. The real CIR for all main meals was significantly lower than the CIR obtained from the formula 500/TDID (P < .005). There were no significant differences regarding patients with optimal glycemic control (n = 44) when compared to the whole group (n = 170). Table 2 shows the real CIR and formulas derived from these real CIR for the main daily meals for both groups.
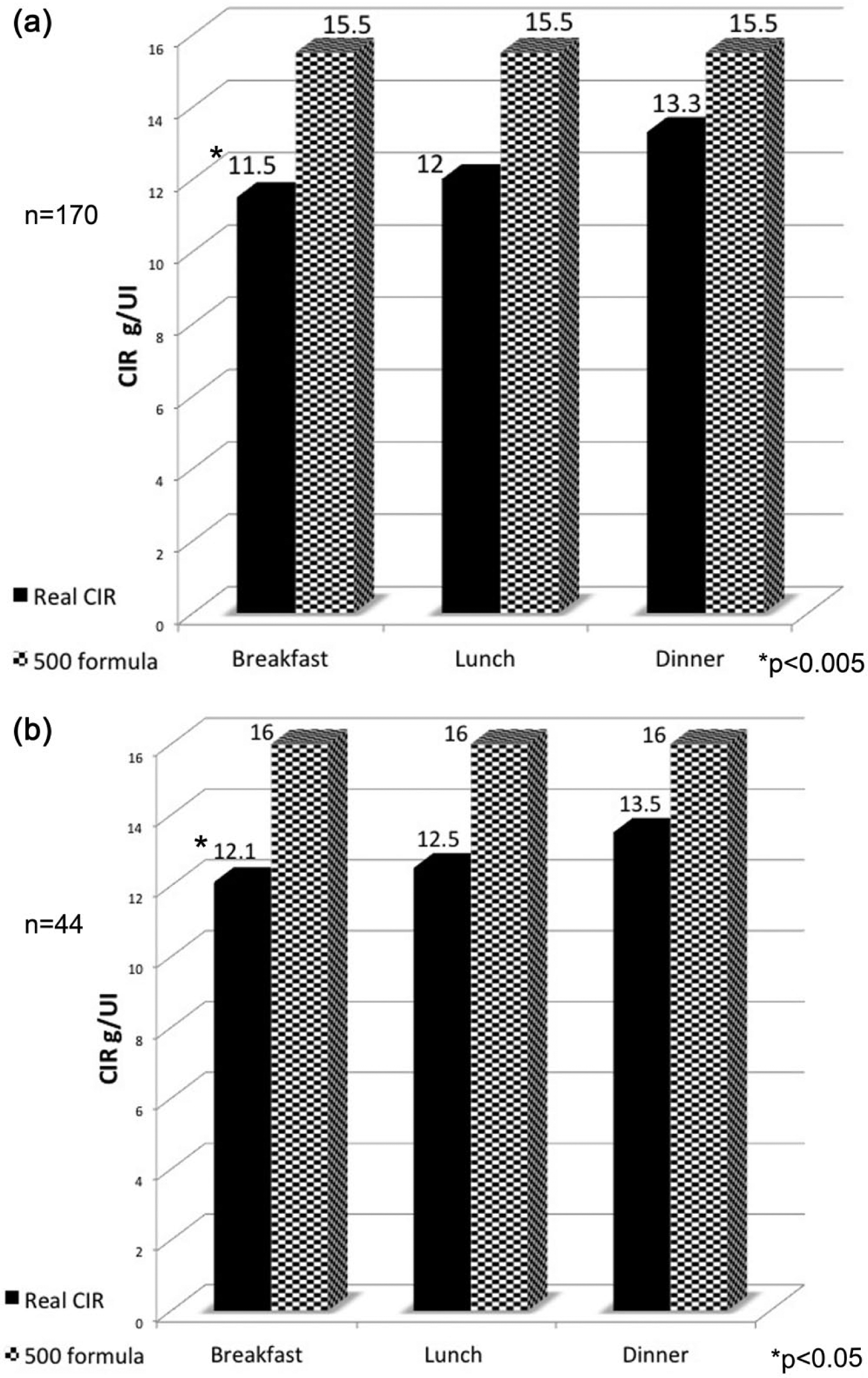
The real CIR used by patients compared to the 500 formula calculated CIR, for all subjects (a) and for the subgroup with optimal glycemic control (b).
The Real CIR Used by Patients in 3 Main Meals and the Formulas Derived From These CIR.
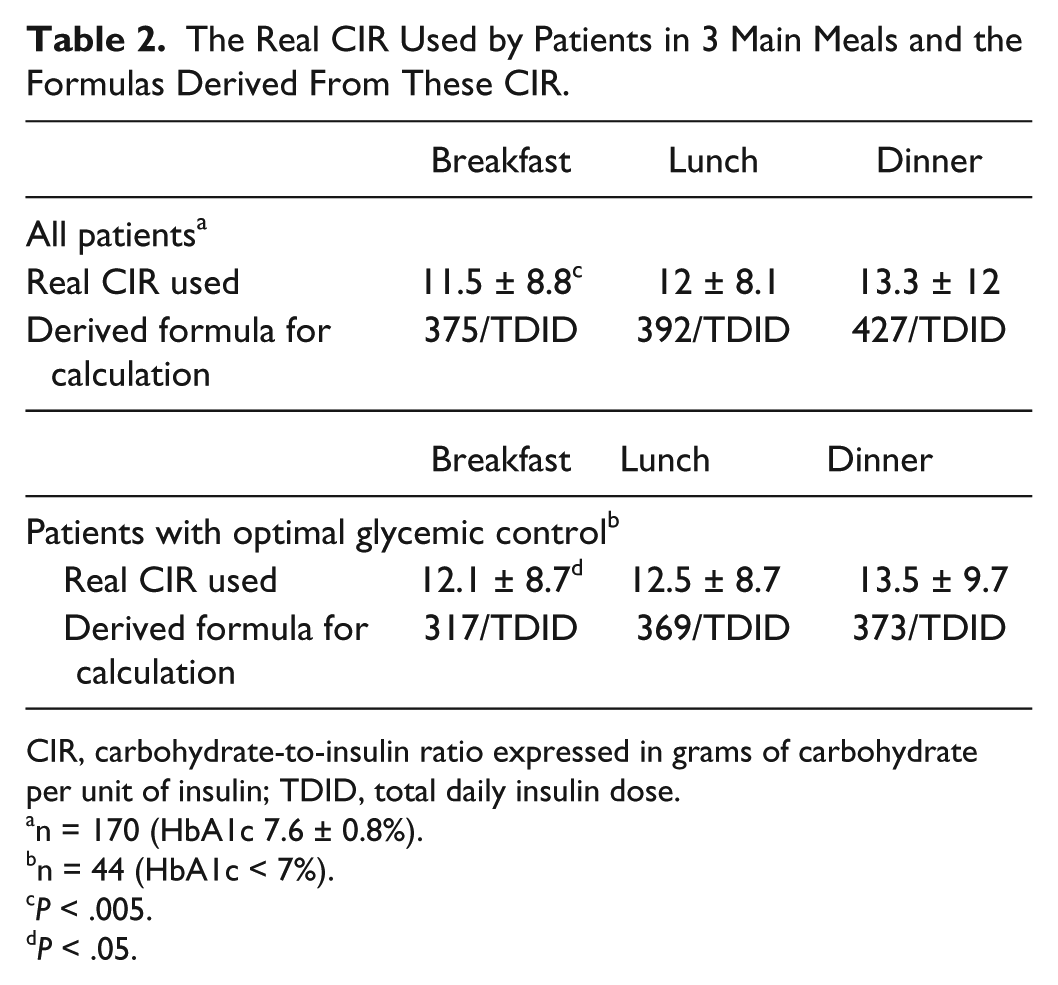
CIR, carbohydrate-to-insulin ratio expressed in grams of carbohydrate per unit of insulin; TDID, total daily insulin dose.
n = 170 (HbA1c 7.6 ± 0.8%).
n = 44 (HbA1c < 7%).
P < .005.
P < .05.
CIR differed significantly between breakfast and lunch and between breakfast and dinner. Breakfast was the meal with the lowest CIR (P < .005). No correlation was found between the CIR and other variables such as age, sex, BMI, HbA1c, or diabetes duration.
Discussion
We investigated the real CIR used by T1DM patients under CSII therapy at our center and found significantly lower values than those obtained by the formula 500/TDID. When comparing between meals we found significant differences between breakfast and the other main meals. Insulin requirements were higher for breakfast.
The subgroup with optimal glycemic control (n = 44) showed similar findings, supporting our results. It is debatable to use HbA1c as an indicator of accurate bolus calculation, given that hypoglycemia has been shown to be prevalent among all ranges of HbA1c. 18 However, there has also been improvements reducing the risk of hypoglycemia with the use of insulin analogues and improving patient’s diabetes education.2,3,19,20 Furthermore, the patients included in this study received diabetes education for carbohydrate counting and hypoglycemia prevention. Glucose self-monitorization data were used to achieve target postprandial glucose levels and prevent hypoglycemia even though these data are unavailable for this analysis.
Other groups have established their own adjusted formulas for CIR calculation in their populations.14,16 It has been postulated that body weight has an impact on CIR given that it affects insulin sensitivity. Therefore, a formula that includes weight and charts with these calculations according to the patient’s weight has been developed. 10 BMI for our population was relatively high, even approaching overweight, but no correlation was found with CIR.
In accordance with previous reports from other populations, our data show that CIR for breakfast is not accurately calculated with the same formula as for lunch and dinner.15,16 The numerical difference between CIR at breakfast and the CIR for the rest of the meals is small in magnitude but suggests a further adjustment to the formulas we use for initial CIR calculation. The adjustment of current formulas for the initial calculation of CIR according to these differences could be clinically relevant.
Different insulin requirements at breakfast might respond to the dawn phenomenon. Other authors have found no significant differences and suggest that higher insulin requirements for breakfast might be a result of inadequate basal glucose control rather than an actual higher prandial insulin requirement in that time lapse.11,14
The main limitation of our study is its retrospective nature. Collateral limitations are that basal insulin rates were not verified in a controlled setting and possible corrective boluses between meals were not taken into account. The main contributions of the present study are that (1) we present CIR data from real-life conditions for the first time from a Mediterranean population and (2) we show CIR in real-life conditions significantly differs from that calculated by the formula 500/TDID. Dietary components as well as daily meal schedules differ among populations and may likely render differences in CIR calculations, but with the present information it is not possible to assess these differences.
Conclusions
The 500/TDID formula underestimates insulin requirements for this population. Similar to a previous report in a Japanese population, 16 a more approximate calculation could be achieved by the formulas 350/TDID for breakfast and 400/TDID for lunch and dinner.
Footnotes
Abbreviations
CIR, carbohydrate-to-insulin ratio; CSII, continuous subcutaneous insulin infusion; MDI, multiple daily insulin injection therapy; SNR-CSII, Spanish National Registry of CSII Therapy; TDID, total daily insulin dose; T1DM, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.