
Abstract
The article by Cobb et al represents solid research work applying the most sophisticated laboratory technologies, a very sound clinical research methodology, and valid statistical analysis procedures. The authors have identified a combination of metabolites suitable to replace the oral glucose tolerance test procedure in the identification of patients with impaired glucose tolerance (IGT) from a fasting blood draw. However, the discussed pathophysiological, clinical, and economic aspects may induce mechanisms restricting the probability of a global acceptance of this test for daily routine.
Type 2 Diabetes is a pandemic clinical phenomenon which is becoming the key challenge of the current century with respect to disease prevalence, costs, and the associated overall social and economic burden to the modern countries and societies. There is no doubt that any improved diagnostic method helping to identify high-risk patient populations, thus allowing for at least an attempt to stop or delay disease manifestation, is to be welcomed and introduced into practice, when the feasibility and added value for daily routine is shown and proven. This may be one of the reasons, why commercial organizations have now started to use modern diagnostic methodologies, such as “metabolomics,”1,2 to identify suitable laboratory solutions for this unmet medical need. A typical example is presented in the article by Cobb et al in this present volume of Journal of Diabetes Science and Technology. 3 It becomes immediately apparent that this manuscript clearly has an important value for the company working on this biomarker panel, which is highlighted by the fact that the article has a substantial number of 13 (!) authors, of whom 10 (!) are employees of the study sponsor.
The reported evaluation itself is providing an impressive and very comprehensive analysis of 2 large patient cohorts. One cohort is used for the identification of the suitable biomarker panel and the second cohort is used for its validation. This method is sound and the statistics applied are in accordance with current state of the art procedures used for this kind of evaluations leaving no doubt about the validity and even reproducibility of the reported results. It can be trusted that the developed QIGT might really be an alternative to the established oral glucose tolerance test (OGTT) for identification of impaired glucose tolerance (IGT) patients in practical routine. However, there is a series of considerations to be discussed, which might also dampen the enthusiasm of the authors, who are even keen to consider redefining IGT by alternative means, including (their?) metabolite profile as indicators for insulin resistance and/or ß-cell dysfunction.
Pathophysiological Considerations
Type 2 diabetes is a multifactorial disease based on several physiological and pathological mechanisms. When described in a simplified model summarizing the existing pathophysiological evidence, it is very likely that an increase in body weight results in an increased hormonal activity of the visceral lipid tissue leading to an initial metabolic insulin resistance. This condition allows the body to tolerate higher insulin levels without risk of hypoglycemia. Insulin is the only physiological hormone, which induces further growth of the lipid tissue, thus closing an anabolic loop to accelerate energy storage in the organism (see Figure 1a). What may have been an excellent survival strategy several thousand years ago, when access to excess food was a rare circumstance, turns to become a real curse in modern civilizations, where food excess can be fortunately considered to be the normal situation. The result is a pandemic obesity, which can, for example, be seen in every country switching from a poor economy with more traditional nutrition to an emerging economy with easier access to food—and especially with access to processed food.4,5 Development of type 2 diabetes requires an additional (genetically driven) dysfunction of the ß-cells, which results in complex secretion disorders and ultimately in an exhaustion of the secretion capacity of the endocrine organ. The resulting quantitative and qualitative dysfunction leads (among other deteriorations) to hyperglycemia (Figure 1b). So in this model, hyperglycemia can be regarded as a later stage symptom of the disease, which introduces an independent and substantial further aggravation to the already impaired survival prognosis of the affected patients. 6
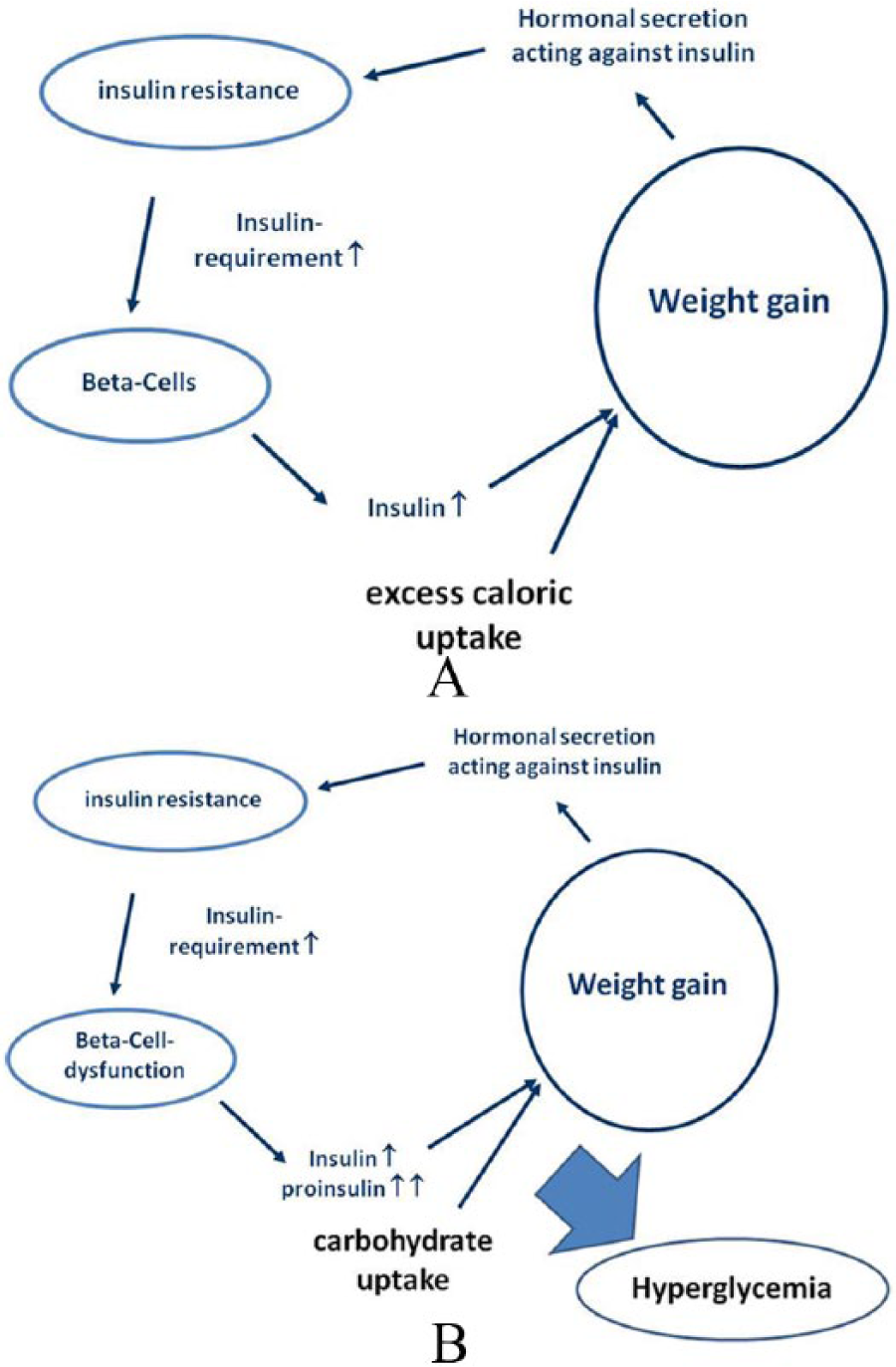
(A) Simplified model of the anabolic metabolic circle leading to weight gain. (B) Development of hyperglycemia in the simplified model of diabetes pathophysiology.
We have a tendency to ignore it, but it needs to be made very clear that the degree of evidence for the current definition of type 2 diabetes and “prediabetes” is not higher than class IV. The current boundaries have been discussed and arbitrarily agreed on by a group of invited WHO-experts 7 and are not supported by any prospective or randomized investigation whatsoever. An FPG > 100 mg/dL and a 2hPG > 140 mg/dL after the oral glucose challenge are not within the mean ± 2 standard deviation range of a “healthy” population, but are still not allowed to be named “diabetes.” From a pathophysiological perspective, it would make much more sense to suggest that repeated blood glucose levels above 180 mg/dL (10 mmol/L = the concentration where glucose becomes toxic to cells 8 ) are defined as “type 2 diabetes,” while indicators of ß-cell dysfunction in case of normal glucose levels (eg, elevated intact proinsulin 9 ) are used to define prediabetes. However, the global community of diabetologists is not ready or willing to consider such pragmatic suggestions, and we have to acknowledge that the current diagnostic criteria are the accepted state of the art and are to be used in daily practice. It will also be very difficult to replace the current “holy grail” HbA1c, 10 which is basically a suboptimal surrogate parameter of a disease symptom, with any other diagnostic parameter.
Clinical Considerations
Patients who are supposed to undergo an OGTT are currently selected by a couple of very cheap to assess reasons and measures, including but not limited to routine checks, pregnancy, increased body weight, increased waist circumference, personal history, family history, and elevated anecdotal glucose levels. As seen in the analyses by Cobb et al, 3 the QIGT score based on 8 parameters (1 blood draw: fasting plasma levels of glucose, a-HB, b-HB, 4-methyl-2-oxopentanoic acid, LGPC, oleic acid, serine and vitamin B5) achieved a predictive hit rate for IGT of 0.83, while the hit rate of a very cheap and easy to assess group of parameters (age, sex, BMI, waist circumference, family history of diabetes, 1 blood draw: insulin and FPG) was already 0.73. Clinically, this translates into an added predictive value of about 10% to identify an IGT patient, when performing the QIGT score as compared to parameters regularly assessed during current daily routine. If health care professionals do not consider this improvement to be very significant, the only remaining advantage of using QIGT will be the time savings by omitting the necessity of a second blood draw 2 hours after glucose ingestion. This is, however, counterbalanced by the availability of a preliminary result, for example, by a point-of-care glucose meter immediately at the end of the OGTT, while discussing the QIGT results may require a second consultation several days later after the results are obtained from the laboratory.
Economic Considerations
The analytical method used for the assessment of the QIGT score is based on an isotope dilution UHPLC-MS-MS method, so a HPLC separation is followed by 2 consecutive mass spectrometry procedures for identification and quantification of several metabolites. In consequence, costs are high. Even if the determination of the biomarkers is fully automated and only focused on the described biomarkers of interest, it may be difficult—if not impossible—to produce the score for acceptable costs, that is, below US$50-80. In consequence, other laboratory tests may have to be developed to determine the identified biomarkers in a cheaper way. In contrast, costs for an OGTT for the cost carriers are in the range of US$25-30 in many countries. In the current situation cost constraints are the major driver for reimbursement decisions, even irrespective of the added value of new drugs or diagnostic procedures. It appears quite unlikely that the presented test, which offers a 10-12% higher identification rate than the cheap measures described in the section above, has a chance to become finally accepted as an acknowledged and reimbursed tool to identify patients at risk for diabetes development. In consequence, patients will have to pay for this test out of pocket.
Conclusions
The article represents a solid research project applying most sophisticated laboratory technologies, a very sound clinical research methodology, and valid statistical analysis procedures. The authors have identified a combination of metabolites suitable to replace the OGTT procedure in the identification of patients with IGT from 1 fasting blood draw. However, the discussed pathophysiological, clinical, and economic aspects may induce mechanisms restricting the probability of a global acceptance of this test for daily routine.
Footnotes
Abbreviations
a-HB, alpha-hydroxybutyric acid; b-HB, beta-hydroxybutyric acid; FPG, fasting plasma glucose; IGT, impaired glucose tolerance; LGPC, linoleoylglycero-phosphocholine; OGTT, oral glucose tolerance test; QIGT, risk of IGT score from the all metabolite IGT test; 2hPG, postprandial glucose 2 hours after glucose uptake.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.