
Abstract
Practitioners need to prepare for a rapid expansion of new concentrated insulins. For many years, the treatment regimens for patients have been limited to 2 concentrations (100 units/mL and 500 units/mL), which pose challenges to both patients and providers. As the new concentrated insulins are at various stages of development, this manuscript reviews the available information on the new concentrated products. This information was obtained from publications, poster presentations, abstracts, and the manufacturers for the products in earlier stages of development. To have a basis for comparison, it is important to understand the activity profile and the challenges with use of the currently available concentrated insulin, regular insulin 500 units/mL (U500R). We also examine how the newer products may assist clinicians and patients with the difficulties faced with the use of U500R.
Keywords
Approximately 90% of people with type 2 diabetes (T2DM) in the United States are overweight or obese and these patients are insulin resistant. Globally, approximately 30% of patients with T2DM are using more than 60 units of basal insulin per day.1,2 Reaching glycemic goals for diabetes is difficult. Almost half of US adults with diabetes did not meet the recommended goals for diabetes care. 3 New concentrated insulins will add tools to tailor insulin regimens for patients who require large daily doses or for use in administration devices (insulin pumps or artificial pancreas) with smaller reservoirs than currently available models.
Pharmacokinetics/Pharmacodynamics
Even though various formulations of U500R have been available since 1952, how this insulin acts in the body is still being investigated.4,5 The first clamp study evaluating the activity profile of human U500R was published in 2011. They reviewed 2 doses (50 units and 100 units) and formulations of regular insulin, U500R and 100 units/mL (U100R), in nondiabetic, obese subjects during euglycemic clamps. This study revealed an activity profile for U500R of similar onset, with a delayed, blunted, but prolonged peak; and extended duration compared to U-100R. 6 The similar onset and bioavailability negated the previous supposition that decreasing the volume led to better absorption. Rather, it demonstrated that the blunted and prolonged activity was indicative of the aggregation of the protein. As this insulin is not used as a single dose, models estimated its activity when administered in multiple daily doses were derived from the small studies of individuals with type 1 diabetes (T1DM) and individuals without diabetes, nonobese and obese. These models indicate an increase in activity after each subsequent dose, with stable background activity and a gradual, prolonged decline in effects. This pattern is similarly postulated to be due to protracted absorption from the subcutaneous depot due to protein aggregation, however slowed clearance may also contribute.4,6 Use of this insulin in multiple daily dosing allows for basal and bolus coverage from the same insulin.
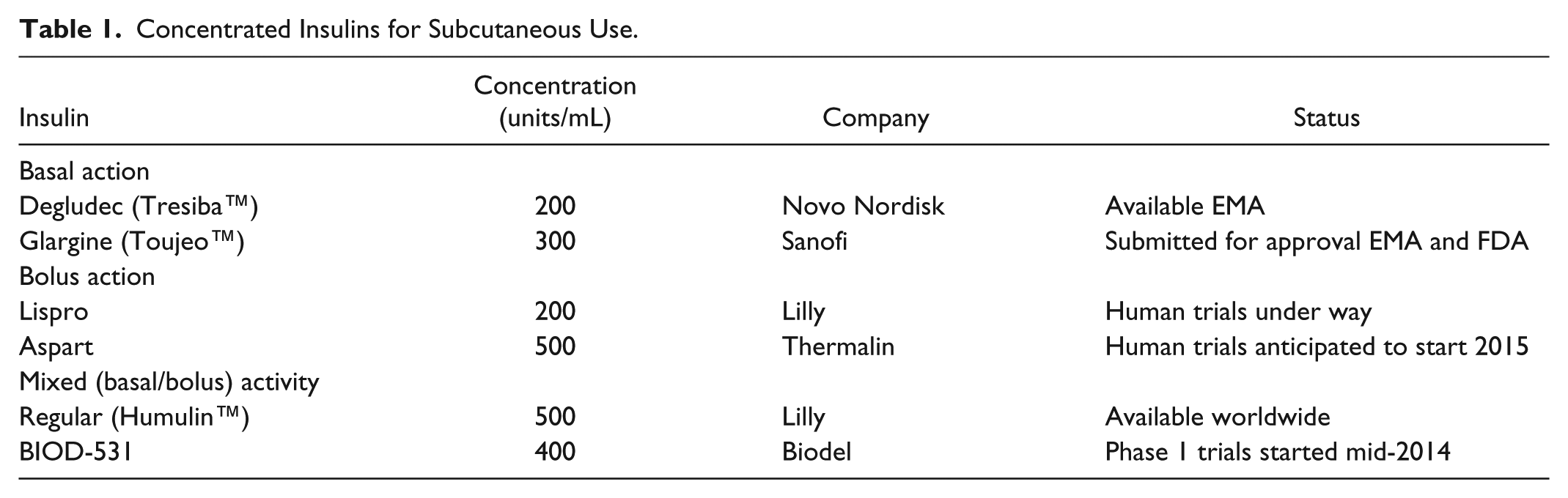
The 5 new concentrated insulins discussed in this article can be categorized based on their prospective utility, their pharmacokinetic (PK) and pharmacodynamic (PD) profiles. The basal concentrated insulins, insulin degludec at 200 units/mL (IDegU200) and insulin glargine at 300 units/mL (IGlarU300), are further in development than 2 bolus insulins, insulin lispro 200 units/mL and a derivative of insulin lispro at 500 units/mL (Fluorolog™), and a mixed activity insulin, BIOD-531 at 400 units/mL. Table 1 provides a summary of the concentrated insulins and their stage of development at the time of this publication.
Concentrated Insulins for Subcutaneous Use.
Insulin degludec 100 units/mL (IDegU100) and IDegU200 were simultaneously developed with the goal of lower within-day variability and extended duration of activity than the current insulins used for basal insulin coverage. 7 Euglycemic clamp studies of individuals with T1DM demonstrated almost equivalent activity during the first and second 12-hour periods of the 26-hour study. Maximum concentration was achieved by approximately 9 hours and declined slowly thereafter. Glucose infusion rates were fairly horizontal in multiple clamp studies with dose-dependent increases when multiple doses were assessed.8-10 The end of activity was not seen within the duration of the clamp studies.8,10 The PK and PD profiles had low rates of variability between the 2 concentrations. 8 Structural modifications allow degludec to form a depot of multiple linked hexamers of insulin upon SC injection that slowly release monomers combined with reversible bonding to albumin enable the desired pattern of effects.8,11
The gradual release of IGlarU300 from a smaller concentrated depot matrix allows for slower and prolonged absorption, similar to U500R. Euglycemic clamp studies comparing glargine 100 units/mL (IGlarU100) and IGlarU300 in individuals with T1DM demonstrated lower peak to trough ratios, with the increase in concentration occurring by 2 hours and continuing through 12 hours followed by a gradual decline through the 36-hour duration of the studies.12,13 Duration of activity was longer for IGlarU300 maintaining euglycemia for a mean of 32 and 34 hours for doses of 0.4 and 0.6 units/kg compared to 29 hours for 0.4 units/kg of IGlarU100.12,13 Lower within-subject variability was seen with IGlarU300 than previously reported with IGlarU100.14,15 Increasing the concentration from 100 to 300 units/mL, results in prolonged activity with low within-day and subject variability that may provide consistent basal activity for individuals requiring high doses of insulin.
Although the more rapid-acting concentrated insulin options have either yet to start human studies or recently finished phase 2 trials. Preclinical trials using swine models and the early phase trials give an insight into their future utility. The furthest along in development is BIOD-531. This 400 unit/mL formulation uses ethylenediabminetetraacetic acid (EDTA) and citrate to facilitate monomer stability for rapid absorption and magnesium sulfate to decrease injection site irritation. Its preclinical studies illustrate the significant PK and PD differences between the BIOD-531 compared to lispro protamine/lispro 75/25 100 units/mL and U500R in nondiabetic, obese subjects. Compared to a dose of U500R of 1 unit/kg, BIOD-531 1 unit/kg demonstrates faster onset (7.2 vs 21.4 minutes), higher (6.28 vs 5.54 mg/kg/min) and more rapid (223.8 vs 393.3 minutes) peak, and shorter duration (1165 vs 1383.6 minutes) of effects. When compared to a dose of 0.5 units/kg of lispro protamine/lispro 75/25, BIOD-531 0.5 units/kg exhibited a faster onset (14.6 vs 35.9 minutes), higher peak effect (4.89 vs 3.1 mg/kg/min), although the time to peak was not statistically different (131.3 vs 160 minutes), and shorter duration (1076.2 vs 1284 minutes) of effects. 16 The formulation differences allow BIOD-531 rapid absorption along with a significant duration of effects revealing the potential for both bolus and basal effects similar to U500R.
Fluorolog, a derivative of lispro insulin is under development for its bolus insulin activity. When administered as a single injection to Yorkshire pigs, Fluorolog was found to have an onset similar to lispro 100 units/mL and significantly faster than U500R; with delayed (~150 minutes postinjection) and higher peak effects compared to lispro, although sooner and significantly higher than U500R (~180 minutes); and similar duration to lispro, which was significantly shorter than U500R. 17 Thus, this insulin is expected to demonstrate potent bolus effects without the basal effects when human studies are completed.
The PK and PD profile for the higher concentration of lispro (200 units/mL) have not been published or presented prior to this publication. Extrapolation based on the similar profile seen with the IDegU200 compared to the 100 units/mL formulation, indicate that the profile of insulin lipro 200 units/mL should be very similar to the 100 units/mL formulation, 8 thus allowing the higher concentration of lispro to be used solely as a bolus insulin.
Efficacy Studies
As several reviews of the retrospective and few prospective studies using concentrated U500R insulin have been published, they will not be discussed in this publication.18,19 The published evidence of the improvement in glycemic control with the new concentrated insulins was limited to the basal formulations at the time of this review. A total of 1993 subjects were exposed to these basal formulations (1765 subjects in the various EDITION trials for IGlarU300 and 228 subjects in the BEGIN LOW VOLUME trial of IDegU200) to assess their efficacy.20-27 The information from these studies has been organized by their primary glycemic control endpoint, hypoglycemia, and weight-related changes presented within the available abstracts and articles.
Glargine (300 Units/mL)
The most extensive investigative program for the newer concentrated formulations is the EDITION trials which evaluated IGlarU300. The EDITION trials demonstrated noninferior glycemic control between the IGlarU300 and IGlarU100. Four of the trials were conducted in subjects with T2DM adding IGlarU300 to various regimens (EDITION 1-3 and EDITION JP-2), while 2 studies were conducted in subjects with T1DM (EDITION 4 and EDITION JP-1).20-26 A summary of the baseline characteristics of the subjects and the results of the EDITION trials is included as supplemental information (available at: http://DST.sagepub.com/supplemental).
When evaluating the EDITION studies, it is important to note that higher doses of IGlarU300 are necessary to attain similar efficacy to IGlarU100, except for EDITION JP-1 where dosage requirements were comparable. The majority (80%) of the difference in dosage appears to be reached by month 4 in most of the EDITION trials.20-23 In EDITION 1, prandial insulin doses were comparable throughout the 12-month study. 20 In EDITION 2, the mean daily basal dose was higher by approximately 12% for IGlarU300. 22 This trend was also seen for T1DM in EDITION 4, however EDITION JP-1’s results showed similar total insulin doses.25,26
The primary endpoint for the EDITION trials was the change from baseline in hemoglobin A1c (HbA1c). All of the EDITION trials revealed similar HbA1c reductions with IGlarU300 and IGlarU100. In the EDITION 1 trial, glycemic control was maintained through the 6-month open-label extension period, with similar prandial insulin requirements for both groups.20,21 The EDITION 2 trial revealed improved control of HbA1c was maintained at 12 months, with a similar decline in fasting plasma glucose (FPG) for both glargine formulations in addition to oral agents. 22 Insulin-naïve subjects studied in the EDITION 3 trial saw similar HbA1C reductions in both treatment groups. 23 The EDITION JP-2 trial focused on Japanese subjects for a 6-month intervention, which found achievement of similar declines in HbA1c, no differences were observed in change from baseline in FPG or in the percentage of participants at HbA1c target (< 7%), with similar percentages achieving target without experiencing confirmed (<54 mg/dL) or severe hypoglycemic events. 24
Similar reductions in HbA1c were achieved by subjects with T1DM in both the EDITION 4 and EDITION JP-1.25,26 The EDITIONJP-1, which evaluated Japanese subjects with T1DM, also found that 15.6% and 20.0% of subjects achieved the target HbA1c receiving IGlarU300 and IGlarU100, respectively, with approximately 13.5% in both groups reached the target without any hypoglycemic events. 26
Hypoglycemia was measured in many different ways in the EDITION trials. Depending on the study, hypoglycemia was defined as confirmed hypoglycemia (≤70 mg/dL) or severe hypoglycemia, nocturnal hypoglycemia, and/or annualized hypoglycemia rates or events per participant-year. EDITION 1 reported lower percentages of participants experiencing confirmed or severe hypoglycemia with IGlarU300. In addition, IGlarU300 was associated with 21% fewer patients experiencing severe or confirmed nocturnal hypoglycemia between month 3 and month 6.20,21 It is not clear if the open-label design contributed to this difference, as the providers may have provided additional counsel regarding precautions with IGlarU300, since it is a concentrated insulin. EDITION 2 showed comparable percentages of participants reporting more than 1 confirmed or severe hypoglycemia (RR 0.96, 95% CI: 0.89 to 1.02). However, percentages of nocturnal events were lower with IGlarU300 (RR 0.84, 95% CI: 0.71 to 0.99). A similar percentage of participants experienced severe hypoglycemia. 22 EDITION 3 considered hypoglycemia as a secondary end point. The relative risk of experiencing any confirmed or severe events at any time was lower with IGlarU300 (RR 0.75; CI: 0.57 to 0.990). Episodes of severe hypoglycemia were infrequent in this study. 23 Fewer participants reported ≥1 confirmed or severe event in EDITION JP-2 with IGlarU300 and a significantly lower percentage of participants experienced ≥1 event during the first 8 weeks. The percentage reporting ≥1 nocturnal hypoglycemic events was also reduced with IGlarU300. Similar to EDITION 3, severe hypoglycemia was infrequent in both groups. 24
EDITION 4 calculated rates of nocturnal hypoglycemia from month 3 to 6, but they were not prespecified secondary endpoints. No difference between treatments was shown in the rate of hypoglycemia at any time (24 hours). Rates of nocturnal hypoglycemia were lower for IGlarU300 in the first 8 weeks, when the majority of dose increases occurred. Rates of hypoglycemia were comparable regardless of injection timing. 25 EDITION JP-1 demonstrated statistically lower hypoglycemic event rates with IGlarU300 (20% rate reduction). In addition, the rate of nocturnal hypoglycemia was lower with IGlarU300 (34% rate reduction) and a lower or comparable percentage experienced ≥1 confirmed or severe event with IGlarU300 than IGlarU100. Last, the percentage of patients affected by severe hypoglycemia was 5.7% and 9.9% with IGlarU300 and IGlarU100, respectively. 26
Even though the participants on IGlarU300 tended to require higher doses, the weight changes were either comparable or favored IGlarU300 in the EDITION trials. Participants in EDITION 1 and 3 had similar weight changes between treatment groups.20,23 Whereas those on IGlarU300 in the EDITION JP-1 and JP-2 saw their weight decline, those in the EDITION 2 and 4 gained less weight compared to those on IGlarU100.22,24-26
Degludec (200 Units/mL)
Although many studies are available using insulin degludec 100 units/mL (IDegU100), 1 study was available for inclusion for IDegU200, the BEGIN LOW VOLUME trial. This 26-week, randomized, controlled, multinational, treat-to-target trial compared IDegU200 to IGlarU100 in insulin-naïve subjects with T2DM adequately controlled with oral antidiabetic drugs. By week 26, IDegU200 reduced HbA1C (by 1.3%) and was not inferior to IGlarU100. Mean observed FPG reductions were greater with IDegU200 compared to IGlarU100 (−67 vs −61 mg/dL: estimated treatment difference (ETD): 0.42, 95% CI −7.08 to 0.006; P = .02). No differences in hypoglycemia rates were observed between IDegU200 and IGlarU100 (1.22 and 1.42 episodes/patient-year, respectively). The daily basal dose was significantly lower (by 11%) with IDegU200 compared to IGlarU100. Quality of life assessments, using the Short Form-36, identified 2 of 8 domains in the Health-Related Quality of Life questionnaire significantly favored IDegU200, less bodily pain (ETD 1.6, 95% CI 0.1 to 3.2, P = .04) and improved vitality (ETD 1.5, 95% CI 0.1 to 3.0, P = .04). 27
To provide more insight into the future utility of IDegU200, a 32-week phase 3 trial comparing the efficacy, patient-reported outcomes and safety of IDegU200 vs IGlarU100 in subjects with T2DM requiring high-dose insulin was completed. The trial’s aim was to confirm the efficacy of IDegU200 versus IGlarU100 in controlling glycemia with the primary outcome of change from baseline HbA1c at the end of two 16-week treatment periods. Although this trial was completed in January 2014, the results were not available at the time of this publication. 28
Over the next several years, human studies of lispro 200 units/mL, BIOD-531, and Fluorolog will become available to evaluate their prospective utility, efficacy, and safety.
Challenges With Concentrated Insulin: Will Newer Products Provide Solutions?
Product Identification
One of the major concerns is making sure the patient receives the insulin one intended them to receive. When 2 different concentrations are marketed under the same brand name, confusion may occur at several points in the prescription and dispensing processes: patient reporting of dose based on unit-marks or incorrect concentration identified during provider ordering and/or pharmacist dispensing. 5 Misidentification in which Humulin insulin is required may lead in overdosing of individuals requiring a dose of 100 unit/mL or under-dosing for those requiring U500R, resulting in significant and prolonged hypo- or hyperglycemia.
These same concerns could occur with insulin degludec, as both the IDegU100 and IDegU200 are marketed as Tresiba™. 29 One possible solution is concentrated formulations marketed under a separate brand name, as demonstrated by the submission of IGlarU300 with a brand name of Toujeo™, rather than Lantus™. 30 Monitoring of product identification errors once IGlarU300 is available will be essential to determine if this resolves this issue or should another resolution be explored.
Administration: Injection, Dosing, and Devices
Patients who require more than 200 units/day face difficulties administering their required amount of insulin. If they use syringes for administering insulin from a vial, they may have to inject themselves 5 to 10 times throughout the day to successfully administer their required doses. This is often due to the volume of insulin, maximum volume for syringes is 100 units, leakage from the injection site, and pain on injection. 5 As for those using the available insulin pens or pumps, they are significantly limited by the cartridge or reservoir size and the administration limits of the devices. 31
Currently, the only concentrated insulin available in the United States is available only in a vial, which poses several challenges for patients. First, no device calibrated to inject based on actual units is available for concentrations other than 100 units/mL. Although a human factors assessment of a syringe calibrated for 500 unit/mL was published in 2013 32 and there are reports of an ongoing human factors study evaluating a prefilled pen calibrated for 500 units/mL by Lilly, USA. At this time, U500R requires delivery using either tuberculin syringes, which measure the fluid by volume, or using insulin syringes, for which the dose is often expressed as “unitmark.” As patients are initially trained to understand dosing of insulin by units, either option can lead to problems in patients understanding their dosage.
Administration of U500R dosed by volume using tuberculin syringes is the technique recommended by the Institute for Safe Medication Practices. 33 This technique offers a unique designation of dose, by volume or milliliter, rather than by units, thus allowing easier recognition of the use of U500R upon patient report by health care practitioners. Due to the same brand name, Humulin™, ability to use the dosage units for identifying the use of U500R versus the 100units/mL formulation is particularly important.
Use of the “unitmark” or “syringemark” for dosing of U500R allows patients to use traditional insulin syringes. This option offers the comfort of using thinner needles, but requires practitioners and patients to understand the dosage conversion. As mentioned above, patient reports of their dose using this method may result in misidentification of the concentration of insulin. In addition, calculation errors by either patients or providers may lead to incorrect dose administration and/or adjustment.
Tuberculin syringes are only available with larger needles, are not covered by most insurance, and are rarely available in pharmacies. These difficulties may delay initiation or cause interruptions in treatment.
Regardless of the administration method, errors could occur with the potential for significant adverse outcomes. Effective communication is required between providers, patients and pharmacists regarding dosage initiation and changes, as well as the administration method, to facilitate patient receipt of the correct products and appropriate use of their insulin. Resources have published conversion tables to assist in dosage calculations.5,34 Wallet cards are available from Lilly, USA to assist with identification of individuals using U500R.
The newer concentrated insulins must develop measures to overcome the administration challenges due to large doses of 100units/mL or with use of the U500R. Manufacturers may follow the examples of Novo Nordisk A/S, whose IDegU200 is approved by the European Medical Agency (EMA), or Sanofi, who submitted IGlarU300 for approval by the EMA and the Food and Drug Administration (FDA), only as prefilled pen devices.29,30 In addition, the dose-counter window for IDegU200 displays doses in actual units, and each click is equivalent to a 2-unit increase in dose. 29 As the pen device for IGlarU300 has not yet been approved by either the FDA or EMA, the increments at which the dose will be indicated in the device that will be available to patients is not yet known. Limiting availability to prefilled pens and dosing in actual units eliminates errors from calculating dose conversions, as well as the use of devices not calibrated for the concentration of the solution.
Use via Continuous Subcutaneous Insulin Infusion (CSII)
The availability of concentrated insulins from vials allow for the transfer of that insulin into the reservoir of an insulin pump. In addition, use of concentrated insulins may allow for the development of devices with smaller reservoirs. The use of U500R for CSII has been evaluated through small retrospective and 1 prospective study, as well as a few case reports.31,35-45 The glycemic, weight, and insulin dose changes from the studies were discussed in a recent meta-analysis. 19 The determination for use of concentrated insulin via CSII include a total daily dose greater than 200 units with persistent suboptimal glycemic control, good adherence to current insulin regimen, and, if not currently using CSII, the ability and willingness to perform frequent self-monitoring glucose, ability to learn and understand the complexity of insulin pump use, financial capability to afford insulin pump therapy, and, if currently using CSII, requirement of daily reservoir changes.35-37
None of the pumps for CSII are calibrated for dosing concentrated insulin. Errors can occur when determining and converting doses. For U500R, doses, rates and ratios may be converted by either dividing or multiplying by 5.31,35,38,39 Delays in meals, accidental administration during pump priming, stacking of boluses due to snacking, and lack of a decrease in dose when not eating or during hospitalization are associated with episodes of hypoglycemia.36,38,40,41 To minimize or eliminate these episodes, use the insulin on board function and avoid correction doses at bedtime.
To avoid the dosage conversion challenges with multiple daily injections, newer products may not be available in vials. This limits the ability for these products to be used for CSII for future artificial pancreas devices. The exception may be BIOD-531, which demonstrated similar activity, with the exception of a faster onset of action, when compared to U500R administered to a swine via CSII and a 400 units/mL formulation of regular insulin being developed for intraperitoneal artificial pancreas devices (not discussed in this review).46,47 Whether the selective bolus profile concentrated insulins, lispro or Fluorolog will be available for CSII remains to be seen.
Cost
There are several ways to look at the cost of current concentrated treatment regimens. The first cost to discuss is the insulin itself. In the U.S. as most patients have medication coverage their cost is determined by the copay their coverage plan dictates. Interpretation of coverage is complex and differs widely between plans. Concentrated insulin is not always covered, leading to prior authorizations with higher copays or payment of percentages of retail price, which may be a significantly higher cost than the copay for insulin covered by the insurance. Reviewing retail costs from pharmacies across the U.S. and the average wholesale price (AWP), the cost of either concentration is almost equivalent ranging from $0.09 to $0.12 per unit of insulin.48,49 Thus, a patient may be asked to pay $540 to $720 (estimated for requirement of 200units/day) rather than a copay of $40 to $80 for a month supply.
Additional aspects contributing to the cost of current concentrated insulin regimens are the administration device, syringes or pump supplies. Cost per unit for current and new concentrated insulins, insurance coverage, the cost for the patients, and their perception of that cost and value based on their challenges with standard insulin regimens will impact their decision to pursue and adhere to concentrated insulin regimens.
Inpatient Usage of Concentrated Insulins
The availability of more concentrated forms of insulin represents another layer of complexity in maintaining safe insulin use practices in hospitals. Medication errors with insulin can lead to serious adverse events, some of which can unfortunately be fatal. 50 Inpatient use of concentrated insulin can cause significant confusion and anxiety at every step from ordering, to transcribing orders to dispensing and administering the insulin.51-53 Several publications offer suggestions for the development of systematic processes for concentrated insulin.5,54-56 As additional concentrated products become available, institutions need to reevaluate their processes to ensure safe and effective use for patients requiring these treatments.
Discussion
As stated, the new insulins may provide solutions to some of the challenges for patients requiring high doses. This review used available data to evaluate future concentrated insulins, with the restriction of some trials only reported as abstracts or press releases from pharmaceutical companies. We believe, based on what we have reviewed, the trials were properly designed and conducted. However, phase 3 trials have inherent limitations that practicing physician need to be aware of while interpreting data and making clinical decisions. 57 The phase 3 trials were short term, ranging from 6 to 12 months, designed to assess efficacy, using end points such as HbA1C. Long-term benefit and risks are partially but not fully assessed.
The change in weight differs within the prospective and retrospective studies with concentrated insulins.19-27 It is important for any practitioner and patient to understand when converting to a concentrated insulin regimen that if glycemic control was impaired prior to the conversion, the patient’s weight is likely to increase due to the decrease in caloric loss due to glycosuria with the prior regimen. This weight increase can range between 3% and 9%.58,59
The more flat profiles and hypoglycemia reduction, especially with nocturnal hypoglycemia, revealed in the new concentrated basal insulin trials is quite promising. However our general observations from these studies are that the methods of assessing hypoglycemia need more standardization. No clear guidelines exist for how a hypoglycemia event should be identified or method for analyses of products in clinical studies. Different methods and definitions for hypoglycemia are necessary when evaluating products with basal PD, from those used for products with a bolus PD profile. The variety of methods used within the EDITION and BEGIN LOW VOLUME studies cause additional layers of confusion for clinicians attempting to compare trial outcomes.
One of the main justifications for these new insulin formulations is more patient convenience via smaller volumes and less injections. However, if adherence was addressed in the trials discussed in this review, the data were not available.
Some aspects of these new insulins may prevent errors that have occurred with U500R. These include product identification errors by marketing the higher concentration under a different brand name as the 100 unit/mL product and decreasing dosing errors (both prescribing and administration) by using devices to administer doses using the actual units rather than using devices which require dose conversion calculations. Whether the new concentrated insulins will provide solutions to other challenges may have to wait for evaluation when the products arrive to market.
Footnotes
Abbreviations
AWP, average wholesale price; CSII, continuous subcutaneous insulin infusion; EDTA, ethylenediabminetetraacetic acid; EMA, European Medical Agency; ETD, estimated treatment difference; FDA, Food and Drug Administration; FPG, fasting plasma glucose; HbA1c, hemoglobin A1c; IDegU200, insulin degludec 200 units/mL; IDegU100, insulin degludec 100 units/mL; IGlarU300, insulin glargine 300 units/mL; IGlarU100, insulin glargine 100 units/mL; OAD, oral antidiabetic agents; PD, pharmacodynamics; PK, pharmacokinetics; SC, subcutaneous; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; U500R, regular insulin 500 units/mL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.