
Abstract
Background:
Galactomannan is an insoluble polysaccharide that has been shown to reduce postprandial excursions. We assessed the impact of a novel galactomannan derivative (PAZ320) on the magnitude of 2-hour postprandial glucose excursions in individuals with type 2 diabetes who were being treated with oral medication and/or insulin.
Methods:
Investigators recently reported findings from a single-center, open-label, prospective study that evaluated the efficacy of PAZ320 in 24 subjects with type 2 diabetes who were treated with oral antidiabetic agents and/or insulin. End points included adverse events and area under the curve during 3-hour postprandial glucose excursion (gAUC). Subjects consumed a test meal without PAZ320 at baseline and then ingested low-dose (8 g) and high-dose (16 g) PAZ320 with test meals at subsequent intervention visits. A post hoc analysis was conducted to determine changes in 2-hour postprandial glucose excursions.
Results:
Among the 20 subjects for whom data were available for all clinic visit test meals, 15 (75%) responded to low-dose, high-dose, or both medication dosages. Low-dose responders (n = 8) experienced clinically significant improvements in 2-hour postprandial glucose excursions from baseline excursions compared with nonresponders (–28.00 ± 25.97 mg/dL vs 23.42 ± 11.45 mg/dL, P = .005). Similar differences were seen in high-dose responders (–28.82 ± 24.26 vs 33.89 ± 20.56 mg/dL, P < .0001).
Conclusions:
PAZ320 was shown to be safe in all patients studied and effective in controlling postprandial glucose in a large portion of the study population. Additional studies are needed to determine its long-term effects on HbA1c and to further define which subpopulation(s) may respond to PAZ320 therapy.
Diminished first-phase insulin secretion and subsequent elevated postprandial glucose is well recognized as an early marker of beta-cell dysfunction.1-3 and may represent a primary genetic risk factor predisposing individuals to type 2 diabetes. 4 Emerging evidence suggests that excessive postprandial excursions may be a significant risk factor for both microvascular 5 and macrovascular disease.6-11
Galactomannan is an insoluble polysaccharide that has been shown to reduce postprandial excursions. PAZ320 (Boston Therapeutics, Inc, Manchester, NH, USA) is a nonsystemic chewable complex carbohydrate-based compound derived from galactomannan that reduces postprandial glucose excursions and increases satiety. 12
Using a single-center, open-label, sequential dose-escalation, prospective study design, Trask and colleagues evaluated the efficacy of PAZ320 in 24 subjects with type 2 diabetes who were treated with oral antidiabetic agents and/or insulin. 12 End points included adverse events and area under the curve during 3-hour postprandial glucose excursion (gAUC). 12 Subjects consumed a test meal without PAZ320 at the first intervention visit to obtain baseline values, and then ingested low-dose (8 g) and high-dose (16 g) PAZ320 with test meals at subsequent intervention visits. 12 Investigators found PAZ320 to be safe and well tolerated with no increase in hypoglycemia. Flatulence was the most common side effect, but was generally described as “mild” when reported by subjects. 12 Efficacy of treatment with PAZ320, however, was not consistent for all 3 intervention visits. Although 9 (47%) subjects showed significant reductions in 3-hour postprandial gAUC (P = .012), postprandial glucose control significantly worsened from baseline in the remaining 10 (53%) subjects (P = .014). Additional studies are underway to identify the diabetic population(s) most likely to respond positively to PAZ320 therapy.
For the current study, we conducted a post hoc analysis of data from the Trask et al study 12 to assess the magnitude of 2-hour postprandial glucose excursions.
Methods
Subjects
Details of the study design and intervention have been published elsewhere. 12 In brief, subjects were recruited from the Dartmouth-Hitchcock Medical Center in Lebanon, New Hampshire. The first subject entered the study in September 2011; the last subject completed follow-up in May 2012. The study protocol was approved by the Committee for the Protection of Human Subjects (institutional review board) and was in compliance with the Declaration of Helsinki. 13
Inclusion criteria were as follows: male or female; aged 18 to 75 years; diagnosed with type 2 diabetes mellitus; currently treated with oral/injectable agents or insulin; HbA1c ≤ 9%; BMI 25-45 kg/m2; able to comply with study procedures; and willing to sign informed consent. Exclusion criteria were as follows: treated with medication (other than diabetes medications or insulin) or dietary supplement known to affect glucose or galactose metabolism; use of acetaminophen-containing products; lactose or galactose intolerance; history of eating disorder; food allergy or severe food intolerance; pregnant or lactating female; treated with very high dosages of sulfonylureas (glyburide > 20 mg/day, glimepiride > 8 mg per day, and glipizide > 20 mg per day) α-glucosidase inhibitors (acarbose), or meglitinides (repaglinide >6 mg per day); gastrointestinal disease that may interfere with absorption of the investigational products at discretion of investigator, including but are not limited to malabsorption syndromes and gastric ulcer; treated with any investigational agent within 30 days prior to the first dose of investigational agent.
Study Medication
The study medication, PAZ320, is derived from galactomannan and acts by blocking key carbohydrate hydrolyzing enzymes such as glucosidase, amylase, maltase, lactase, and sucrase in the gastrointestinal tract. It also acts to bind to ingested polysaccharides and slow their absorption with each meal, thereby reducing the postprandial glucose excursion. Ingestion of PAZ320 generally increases satiety and may cause gastrointestinal related side effects including flatulence and bloating. PAZ320 was supplied as a tasteless, chewable oral tablet, 4 grams per tablet. Low-dosage treatment included 8 g PAZ320 (2 chewable tablets) administered orally 10 minutes prior to meal ingestion. High-dosage treatment included 16 g PAZ320 (4 chewable tablets) administered orally 10 minutes prior to meal ingestion.
Procedures
Subjects attended 4 clinic visits: visit 1 (baseline), visit 2 (control meal), visit 3 (low-dose intervention), and visit 4 (high-dose intervention). Visits 2, 3, and 4 were conducted within a 7-day period. At the baseline visit, investigators confirmed subject eligibility, obtained signed written informed consent, verified demographic information and obtained medical history. Subjects were instructed to administer usual medications and fast for 10 hours prior to visit 2. At visit 2, investigators attached a continuous glucose monitoring (CGM) device (Dexcom SEVEN PLUS, Dexcom, Inc, San Diego, CA, USA) in the blinded mode according to manufacturer instructions. After the CGM was in place for 2 hours, 2 fingerstick glucoses were checked for calibration. Subjects then consumed a control meal that consisted of 75 g (dry weight, 60 grams carbohydrate) of cooked jasmine rice (White Gold brand). At visits 3 and 4, subjects ingested a PAZ320 followed by the control meal; low dosage (8 g) was administered at visit 3 and high dosage (16 g) was administered at visit 4. Questionnaires to document any adverse drug reactions were administered at visits 2, 3, and 4.
Measures
Changes in 2-hour postprandial interstitial glucose excursions were assessed using CGM data from the clinic visits (visits 2, 3, and 4). Responder was defined as any subject who showed improvement in magnitude of 2-hour postprandial glucose excursions at low (visit 3) and/or high (visit 4) PAZ320 dosages compared with his or her 2-hour postprandial glucose excursion at visit 2.
Statistical Analysis
For each subject, the 2-hour postprandial excursion was computed for the in-clinic meal at each visit by subtracting the baseline glucose level from the 2-hour glucose level. A subject was classified as a responder, at that visit, if the 2-hour glucose was lower than baseline (a negative difference). For each visit, the subjects were divided into responders and nonresponders. A standard 2-sample t test was used to compare mean difference between responders and nonresponders at each visit and overall. Satterthwaite’s correction was used if the standard deviations of the 2 groups were significantly different (P = .05). If the resulting P value of the t test was less than .05, then the responders and nonresponders were declared statistically significantly different. A Fisher’s exact test was used to determine if adverse events were associated with an intervention. A logistic model was used to determine if any adverse event was associated with a group (responder or nonresponder). The statistical analyses were reported using summary tables. All statistical testing was 2-sided and was performed at the .05 significance level unless otherwise noted. Tests were declared statistically significant if the calculated P value was ≤.05. Continuous variables were summarized with means, standard deviations, medians, minimums, and maximums. All statistical tests were done using Stata (version 8, College Station, TX) or SAS version 9.2 (Cary, NC).
Results
Subject Disposition
Twenty-four subjects were screened, met eligibility criteria, and provided signed informed consent forms. Among these, 22 subjects completed the study; 1 subject was discontinued following the baseline visit due to unwillingness to attend subsequent clinic visits, another subject voluntarily withdrew from the study following visit 3, and 2 subjects were excluded from the analysis because glucose values were not available at 1 or more of the clinic visits. Demographic characteristics of the 20 subjects included in this analysis were 55% male, mean (SD) age 59 (9.8) years, mean duration of diagnosed type 2 diabetes 10 (6.4) years, mean HbA1c 7.5% (0.7), and mean BMI 33 (5.5) kg/m2.
Magnitude of 2-Hour Postprandial Glucose Excursions
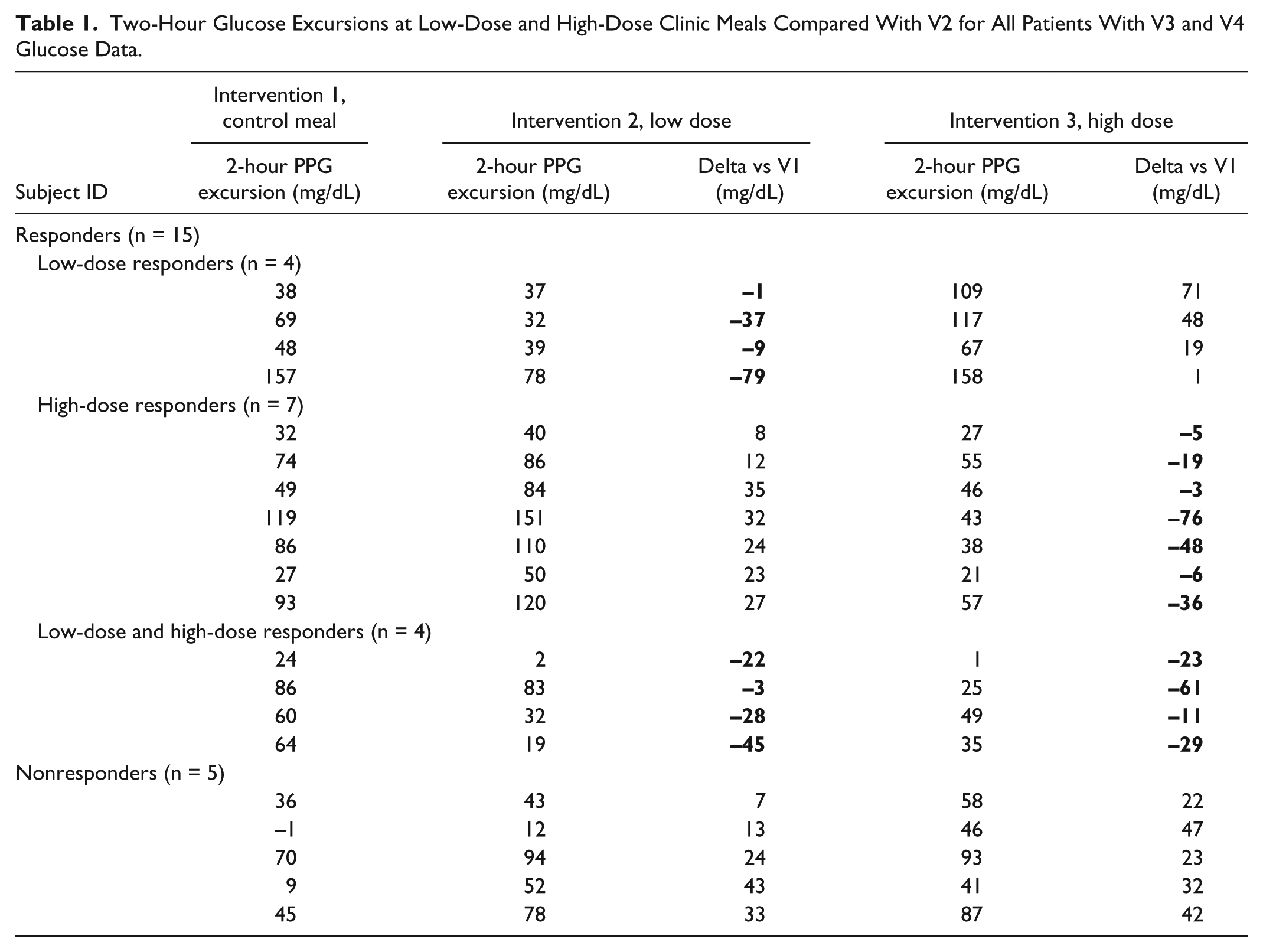
Among the 20 subjects for whom 2-hour postprandial glucose excursion data were available for all clinic test meals at visits 2, 3, and 4. Fifteen (75.0%) subjects responded to therapy: low-dose therapy only (n = 4, 20.0%), high-dose therapy only (n = 7, 35.0%), or low- and high-dose therapy (n = 4, 20%; Table 1).
Two-Hour Glucose Excursions at Low-Dose and High-Dose Clinic Meals Compared With V2 for All Patients With V3 and V4 Glucose Data.
As shown in Table 2, many subjects who responded to low-dose therapy (n = 8) experienced clinically significant reductions in 2-hour postprandial glucose excursions (–28.00 ± 25.97 mg/dL) compared to baseline (visit 2) excursions. Conversely, subjects who did not respond to low-dose therapy (n = 13) experienced clinically significant increases in 2-hour glucose excursions (23.42 ± 11.45 mg/dL). Similar differences were seen between high-dose responders and nonresponders. There were no differences between responders and nonresponders in gender, baseline HbA1c, or medication regimens. However, responders were older than nonresponders (57.6 vs 53.9 years) had slightly longer duration of diabetes (11.3 vs 10.7 years) and experienced greater 2-hour postprandial glucose excursions at baseline (V2) than nonresponders: 75.0 versus 29.9 mg/dL. These differences were not statistically significant, which is likely due to the small sample size.
Change in 2-Hour Postprandial Glucose Excursions Compared With Baseline.
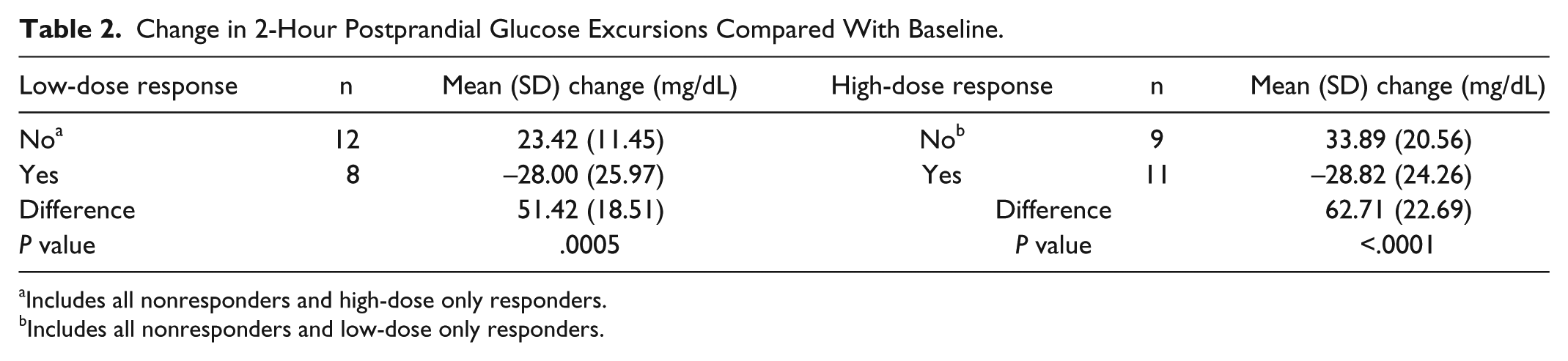
Includes all nonresponders and high-dose only responders.
Includes all nonresponders and low-dose only responders.
Discussion
Treatment with PAZ320 was shown to be efficacious in controlling postprandial glucose in a large majority of study subjects. Emerging evidence suggests that excessive postprandial excursions may be a significant risk factor for both microvascular 5 and macrovascular disease.6-11
Several limitations of the study must be acknowledged. PAZ320 was only given for a short time and 2-hour postprandial glucose excursions were analyzed for only a single carbohydrate-alone meal. Due to the short duration of the study, there are no data on changes in subjects’ subsequent HbA1c, which often requires 6 months of evaluation. In addition, the heterogeneity of diabetes treatment regimens within the study population confounds our ability to discern the cause(s) of the significant differences in glycemic response.
Interestingly, the responders and nonresponders had a significantly different response to the control meal alone; the average postprandial glucose excursion after eating the control meal at baseline was significantly higher for responders compared to nonresponders. Because no meaningful between-group differences were seen in diabetes treatments, this finding suggests that nonresponders had a more robust first-phase insulin response than responders. This is supported by the apparent differences in age and diabetes duration between the groups. As discussed previously, responders were significantly older than nonresponders. Moreover, although the documented between-group difference in diabetes duration was small, it is known that, in many individuals, the diagnosis of type 2 diabetes may occur several years subsequent to the actual manifestation of the disease. As reported earlier by Harris and colleagues, type 2 diabetes is often present for up to 12 years prior to diagnosis. 14 Thus, the differences in age and, likely, duration of diabetes may have played a role in the differences in treatment response.
Although the reason(s) behind the paradoxical glucose responses seen in study subjects remains unknown, our findings underscore the need for clinicians to persistently monitor their patients’ therapies, including use of over-the-counter medications and dietary supplements, given that approximately 25% of subjects experienced greater postprandial glucose excursions with PAZ320 treatment. Nevertheless, our findings show that PAZ320 treatment is beneficial in large majority of the subjects studied in reducing 2-hour postprandial glucose excursions. Fortunately, responders can be quickly identified by monitoring 2-hour postprandial glucose levels during the first few days of PAZ320 therapy. Patients who are not responsive to treatment can be transitioned to more effective therapy with minimal delay. This ability to quickly identify negative responders not only reduces exposure to significant postprandial hyperglycemia but facilitates improved quality of care. A recent study showed that early initiation, persistent monitoring, and timely adjustment of therapy significantly improve glycemic control in individuals with poorly controlled, non-insulin-treated type 2 diabetes. 15
Conclusions
In summary, our findings showed that treatment with PAZ320 was safe in all patients studied and effective in controlling postprandial glucose in a large portion of our study population. Further study is required to better define which subpopulation(s) may respond to PAZ320 therapy and determine its long-term effects on HbA1c.
Footnotes
Acknowledgements
The authors would like to thank Yael Bobruff, PhD, Boston Therapeutics, Inc, for assistance in coordination of data and manuscript development, and Patrick D. O’Meara, PhD, Pat O’Meara Associates, Inc, Lincoln, NE, USA, for statistical analysis support. Results from the primary analysis of this study were published in Endocrine Practice. 12
Abbreviations
BMI, body mass index; gAUC, glucose area under the curve; HbA1c, hemoglobin A1c; mg/dL, milligram per deciliter.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LET and SSC report no relevant financial conflicts of interest. DP is an employee of Boston Therapeutics, Inc. CGP has received consulting fees from Boston Therapeutics, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the study was provided by Boston Therapeutics, Inc, Manchester, NH, USA and Advance Pharmaceutical Co, Ltd, Hong Kong, China.