
Abstract

Although postprandial glucose exposure contributes significantly to the overall glycemic load, especially in patients with relatively good glucose control, affects the glycemia risk index (GRI) and glucose variability,1,2 and is an independent cardiovascular (CV) risk factor, 3 it was not included in the 2019 Consensus among the most useful continuous glucose monitoring (CGM)-derived parameters for routine clinical practice. 4 Postprandial glucose excursion (PPGE) can be calculated from CGM tracing as the area under the curve (AUC) spanning from the time preceding the meal and ending 2 hours after the start of the meal; it evaluates not only glucose peak intensity but also amplitude and duration. 5 Advanced hybrid closed loop (AHCL) systems are more efficient in improving glucose control than conventional insulin pumps. 6 This improvement is recognized very early after the start of the therapy. 7 However, there are few data on the effect of these automated insulin devices on PPGE control. The aim of this study was to evaluate the effect of switching from the manual mode of Sensor Augmented Pump (SAP) Medtronic 670 to the Medtronic 780G AHCL system (automated “Smartguard” model) on PPGE (represented by AUC) in type 1 diabetes (T1D) subjects. The second endpoint was the evaluation of CGM metrics, metabolic and clinical parameters before and after the switching, as well as treatment satisfaction. Fifteen T1D patients (80% males, age 51 ± 12.79 years, disease duration 24 ± 15.48 years) using SAP Medtronic 670 in manual mode for at least 5 years who started with the 780G AHCL system were studied. Average breakfast, lunch, and dinner AUC was calculated for 15 consecutive days before the switching (T0), first 2 weeks after switching (T1), and 2 weeks after 3 months of use (T2). Data about total daily dose (TDD), time above/below/in range (TAR, TBR, TIR), GRI, body mass index (BMI), glycosylated hemoglobin (A1c), lipid profile, and Diabetes Treatment Satisfaction Questionnaire (DTSQ) 8 were considered. A significant reduction in AUC was observed for breakfast and dinner at T2 and for lunch and dinner at T1 (Table 1). TIR increased (Table 1), while TAR, TBR, and GRI (Table 1) reduced significantly from T0 to T1 and T2. We did not observe statistically significant differences for A1c, BMI, and plasma lipids. A significant TDD increase was observed at T2 (from 39.81 units/day at T0 to 46.04 units/day at T2; P < .05), due to the increase of automatically delivered correction boluses. DTSQ score at T2 was 33 (median value, interquartile range 32-34, maximum 36).
Mean AUC of the Three Meals and data about Time in Range and Glycemia Risk Index.
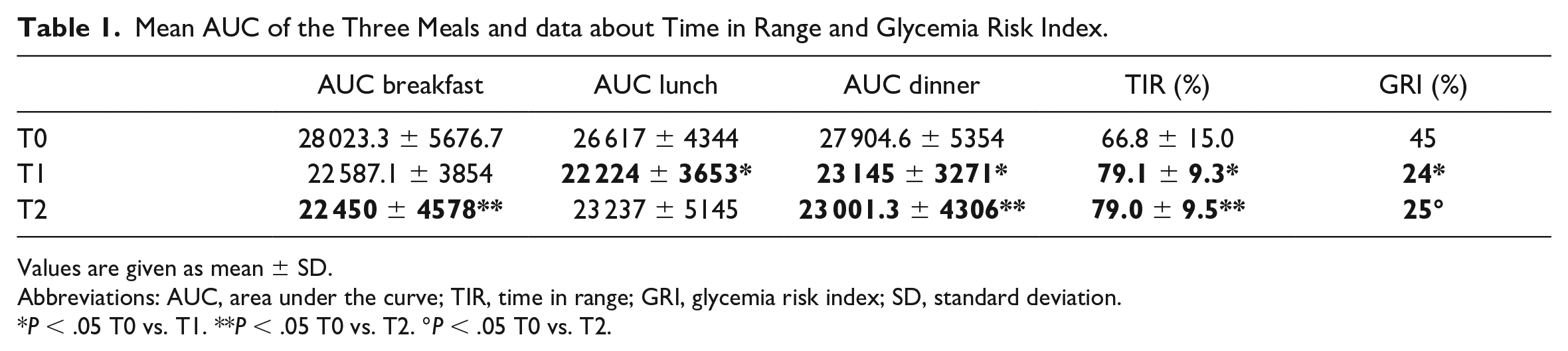
Values are given as mean ± SD.
Abbreviations: AUC, area under the curve; TIR, time in range; GRI, glycemia risk index; SD, standard deviation.
P < .05 T0 vs. T1. **P < .05 T0 vs. T2. °P < .05 T0 vs. T2.
Switching to the 780G AHCL system decreased PPGE rapidly by increasing the automated insulin correction dose without weight gain. Probably this kind of algorithm is more efficient in PPGE control as it can overcome carbohydrate (CHO) counting mistakes, the inability to recognize glycemic index, food processing, and other mixed meal nutrients (fat, protein, fibers). Meal management simplification and glucose control improvement were associated with high user satisfaction scores. Furthermore, our data suggest to consider AUC as a PPGE-related independent glucose metric, useful to underline specifically the impact of dietary choices on glucose profile, and to verify the efficacy of educational therapy and the implementation of healthy dietary habits.
Footnotes
Abbreviations
AHCL, advanced hybrid closed loops; AUC, area under the curve; A1c, glycosylated hemoglobin; BMI, body mass index; CGM, continuous glucose monitoring; CHO, carbohydrate; CV, cardiovascular; DTSQ, Diabetes Treatment Satisfaction Questionnaire; GRI, glycemia risk index; PPGE, postprandial glucose excursion; SAP, Sensor Augmented Pump; TAR, time above range; TBR, time below range; TDD, total insulin daily dose; TIR, time in range; T1D, type 1 diabetes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written permission was obtained from Prof. Ohad Cohen and Dr. Vittorino Smaniotto.