
Abstract
Background:
In the setting of Meaningful Use laws and professional society guidelines, hospitals are rapidly implementing electronic glycemic management order sets. There are a number of best practices established in the literature for glycemic management protocols and programs. We believe that this is the first published account of the detailed steps to be taken to design, implement, and optimize glycemic management protocols in a commercial computerized provider order entry (CPOE) system.
Process:
Prior to CPOE implementation, our hospital already had a mature glycemic management program. To transition to CPOE, we underwent the following 4 steps: (1) preparation and requirements gathering, (2) design and build, (3) implementation and dissemination, and (4) optimization. These steps required more than 2 years of coordinated work between physicians, nurses, pharmacists, and programmers. With the move to CPOE, our complex glycemic management order sets were successfully implemented without any significant interruptions in care. With feedback from users, we have continued to refine the order sets, and this remains an ongoing process.
Conclusions:
Successful implementation of glycemic management protocols in CPOE is dependent on broad stakeholder input and buy-in. When using a commercial CPOE system, there may be limitations of the system, necessitating workarounds. There should be an upfront plan to apply resources for continuous process improvement and optimization after implementation.
Implementing a physiologically based computerized provider order entry (CPOE) glycemic management program into the inpatient setting can be challenging for a health care organization. Beginning with a 2006 task force, the American Diabetes Association (ADA) and American College of Endocrinology (ACE) recommended that hospitals develop comprehensive inpatient glycemic management programs. 1 By 2008, 21% of hospitals had fully implemented protocols for noncritically ill patients, and 39% had done so for critically ill patients. 2 A few years later, in February 2009, the United States government enacted the Health Information Technology for Economic and Clinical Health (HITECH) Act, which through its Meaningful Use program laid out a series of financial incentives (and ultimately financial penalties) to encourage health care organizations to implement electronic health record (EHR) systems, including CPOE.3,4
Even before CPOE, establishing a comprehensive inpatient glycemic management system required years of planning; significant education and coordination of medical, nursing, dietary, and pharmacy staff; and support from hospital administration and quality improvement departments. Transitioning this work into CPOE requires a similar effort as well as the coordination of the above disciplines with informaticists and EHR analysts. The implementation of such a major change into a health care organization requires incorporating the following processes: preparation and requirements gathering, design and build, validation and testing, education, implementation and dissemination, and optimization.
Several institutions have previously published their experiences toward creating a unified, comprehensive inpatient glycemic management program, including experiences with both homegrown and commercial CPOE systems.5-10 Although the benefits of CPOE for glycemic management have been discussed,6,7 to date, there has not been a published comprehensive and detailed description of all the steps required for a successful transition to CPOE.
In this article, we describe our institution’s experience and challenges over a 2-year period in transitioning our paper-based comprehensive inpatient glycemic management program to CPOE-based insulin order sets for glycemic management.
Insulin Management Before CPOE
In the 1990s, at one of the hospitals at our medical center, we established the mandatory use of specific paper-based insulin order sets for all subcutaneous (SQ) and intravenous (IV) insulin use and for diabetic ketoacidosis (DKA). By 2004, all inpatient insulin orders for the entire medical center were required to be written using our preprinted insulin order forms. Nursing staff was educated on the use of these orders with mandatory, interactive Internet-based training. Pharmacists were oriented on the verification steps required to authorize the orders. Internet training for using these order sets was available for providers but was not mandatory. All medical and surgical interns had mandatory case-based training in small groups. While there were initially 4 order sets (for SQ insulin infusion, intensive care unit [ICU] IV insulin infusion, medical-surgical IV insulin infusion, and DKA), over time, this increased to 13 distinct paper order forms (Table 1).
Paper Insulin Order Forms Prior to CPOE Implementation.
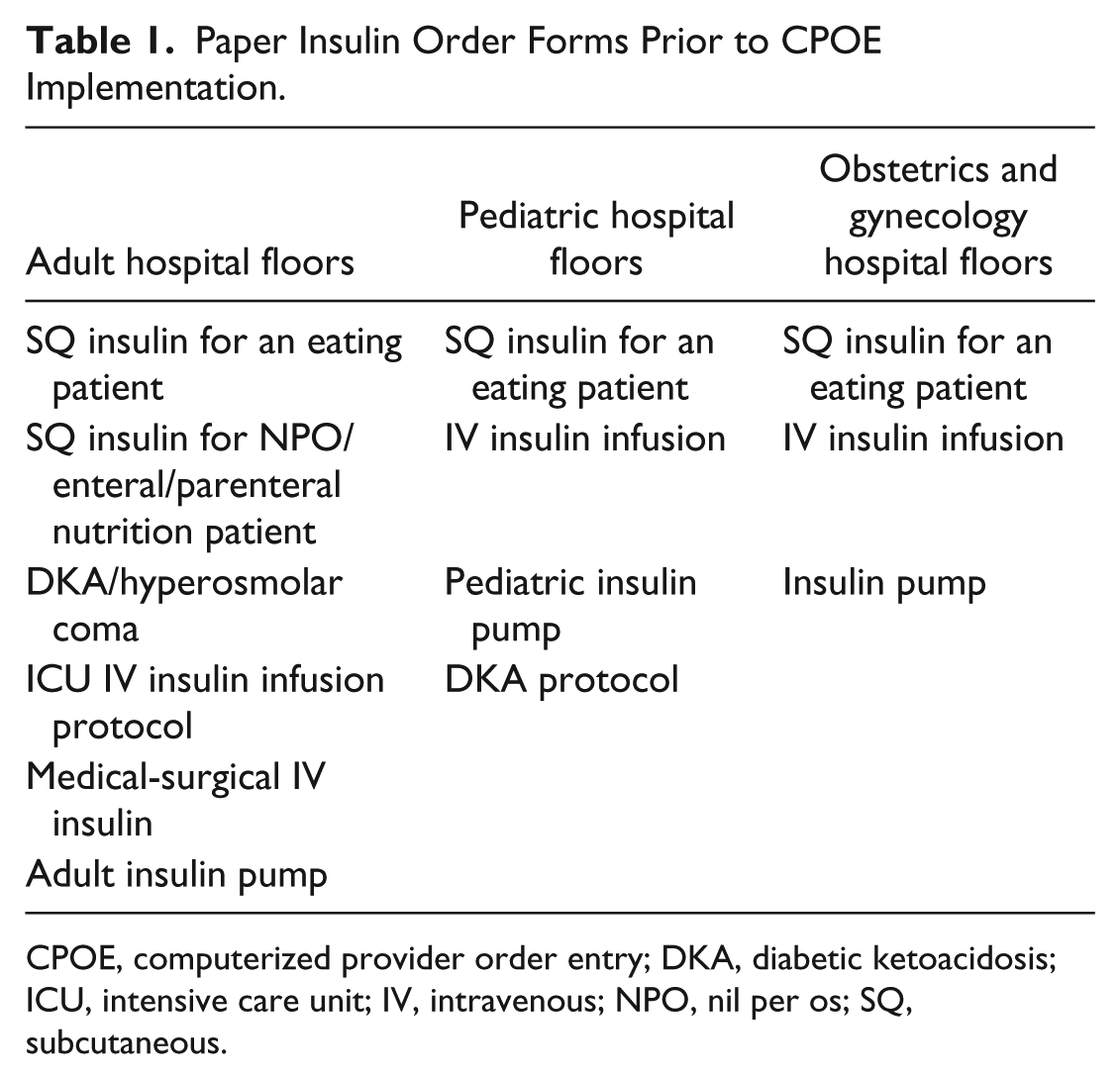
CPOE, computerized provider order entry; DKA, diabetic ketoacidosis; ICU, intensive care unit; IV, intravenous; NPO, nil per os; SQ, subcutaneous.
Since 2003, we have had an inpatient glucose management committee comprising adult and pediatric endocrinologists, hospitalists, obstetricians, house staff, a diabetes nurse specialist, pharmacists, a risk management nurse, dietitians, and staff nurses from both pediatric and adult acute and critical care. This committee was involved in all aspects of inpatient glycemic management, developing the insulin order forms, monitoring glucometrics, and performing audits for insulin-related errors and adverse events. We performed a glucometric analysis in 2006 and found that after the implementation of paper insulin order sets, the mean glucose level for ICU patients on SQ insulin decreased from approximately 260 mg/dL to 155 mg/dL, with a <0.4% rate of glucose under 40 mg/dL. There were similar improvements in non-ICU patients.
Our practices on paper adhered to many best practices for inpatient glycemic management. Some examples include having distinct order sets for specific clinical scenarios (ie, indication-based order sets), a restricted hospital formulary, defaulted nursing instructions (eg, to hold nutritional insulin dosing when food is held), nursing education and in-services, matching the timing of fingerstick glucose checks to meal times and insulin delivery, and having a hospital inpatient diabetes committee. 11
In 2010, our institution began the process of implementing a new EHR (EpicCare, Epic System, Verona, WI) with the goal of completing implementation in all inpatient and ambulatory areas by June 2012. We quickly discovered that attempting a literal translation of paper order forms into CPOE does not work. For example, with paper order forms, a provider can alter the preprinted orders by crossing something out or writing something in. This almost infinite degree of flexibility is not possible with CPOE, in which the order set must be designed to support all likely orders, and there must be some method for a provider to place more rare orders.
Step 1: Preparation and Requirements Gathering
Fortunately, because we had already assembled an inpatient glucose management committee with broad representation, building our team did not occur from scratch. New to our team and leading our work were a clinical pharmacist and clinical informaticist trained in developing and customizing order sets for our EHR. He was joined by a clinical pharmacist and nurses trained in our EHR system who understood the ways in which the orders would translate into administration instructions. This work was overseen by a new hospital committee repurposed from managing the development of all paper order sets and now in charge of all CPOE order sets.
Our primary design objectives for glycemic management order sets for CPOE were to make them: (1) physiological (ie, basal-bolus insulin rather than sliding scale); (2) consistent with our formulary; (3) comprehensive in containing insulin orders, hypoglycemia protocol orders, prescribing guidelines, and clear administration instructions; and (4) contain safeguards to decrease potential errors at the time of order entry, verification, or administration. We first assessed the vendor-provided sample insulin order sets and found that they did not support our needs. We contacted several institutions using the same EHR and also found that they were either in the process of developing customized order sets or had built order sets that also did not meet our objectives.
Step 2: Design and Build
Initially, 2 of us (R.R., M.M.S.) who had been involved in the development of all the paper order sets met with the informaticist (A.N.) tasked with aiding the transition from paper insulin order sets to CPOE. Through the course of 3 meetings and dozens of emails back and forth, the paper order sets were translated into spreadsheets to help visualize the hierarchy of orders and which orders were required or defaulted. An example is shown in Figure 1. This presented the opportunity to make key improvements from paper order sets, such as adding orders that matched the timing of insulin dosing with cycled enteral or parenteral nutrition or adding carbohydrate (CHO)–based SQ insulin administration options.
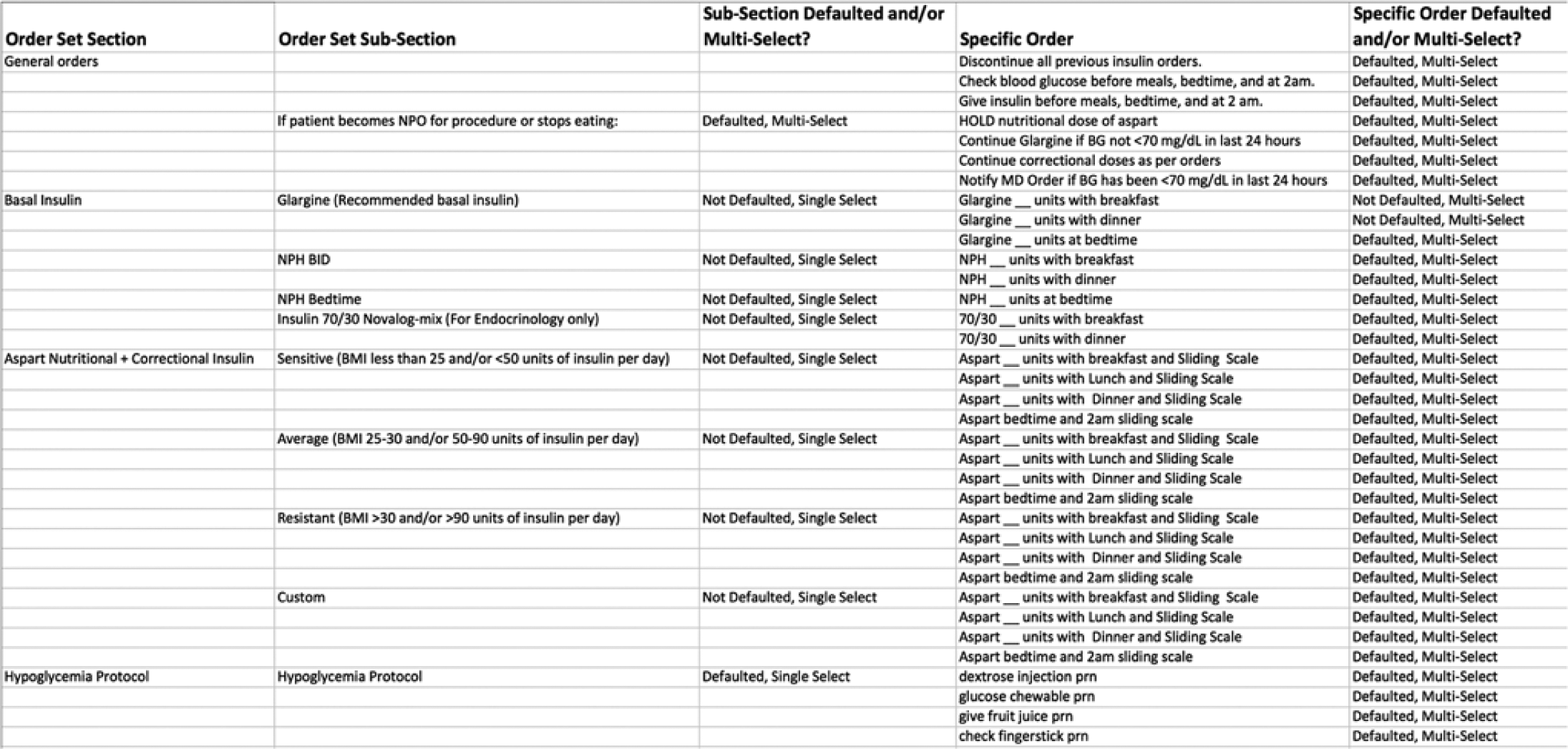
Spreadsheet translating paper orders into electronic orders. This spreadsheet shows our “work in progress” translation of paper order forms into a format that could be built into computerized provider order entry order sets.
The initial design of the new CPOE order sets was based on these detailed spreadsheets, and over the subsequent 3 months, the layout of the various insulin order sets was established. Our goal was to standardize the layout and functions of the many different order sets.
We quickly encountered challenges. As with most institutions, our paper SQ insulin order set requested a dose for nutritional insulin and then a selection from a separate correctional dose table to help the nurse calculate the total premeal insulin dose that the patient should receive (Figure 2).
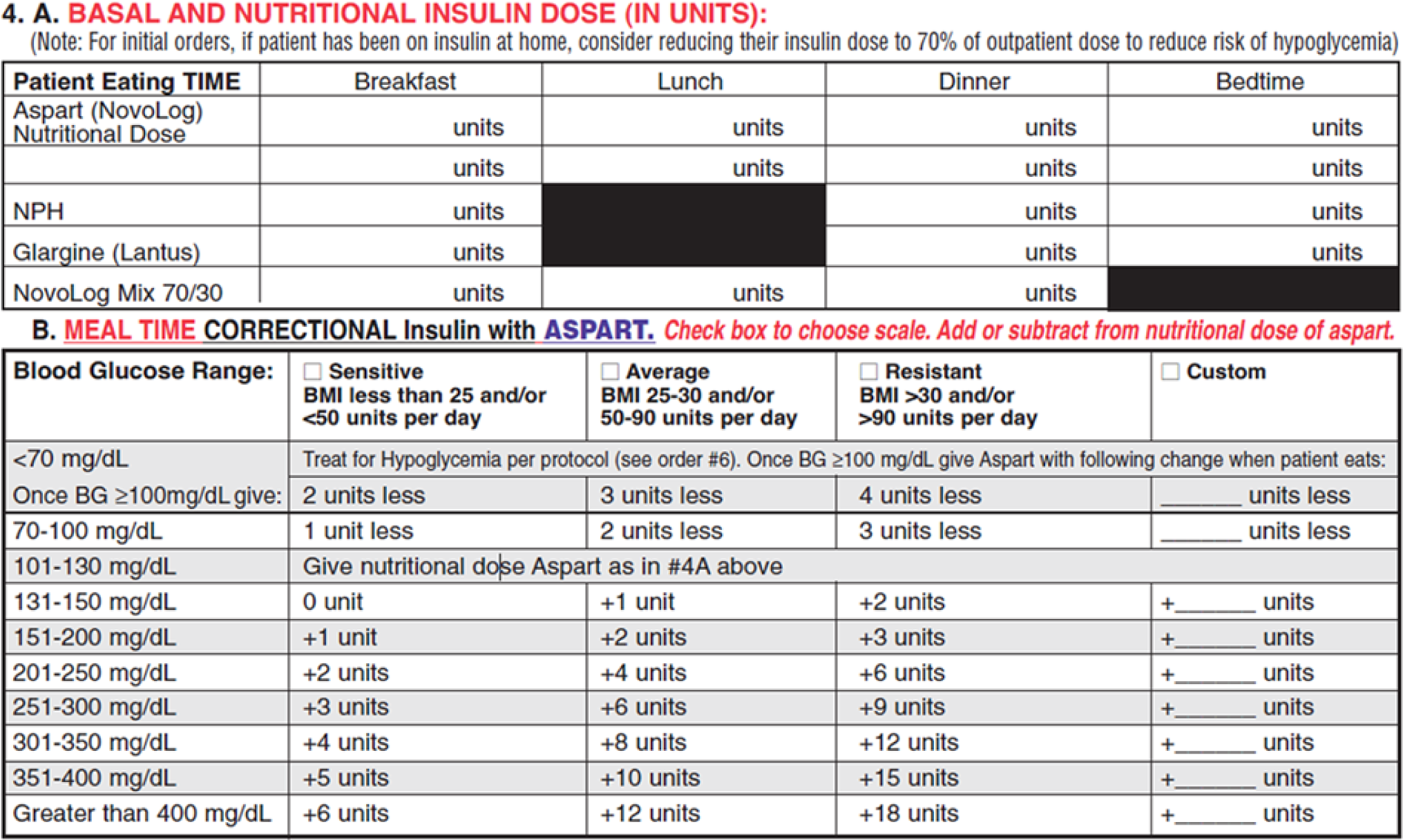
Paper insulin order set.
With our CPOE system, separate orders for nutritional and correctional insulin doses would display separately on the medication administration record [MAR], potentially far apart from each other on a nursing administration screen. We learned from other institutions that this could result in mathematical errors, duplicated injections, or omission of either the nutritional or correctional insulin dose. To avoid this, we decided to group together the nutritional and correctional insulin orders as 1 insulin order (Figure 3).
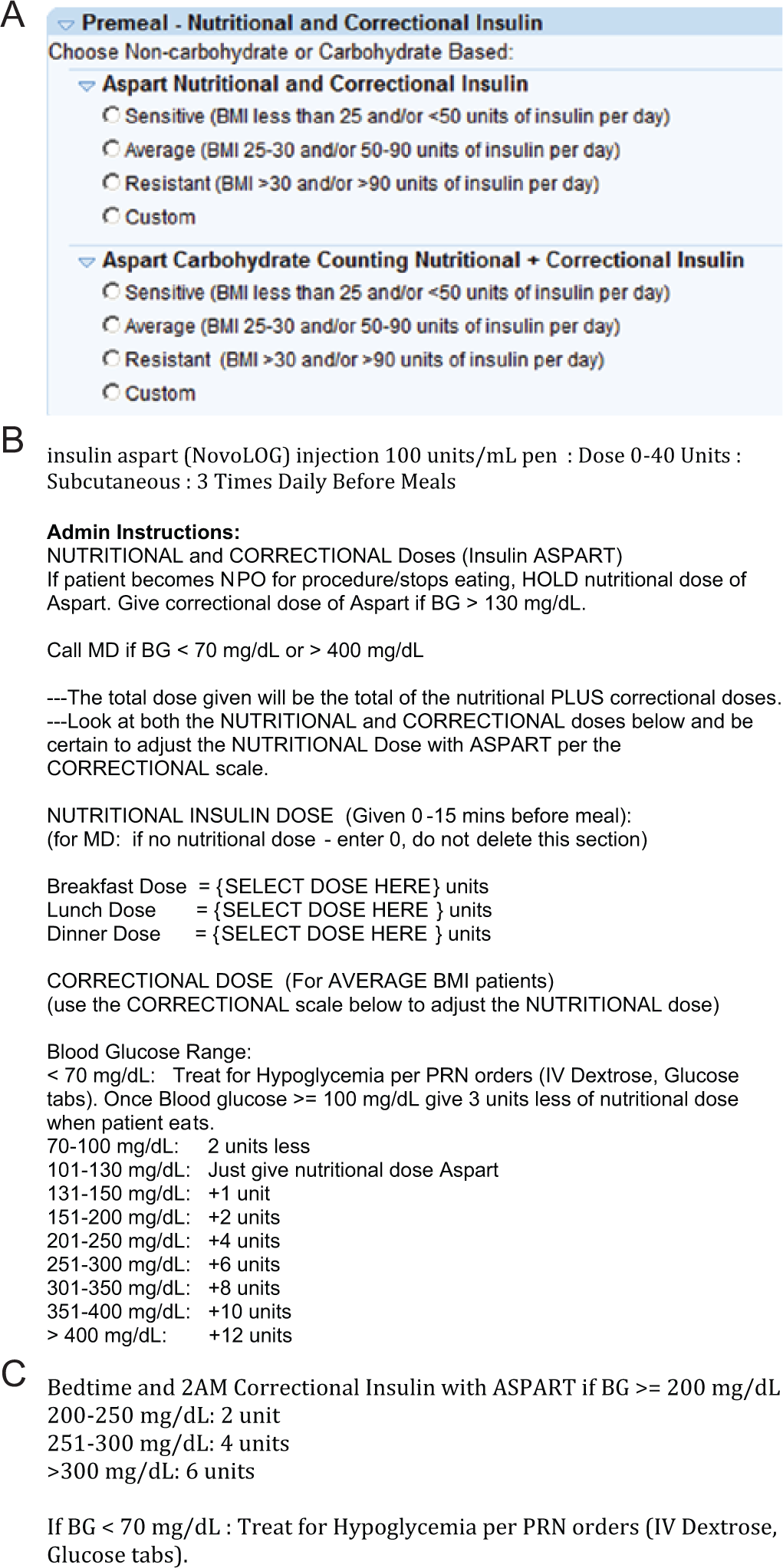
(A) Combined nutritional and correctional insulin order in computerized provider order entry (collapsed for initial order selection). (B) Administration instructions after selecting a combined nutritional and correctional insulin order in A (average scale). (C) Administration instructions after selecting a combined nutritional and correctional insulin order in A: bedtime and 2
Thus, on all SQ insulin order sets, the first step for the prescribing provider would be to choose a rapid-acting insulin based on whether the patient would require a sensitive, average, resistant, or custom correctional dose. Once making that choice, the nutritional insulin dose could be entered into the administration instructions. This workflow also served as embedded decision support, forcing providers to actively order zero units if no nutritional insulin dose was to be given, as opposed to just using “sliding scale” insulin.
One item of note is that the design and functional possibilities may vary greatly between different commercial EHRs. For example, as described in a prior article, 12 the usability principle of “natural mapping,” or laying out an electronic system to match a person’s mental model, was impossible to adhere to in designing insulin order sets in our CPOE system. It was not possible to design our order sets to make use of a tabular format, something that would be self-obvious and familiar to users because this is the conventional way to display insulin plans and the way that was used in our prior paper order forms.
Another issue that we encountered was how to handle changes in insulin orders, for example, changes in a nutritional insulin dose or for a patient transitioning from IV to SQ insulin. On paper, we had mandated that the provider fill out a completely new order set for any change, reducing the risk for duplicate orders. However, with CPOE, having to delete and re-enter a completely new order set seemed inefficient, so our team decided that we would allow modifications to the initial insulin order set. To help with transitioning from IV to SQ insulin, we embedded an SQ insulin dose in the IV infusion order sets.
Although the insulin sections of every order set were developed to specifically match the clinical state of the patient (eg, eating or nil per os [NPO]), all other sections of the order sets were standardized (Figure 4). A nursing orders section included the timing and restrictions for glucose monitoring for a predefined time standard (eg, premeal, bedtime, and 2
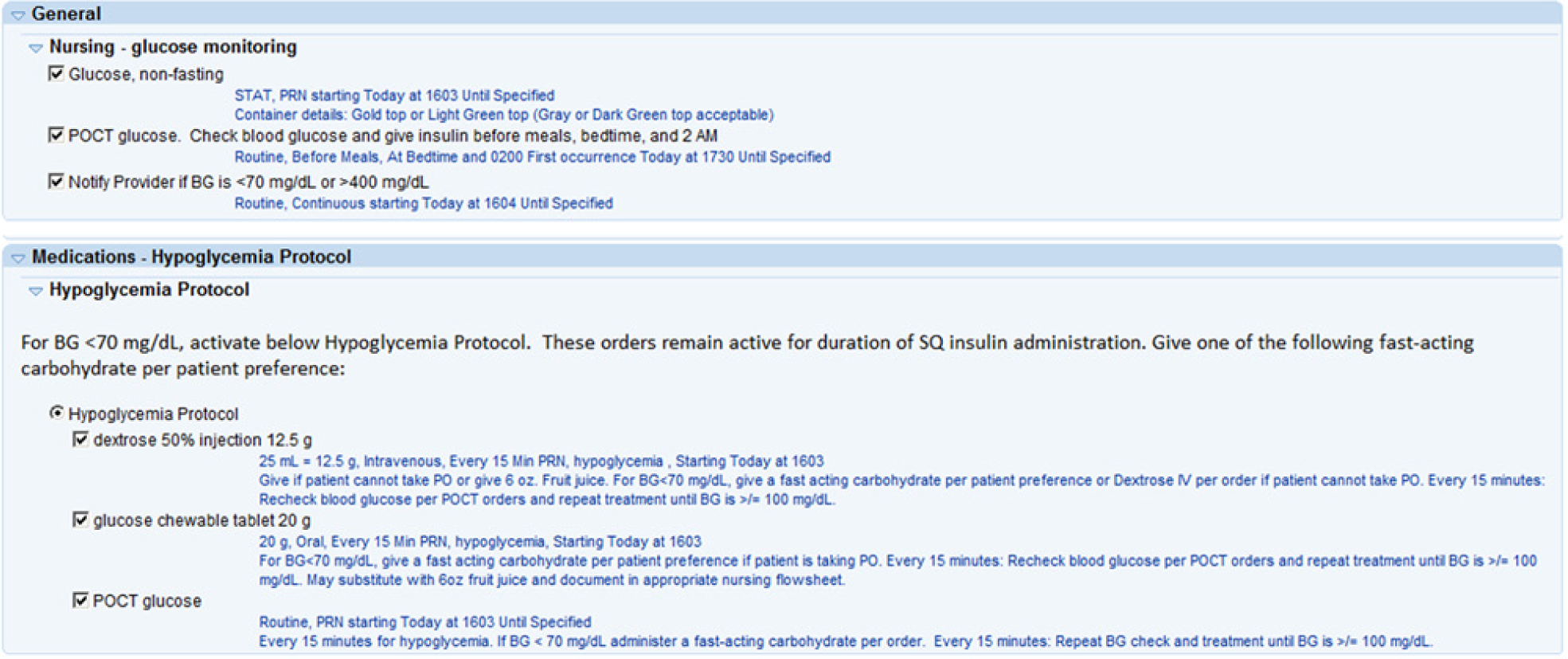
Defaulted nursing and hypoglycemia protocol orders. Every glycemic management order set was built with preselected orders to standardize nursing care and hypoglycemia protocol orders.
As shown in Table 2, we built multiple insulin order sets. Other institutions have chosen to put insulin orders within the main admission order set to avoid workflow barriers, 5 but we chose to make our order sets separate from our admission order set to facilitate indication-based ordering. Within several of the order sets, we included the option to prescribe either fixed or CHO-based nutritional insulin doses. To avoid hypoglycemia in patients with poor appetites, a “postmeal” order set allowed nurses to adjust nutritional doses based on the amount of the meal that the patient ate, administering the dose immediately after the meal.
CPOE Glycemic Management Order Sets for Adult Hospital.
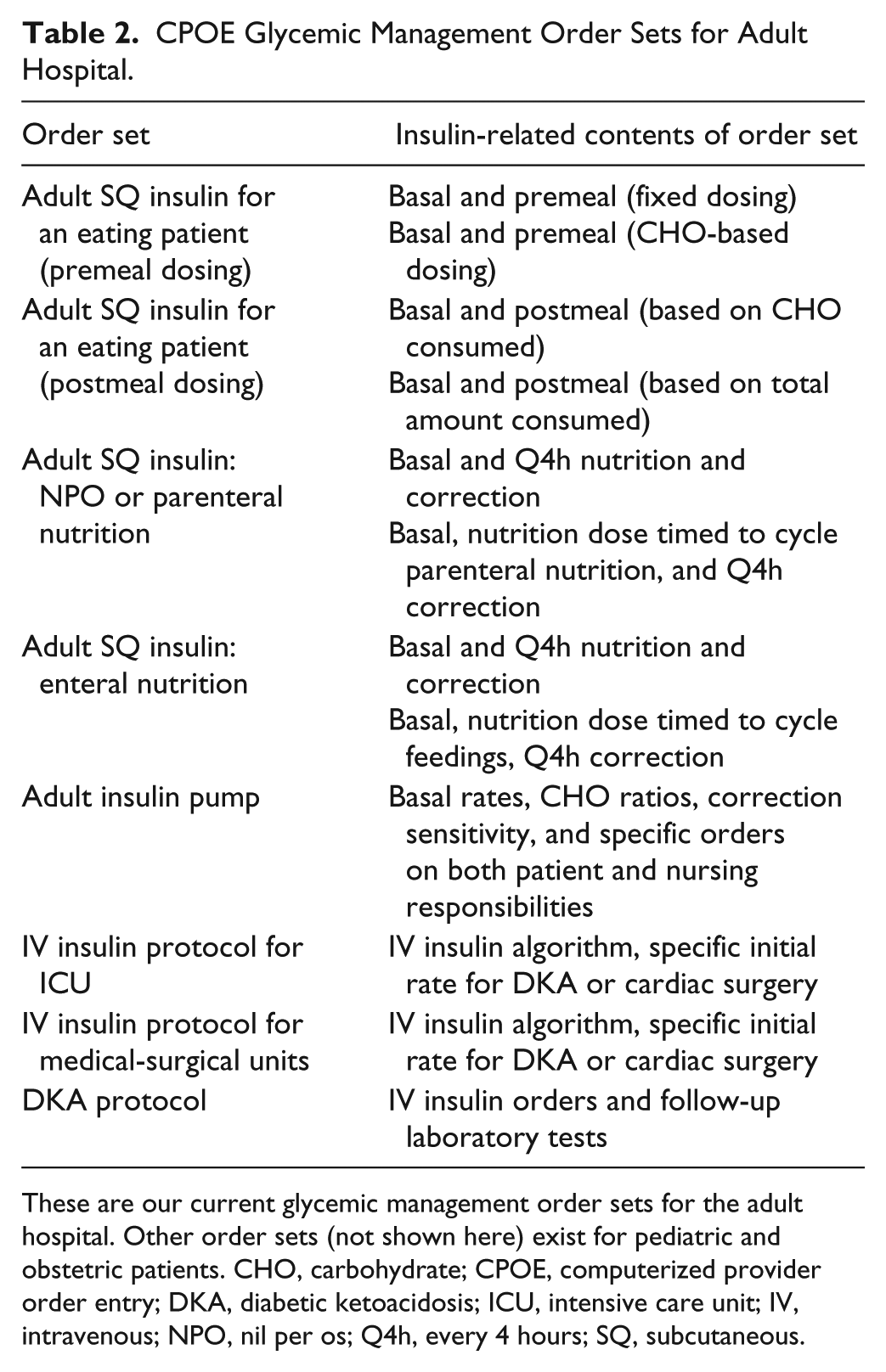
These are our current glycemic management order sets for the adult hospital. Other order sets (not shown here) exist for pediatric and obstetric patients. CHO, carbohydrate; CPOE, computerized provider order entry; DKA, diabetic ketoacidosis; ICU, intensive care unit; IV, intravenous; NPO, nil per os; Q4h, every 4 hours; SQ, subcutaneous.
To prevent insulin dose stacking and iatrogenic hypoglycemia in patients on enteral or parenteral nutrition, we coordinated with nutritional services and surgeons to standardize nutrition cycle times and insulin dosing. Twelve-hour nutrition cycles would all run from 1800 to 0600 hours, 14-hour cycles from 1800 to 0800 hours, and 16-hour cycles from 1800 to 1000 hours. These times are built directly into those order sets to eliminate possible errors. To prevent calculation errors when adding nutritional and correctional insulin doses, we created an insulin dose calculator to help nurses determine the proper rapid-acting insulin dose (Figure 5).
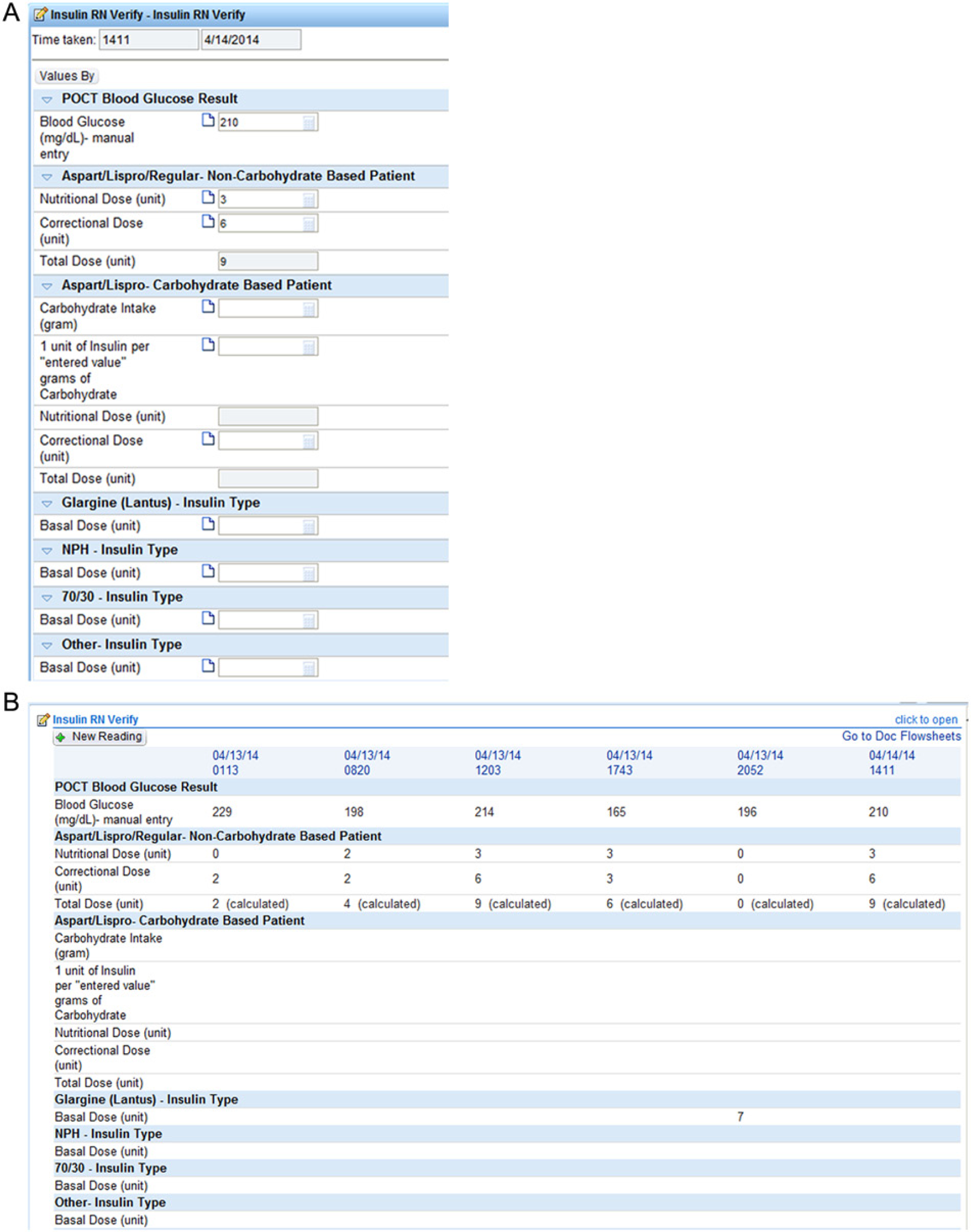
Nursing insulin verification tool. (A) The nurses enter the patient’s point of care testing result for blood glucose and use the patient’s correctional scale to determine the proper correctional dose. The system then adds together the nutritional and correctional doses to come up with the total rapid-acting insulin dose. (B) This information populates a flowsheet.
To assist providers in reviewing and adjusting insulin regimens, we built a review flowsheet (Figure 6) to allow providers to quickly view the last 24 hours of glycemic control information. This comprehensive flowsheet includes point of care glucose values, insulin doses administered, IV medications administered containing dextrose, the percentage of the meal consumed, enteral feeding type and administration rates, and any oral hypoglycemic agents administered. We hoped that this tool would help encourage providers to perform more frequent assessments and adjustments of insulin regimens.
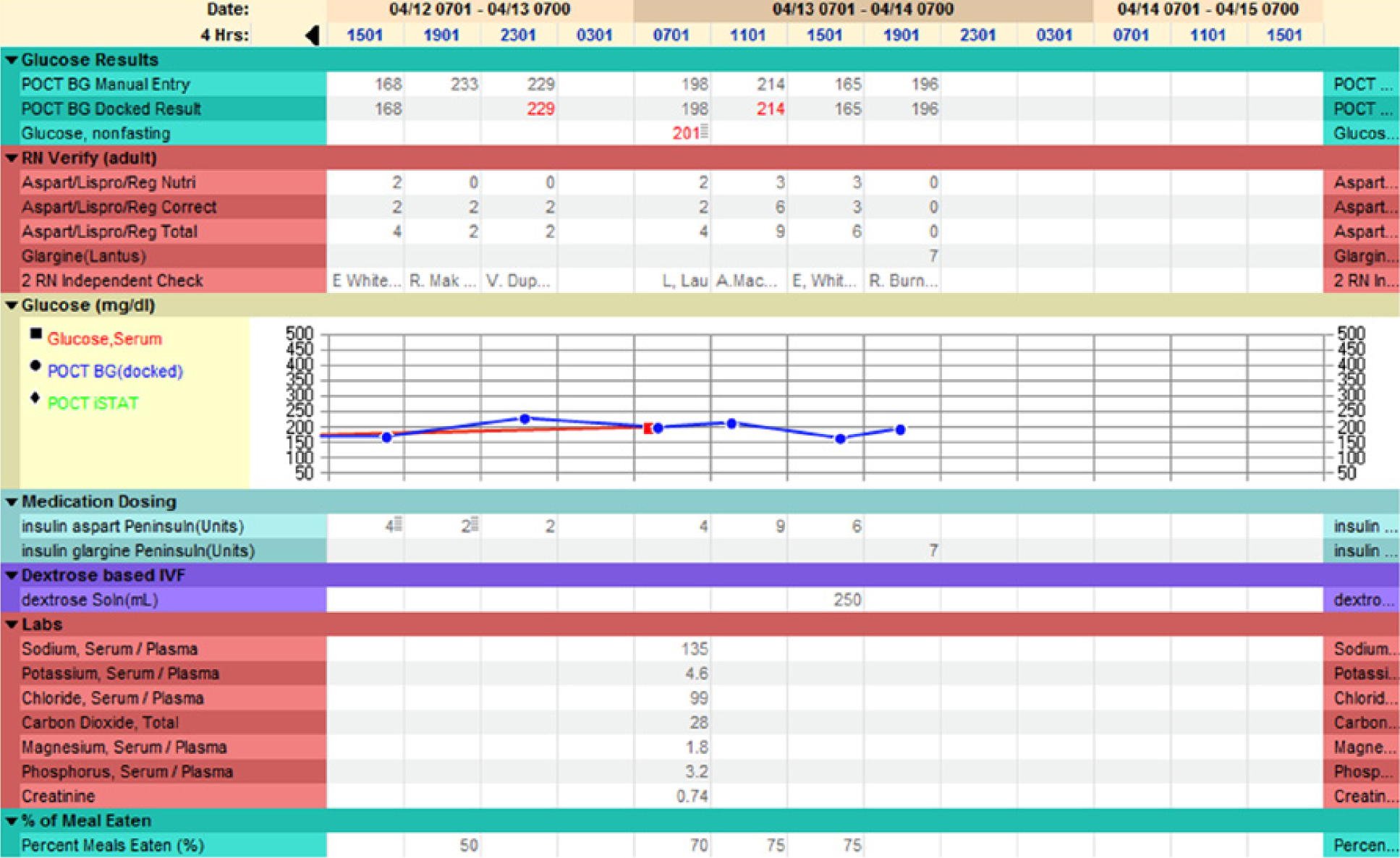
Insulin glucose flowsheet. In this view, 4-hour time intervals are chosen to allow a review of more data points. To view the exact times of blood glucose or insulin doses, a 1-hour time interval could instead be chosen.
Step 3: Implementation and Dissemination
Prior to our institution’s inpatient EHR go-live in June 2012, all health care providers had to attend training courses specific to their discipline. An optional computerized module was created to teach prescribers how to order insulin using the various order sets. Pharmacists were required to complete training, which included verification of the insulin orders as well as how to capture omissions or prescribing errors. Nurses were required to attend the Bar Code Medication Administration Simulation Laboratory, which had simulated cases on insulin administration. We created a guide sheet for nurses and providers to help them use the order sets appropriately.
Step 4: Optimization
To optimize our CPOE glycemic management build, the Diabetes and Insulin Management Committee monitored the change requests that were submitted to the EHR build team. The Diabetes and Insulin Management Committee problem-solved solutions to enhance the order sets and provided additional on-site training to the providers.
One example of a change request was in response to our removal of individual insulin orders from the available medication list. We had done this to ensure that providers only used our insulin order sets, in contrast to what has been done in some other institutions where the use of these order sets was optional. 13 From experience, we did not want to allow for “rogue” insulin orders that could lead to misinterpretation, errors, duplicates, and orders placed without hypoglycemia protocol orders and other linked orders. So, for example, if a provider typed in “lispro” in the medication order field, he or she would not find anything. This decision caused a challenge in a patient admitted with elevated glucose levels due to a faulty insulin pump. The provider was unable to decide whether to commit to the insulin pump order set or the SQ insulin order set, causing a delay in care. This might have been ameliorated had the provider been able to place a 1-time insulin order. So, we created a workflow whereby there is an “order set” allowing a 1-time insulin order.
Nevertheless, a remaining problem is that we have a large number of duplicate orders in the system. In our CPOE system, there is no ability to automatically discontinue the prior insulin orders by placing a new insulin order set. Discontinuing the prior orders requires the providers to remember that they need to do so and to go to a separate screen to do this. Alternately, we could have turned on “duplicate order alerts,” but the system is unable to distinguish between an undesired duplicate order such as 2 conflicting aspart insulin orders and a desired duplicate order such as glargine insulin and aspart insulin. Experience with medication alerting in CPOE has shown that this type of a lack of specificity of alerts would lead to them being unsuccessful. 14 Lee et al 10 reported that they were able to achieve this goal with their build in the Invision Siemens system by allowing for orders to be updated and changed rather than requiring new ones.
To combine our nutritional and correctional insulin doses into 1 order, we had to use a free-text administration instruction for these doses rather than the discrete dose field in the CPOE system. We used a minimum-maximum range in the discrete dose field. This unintentionally caused a large number of “high-dose” alerts from our First Data Bank alerting system. We decided to turn off the high-dose insulin alerts to reconcile this problem, realizing that the alerts in this case were all false-positives.
We have faced additional challenges during optimization. It has been difficult to maintain the necessary resources to continually update our original work after the initial implementation effort. Also, changes in practice cannot be accomplished just by changing order sets, and we have been challenged to get all providers to complete the training and educational modules.
Discussion
Several considerations are critical while developing CPOE glycemic management order sets, a process we have laid out in Figure 7. The implementation team should give equal consideration to all elements of the workflow, such as initial provider order placement, pharmacy verification, and nurse insulin administration. Changing the way that an order looks to a provider will have important downstream consequences on how the order looks to a nurse or pharmacist (Figure 8). Having all stakeholders present to ensure that the build meets their needs is important. Providers, nurses, and pharmacists should receive education on how to use the order sets. It is important to have processes in place for continuous quality improvement so that the order sets can be improved and updated based on user experience and feedback. As shown in Figure 9, some of our order sets are rarely used, such as the order set that accounts for patients who might not finish their food, allowing rapid-acting insulin to be given after the meal rather than before the meal. One limitation of this article is that we have not included data comparing hospital glucometrics before and after this EHR implementation, an analysis that is currently ongoing.
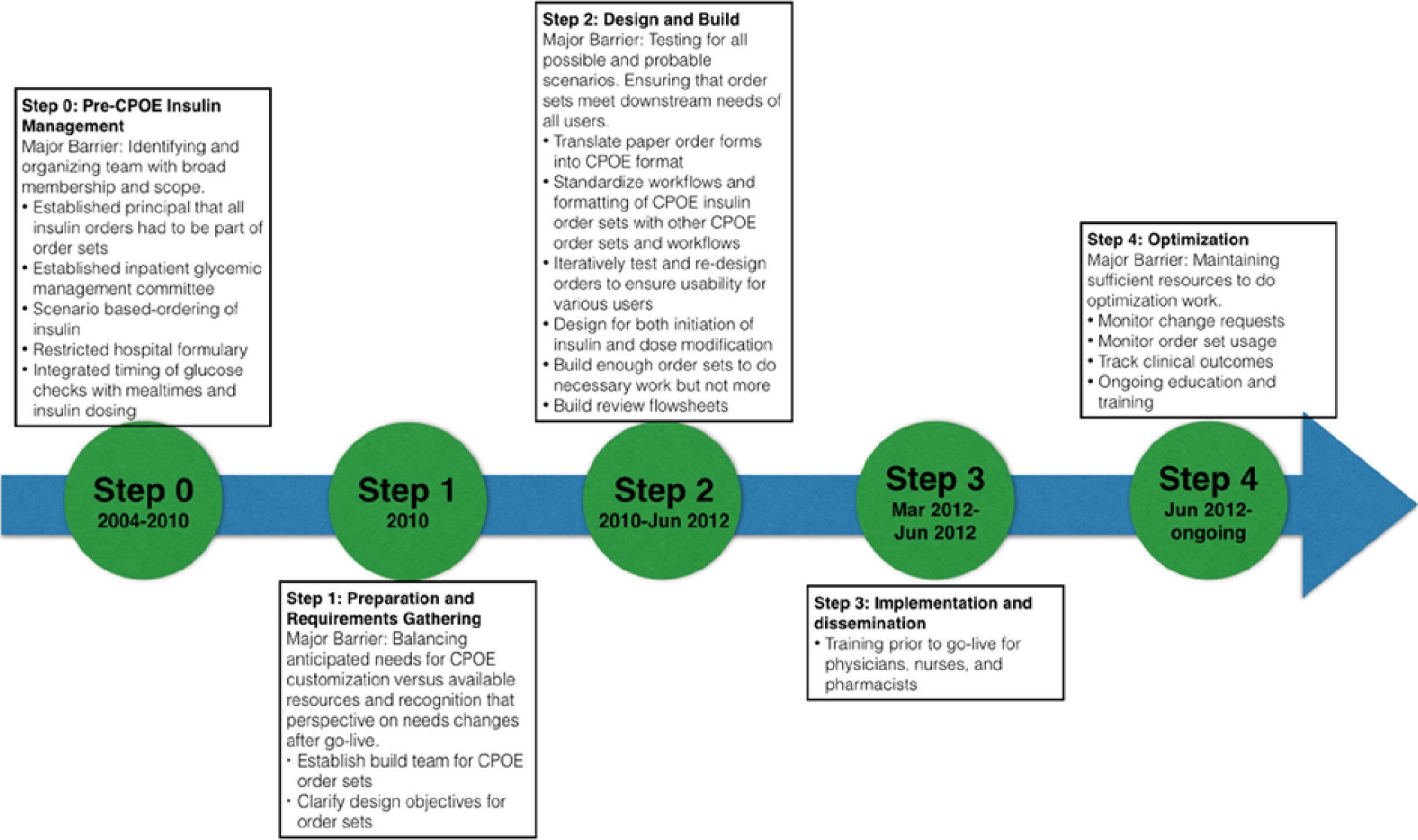
Flowchart of steps to move from paper to computerized provider order entry hyperglycemia management order sets.
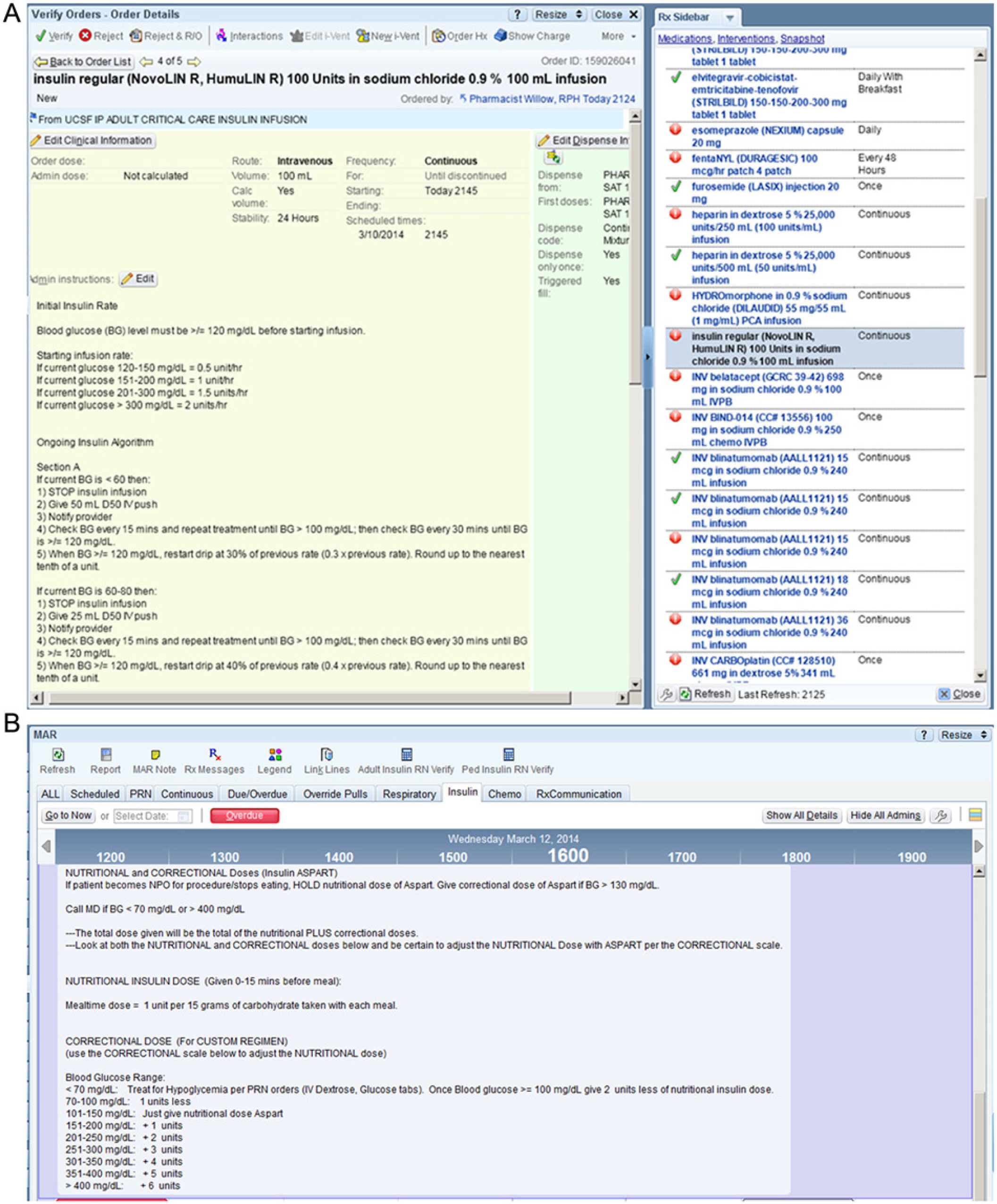
Pharmacist and nurse medication administration record (MAR) view of insulin orders. The insulin administration instructions were altered to allow formatting of the instructions to be clearly legible and well laid out for the pharmacist (A) and for the nurses in the MAR (B).
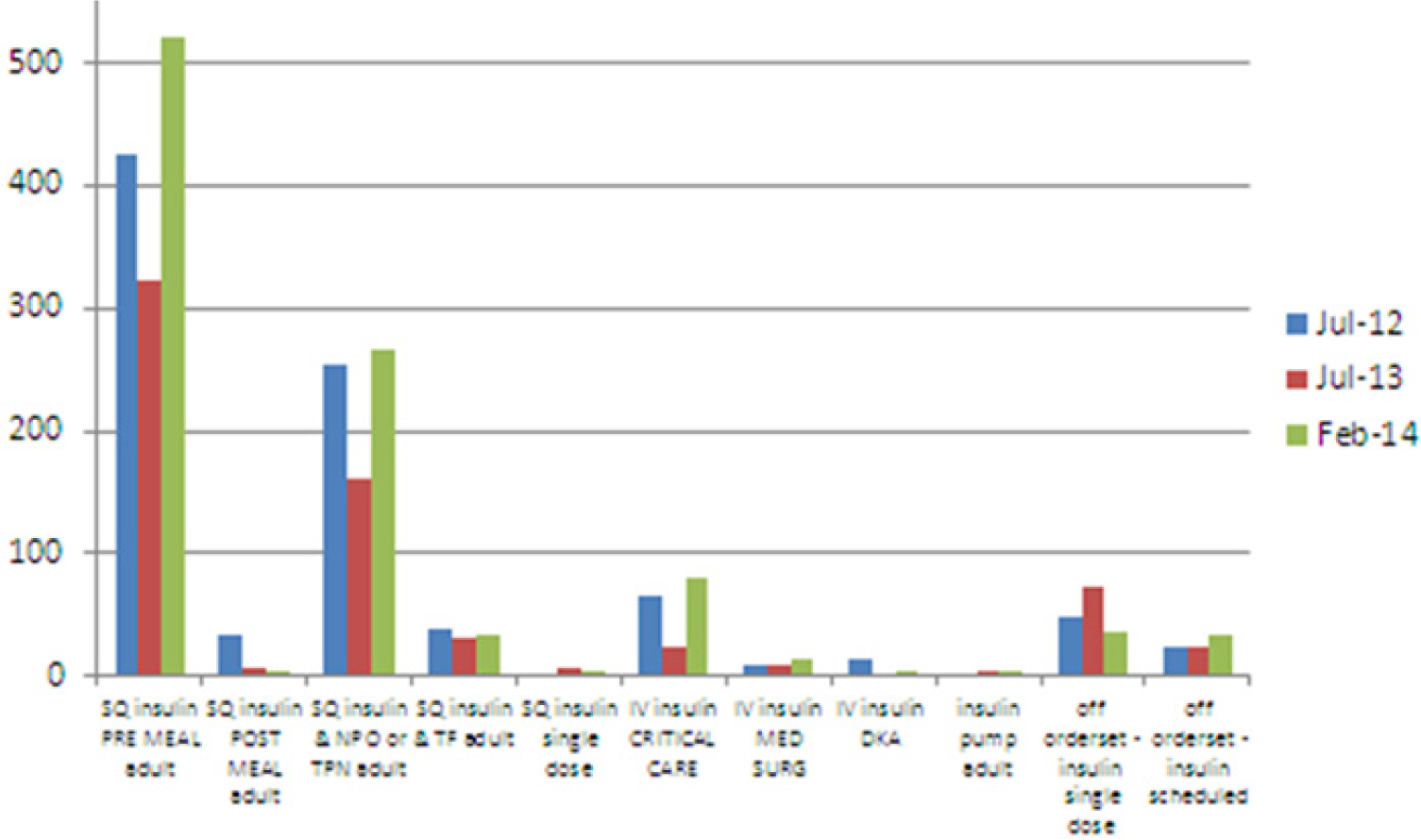
Utilization of glycemic management order set. Some of our order sets have not been frequently used, such as the subcutaneous insulin postmeal order set. Note that our inpatient computerized provider order entry go-live was June 2012, so these data points represent 1 month after go-live, 1 year later, and the current state.
Looking toward the future, there are several looming challenges. As hospitals become more patient centric, one change is the dietary services unit’s move to patient-centered, hotel-style (Meals on Demand) room service. While this is laudable as an act of customer service, it introduces great challenges for glycemia management. For example, the system would have a hard time accounting for the scenario in which a blood glucose (BG) check is performed and intended before the meal but the patient then decides to eat 2 hours later. We currently have hospital floors piloting a system to try to ensure that skipping a meal does not mean skipping a BG check and correctional doses. Patients should also be involved in these workflows and be educated on their responsibility to work with hospital staff to optimize BG control on a flexible eating schedule. We are not aware of an available electronic system that provides integrated information to nursing and food service departments, identifying patients needing BG checks and premeal insulin prior to the delivery of the food tray.
Finally, inpatient insulin orders in CPOE should be thought of as part of the continuum of care rather than a separate entity. Electronic health records have allowed for patients’ records to fluidly follow them from the ambulatory setting to the emergency department to the hospital and back to the ambulatory setting. Ideally, workflows and EHR build should be designed to take advantage of this, allowing glycemic-related orders to flow from setting to setting rather than viewing them each as mutually exclusive settings of care.
Footnotes
Acknowledgements
Kethen So, PharmD, was instrumental in designing and building our glycemic management order sets. Russ Cucina, MD and Andy Auerbach, MD also provided guidance and input.
Abbreviations
BG, blood glucose; CHO, carbohydrate; CPOE, computerized provider order entry; DKA, diabetic ketoacidosis; EHR, electronic health record; ICU, intensive care unit; IV, intravenous; MAR, medication administration record; NPO, nil per os; SQ, subcutaneous.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: R.R. has conducted speaking engagements supported by Novo and Merck within the past 5 years.