
Abstract
During the last 2 decades, the treatment of hyperglycemia in critically ill patients has become one of the most discussed topics in the intensive medicine field. The initial data suggesting significant benefit of normalization of blood glucose levels in critically ill patients using intensive intravenous insulin therapy have been challenged or even neglected by some later studies. At the moment, the need for glucose control in critically ill patients is generally accepted yet the target glucose values are still the subject of ongoing debates. In this review, we summarize the current data on the benefits and risks of tight glucose control in critically ill patients focusing on the novel technological approaches including continuous glucose monitoring and its combination with computer-based algorithms that might help to overcome some of the hurdles of tight glucose control. Since increased risk of hypoglycemia appears to be the major obstacle of tight glucose control, we try to put forward novel approaches that may help to achieve optimal glucose control with low risk of hypoglycemia. If such approaches can be implemented in real-world practice the entire concept of tight glucose control may need to be revisited.
Keywords
Hyperglycemia is a well-known phenomenon in critically ill patients after severe trauma, extensive surgery, major infection or other severe conditions regardless of previous history of diabetes mellitus. 1 It is often called “stress hyperglycemia” or “diabetes of injury.” The development of hyperglycemia is the consequence of increased hepatic glucose output and its reduced peripheral utilization owing to decreased insulin sensitivity. 2 Other contributing factors include insufficient insulin secretion, increased load of enteral or parenteral nutrition and the use of medication increasing glucose levels such as glucocorticoids, catecholamines, and others. 3 Primary factors responsible for increased hepatic glucose output and decreased insulin sensitivity are stress hormones and proinflammatory cytokines.
In critically ill patients, hyperglycemia has long been considered an evolutionary protective and adaptive response of the organism to stress, important for survival. An overall increase in the metabolic turnover of glucose supporting its uptake in non-insulin-dependent tissues was suggested as the main benefit of higher glucose levels in critically ill. The recommended blood glucose levels in critically ill patients, maximizing cellular uptake of glucose without the risk of hyperosmolar effects was 9-11 mmol/l. 4 In addition, mild hyperglycemia was seen as a buffer against the risk of damage of the central nervous system by hypoglycemia during the insulin therapy.
From the current perspective, hyperglycemia is clearly seen as a detrimental factor. 2 Several studies have demonstrated a J-curve relationship between blood glucose and mortality suggesting that both hypo- and hyperglycemia are harmful. 5 It is also fair to mention that these studies by design cannot answer the question whether hyperglycemia per se plays a fundamental causal role in worse outcomes or whether it could be rather a marker of more severe injury. In any case, numerous studies have demonstrated negative effect of increased glucose levels and/or its excessive fluctuations commonly referred to as glucose variability due to induction of oxidative stress resulting from undue production of mitochondrial peroxides.6,7 Almost all organ systems could be negatively affected by hyperglycemia including cardiovascular and central nervous system, kidney, coagulation cascade, and the immune system.8-11 Numerous studies have suggested that stress hyperglycemia present in up to 90% of patients with critical illness is associated with increased morbidity and mortality and poorer prognosis of these patients.12,13
Hyperglycemia in Intensive Care
In 2001, the landmark Leuven study performed in surgical intensive care unit (ICU) demonstrated that intensive insulin therapy (IIT) aimed at maintaining glycaemia between 4.4 and 6.1 mmol/l reduced mortality and decreased frequency of severe organ complications. 14 Several other studies confirmed these findings especially in cardiac surgery patients.15,16 However, some other trials questioned safety, reproducibility and universality of beneficial effects of tight glycemic control (TGC) in other subgroups of critically ill patients, leading consequently to a shift toward a more conservative approach to glucose lowering in ICU settings in the last years.17,18 The results of some of the studies which could not reproduce positive effects of Leuven study could have been partially affected by some methodological shortcomings such as the lack of standardized glucose measurements methods and the insufficient time for tight glucose control implementation in various ICUs consequently leading to very high prevalence of hypoglycemia. On the other hand, at present such limitations do exist in real-life conditions and therefore should be taken into account. Furthermore, while hyperglycemia worsens the outcomes in critically ill patients, several trials including large NICE sugar trial have demonstrated that both moderate and severe hypoglycemia were also independently associated with mortality. 18 The balanced approach without excessive risk of hypoglycemia is therefore clearly needed. Principally, the need to decrease marked hyperglycemia in critically ill patients has been generally accepted, nevertheless the exact target range in various patient subpopulations is a subject of ongoing discussion.19,20 Because of the risk of hypoglycemia, which could potentially outweigh the benefits of tight glucose control, the intermediate target blood glucose range of 6-8 mmol/l is generally recommended in intensive care units with appropriate experience with IIT and the possibility of frequent blood glucose monitoring. 21 A recent meta-analysis of glucose control in ICU has suggested that surgical patients, in particular the cardiac surgery patients, could benefit from even tighter glycemic control targeting the “Leuven range” of 4.4-6.1 mmol/l. 22 The implementation of such tight glucose control may significantly increase the risk of hypoglycemia. Therefore such approach could only be used in the ICUs with long-term experience in insulin titration protocols and properly trained nursing staff. 23 The 3-month implementation period should be according to our and others’ experience the minimum learning time to safely use an appropriate IIT protocol. 23
How to Control Blood Glucose in the ICU
Dynamics of hyperglycemia in critically ill patients is extremely variable due to both individual differences in the development of insulin resistance under different conditions and other influences such as varying pharmacological and nutritional interventions. 24 It is now clear, that the necessary prerequisite for adequate glucose control in critically ill patients is continuous administration of intravenous insulin allowing for better adaptability of insulin protocols to changes in insulin resistance. 25 The use of a simple, safe, and effective insulin administration protocol and standardization of glucose measurements are another critical points necessary for successful tight glucose control implementation. 26
Numerous insulin protocols of variable effectiveness and safety outcomes have been developed.27,28 Most of them require considerable ICU staff training and experience, and some call for intuitive decisions. In consequence, some protocols may lead to inconsistent application, mistakes, or misinterpretation. Most recently introduced computer-based predictive algorithms show significantly better performance with less room for error and adverse effects compared to standard paper-based protocols.29,30 For example, we have demonstrated that the computer-based algorithm with a variable sampling interval (Figure 1) was more effective in achieving and maintaining tight glucose control in cardiac surgery patients compared to standard paper-based protocols. 23 Nevertheless, even with the use of the best insulin administration protocol, appropriate nursing staff training and standardized and precise glucose measurements tight glucose control is still associated with increased risk of hypoglycemia compared to conventional less strict glucose control. 31 Hypoglycemia was associated with increased risk of death and prolonged ICU stay in several studies.18,32 although in some others this association was not found. 33 As the response of ICU patients to hypoglycemia is often blunted, frequent glucose monitoring is an essential prerequisite of nearly all IIT algorithms. 34 However, frequent blood sampling increases dramatically the workload of the nursing staff and the intermittent fashion of classical glucose sampling does not always capture all of the glucose fluctuations including hypoglycemic events. 34 Continuous glucose monitoring (CGM) could therefore be an ideal tool for catching rapid glycemic excursions (both hypo- and hyperglycemia) and providing the algorithm with (nearly) real-time glycemic data to improve its efficacy and safety. 35 A recent study on healthy volunteers has demonstrated that there is a physiological delay of glucose transport from the vascular to the interstitial space of 5-6 minutes. 36 while data on this lag time in critically ill patients are not available at this moment.
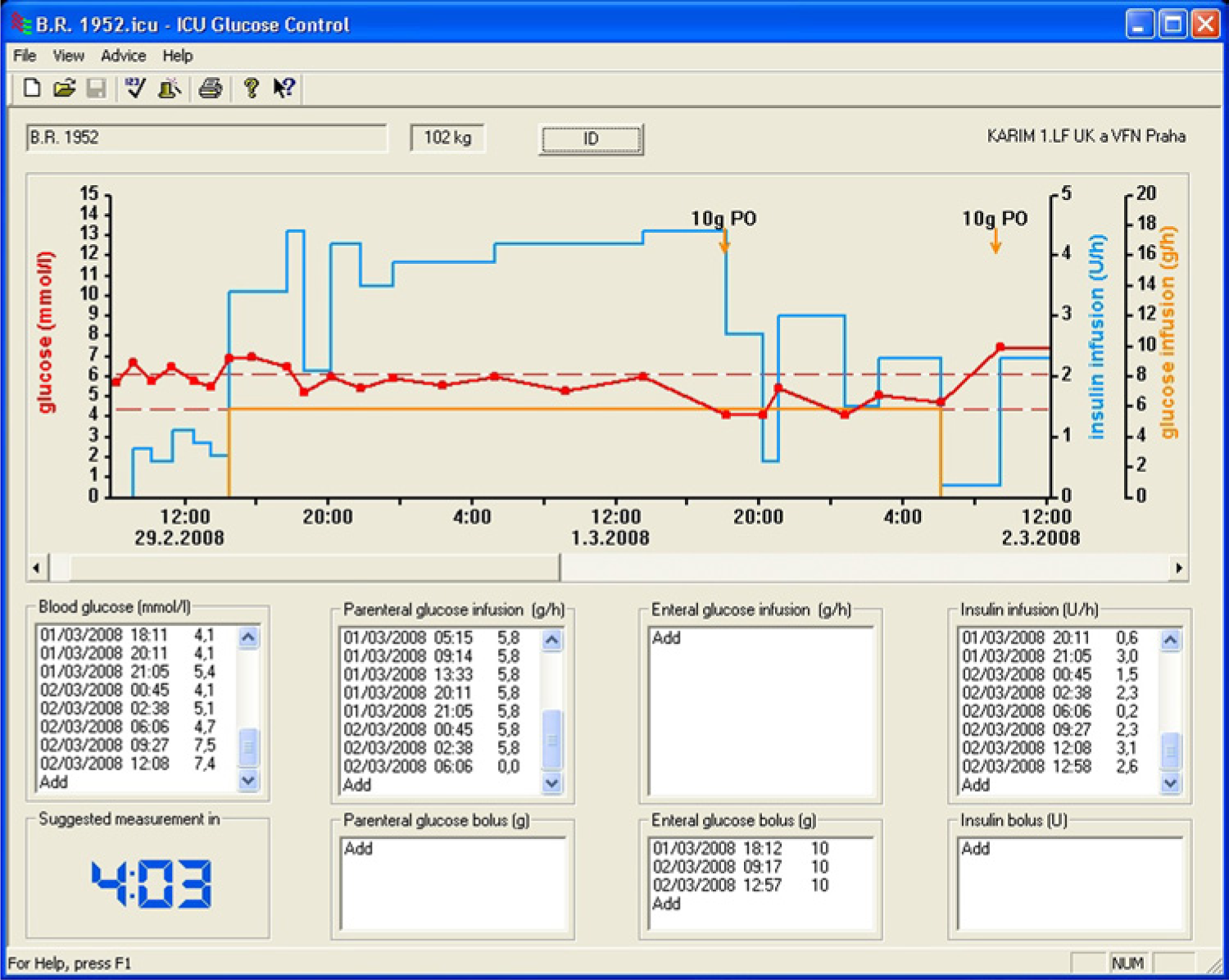
An example of a computer-based insulin algorithm. eMPC, enhanced model of predictive control.
The Timing of Tight Glucose Control: The Devil Is in the Details
In surgical patients, the tighter glucose control is usually implemented after the transfer of patients from operating theatre to intensive care unit while relatively little attention to glucose control is paid during surgery. 37 Only few small studies focusing on intraoperative versus postoperative tight glucose control initiation have been published so far with quite inconsistent results.38,39 A recent meta-analysis of 5 randomized controlled trials comparing intensive and conventional insulin therapy during cardiac surgery did not demonstrate any significant benefit with the exception of reduced infection rates. 40 In our recent randomized study performed on more than 2300 cardiac surgery patients, the perioperative initiation of tight glucose control using intensive intravenous insulin therapy during surgery reduced postoperative morbidity in nondiabetic patients while it had very little effect on diabetic patients. 41 Taken together, the timing of the initiation of tight glucose control in surgical patients represents another potentially important issue that still needs to be tested and further clarified.
How Much Help Can We Get From Novel Technologies?
In the intensive care unit, standard monitoring of glucose levels is performed in an intermittent fashion with various frequencies ranging from a 1- to 6-hour interval. CGM systems, which have been used for several years in patients with diabetes, could solve the problems with unrecognized glucose variations and above all, increase the safety of tight glucose control by preventing hypoglycemia. 42 Nonetheless, at the moment all of the CGM systems are designed to measure glucose concentrations in the interstitial fluid of subcutaneous adipose tissue in clinically stable patients with diabetes. The use of the same devices in critically ill patients suffering from peripheral tissue hypoperfusion thus could give inaccurate results. The correlation between interstitial fluid and systemic glucose has been the subject of several studies including our investigations. Overall, the data suggest a good correlation in most of the patients but the optimal approach would still be the use of intravenous rather than subcutaneous continuous sensor placement. 43 However, the first commercially available intravascular sensors are only now starting to emerge, and their clinical value still needs to be evaluated.
Another possible drawback of the use of commercially available continuous glucose sensors could be the possible interference of electrochemical and optical measurement methods with various medications and other compounds used in critically ill patients. Here, the data are very scarce and this important possibility certainly needs further evaluation.
The ultimate goal of the use of CGM in ICU is its direct connection to glucose control algorithm eventually leading to a complete closing of the loop. To date, only a few studies using CGM values as an input for glucose control algorithms in the ICU have been published, all of them using glucose values obtained by subcutaneous sensors developed for patients with diabetes. In general, the optimal CGM should be able to measure glucose concentrations in a short time period (eg, every 5 minutes) for a couple of days, and its setup and calibration should be simple. The number of calibrations per day should ideally be 2 or less. 44
We have performed a feasibility study using CGM and computer-based enhanced model of predictive control insulin algorithm (eMPC) in 24 elective cardiac surgery patients. 45 A subcutaneous glucose sensor was inserted under the skin in the abdominal region and glucose was measured every 5 minutes and displayed on the monitoring unit. The system was calibrated using arterial blood glucose concentrations. In the CGM group, data from continuous monitor were entered manually into the eMPC every 15 minutes. Every hour, glucose value from continuous glucose monitor was compared with reference arterial glucose using the Clarke error grid analysis (C-EGA) and when clinically unacceptable reference glycaemia was used as input for the eMPC and to recalibrate the CGM system. The control group was treated by the eMPC algorithm alone, while the variable sampling interval for the next blood glucose measurement calculated by the eMPC was respected. Arterial glucose was used as input for the eMPC. In this study, the combination of eMPC algorithm with CGM by Guardian Real-Time (Medtronic, Minneapolis, USA) CGM system was reliable, accurate, and efficient enough to test this approach in larger populations. 25 A larger trial testing this approach is currently underway in our department. A recent prospective randomized controlled trial by Leelarathna and colleagues has demonstrated that an automated closed-loop approach based on subcutaneous glucose measurements (FreeStyle Navigator sensor [Abbott, Alameda, USA]) and intravenous insulin administration in surgical critically ill patients was more effective in controlling glucose than a local sliding-scale insulin-therapy protocol with a negligible risk of hypoglycemia. 46 The important question of whether the subcutaneous CGM system precision might be affected by changes in microcirculation has been tested in a recent prospective, observational study in 60 cardiac surgery patients. 47 In this study, the microcirculation was measured using the microvascular flow index, perfused vessel density, and proportion of perfused vessels using sublingual sidestream dark-field imaging, and tissue oxygenation was measured using near-infrared spectroscopy. Two systems for CGM were used (Guardian Real-Time and FreeStyle Navigator) in each of the patients included into the study. The relative absolute deviation between CGM and the arterial reference glucose was calculated to assess the accuracy. The associations were assessed using a linear mixed-effects model for repeated measures. The authors concluded that both of the continuous sensors had acceptable accuracy in patients after cardiac surgery. The microcirculation was impaired to a limited extent compared with that in patients with sepsis and healthy controls. This impairment was not related to sensor accuracy. Another recent trial has demonstrated that accuracy of the Navigator CGM device during critical illness was comparable to that observed in non-critical-care settings and that further significant improvements in accuracy could be obtained by frequent calibrations with arterial blood glucose measurements. 48
In another recent trial, a central venous catheter with a microdialysis membrane in combination with an online analyzer for continuous monitoring of circulating glucose and lactate by the central route was tested. 49 A total of 10 patients undergoing major upper abdominal surgery were included. The patients were inserted an extra central venous catheter with a microdialysis membrane placed in the right jugular vein. Continuous microdialysis measurement lasted for 20 hours and online values were recorded every minute. Reference arterial plasma glucose and blood lactate samples were collected every hour. This study demonstrated that continuous online microdialysis glucose measurement in a central vein is a feasible and potentially useful technique for CGM in critically ill patients. On the other hand, the use of such technique in a routine clinical practice will still require overcoming of some technical and logistical difficulties such as limited long-term continuous vascular access in some patients, its maintenance, the prevention of its occlusions, and so on.
Why Should the Targets for Glucose Control Be More Ambitious and Is It Feasible?
The idea that normalization of blood glucose levels in critically ill patients may not be beneficial or may be even harmful is supported by some studies showing increased rate of hypoglycemia in intensively treated patients with its potentially harmful consequences.18,50 The outcomes of some of these studies could have been affected by technical or logistical issues such as insufficient experience of some of the centers with tight glucose control, lack of standardized methods for blood glucose measurements, and the use of suboptimal protocols for tight glucose control. 51 Studies favoring tight glucose control have shown that most of these difficulties could be overcome by proper training of nursing staff and the use of advanced computer-based predictive algorithms.14,23,28 Furthermore, IIT may not be the sole therapeutic option of critically ill patients. Smaller studies on patients with acute myocardial infarction 52 and surgical patients 53 including our recent data on cardiac surgery patients suggest that both native GLP-1 and short-acting GLP-1 receptor agonists such as exenatide (Haluzik et al, accepted for American Diabetes Association 74th Scientific Sessions, 2014) can be safely used as a continuous intravenous infusion in the intensive care unit settings allowing for lower dose of insulin and decreased risk of hypoglycemia. Given the possible cardioprotective 54 and neuroprotective effects of GLP-1 receptor agonists 55 such approach could carry additional benefits for critically ill patients beyond effective and safe glucose control. Combining these novel therapeutic options with technical advances in CGM and advanced computer-based algorithms for insulin administration can bring the possibilities of glucose control in critically ill patients to a higher level achieving more ambitious glucose targets with low risk of side effects. The question whether tight glucose control per se with low risk of hypoglycemia is or is not beneficial and what patients could benefit the most may need to be reassessed. Recent trials with tight glucose control in type 2 diabetes patients have taught us a lesson that the one-size-fits-all concept can hardly be successfully applied in any heterogeneous population.56,57 Critically ill patients with different underlying causes of critical illness and diverse combination of other pathologies certainly represent a very heterogeneous population calling for further studies as a base for personalized blood glucose treatment targets.
Conclusions
The need for glucose control in critically ill patients is now generally accepted yet the exact target glucose values for different patient populations are still being intensively discussed. Novel technologies such as CGM, computer-based adaptive glucose control algorithms, and the possibility of adding novel therapeutics such as GLP-1 receptor agonists into treatment armamentarium may help to achieve glucose levels close to the normal range with low risk of hypoglycemia and other side effects. Numerous obstacles still need to be overcome including the availability of better continuous glucose sensors optimally for intravenous application with a full regulatory approval for the use in critically ill patients. This treatment strategy may represent a further step toward a fully automated closed-loop system for the treatment of hyperglycemia in critically ill patients. Once safely implemented into clinical practice it might be worthwhile to rechallenge the benefits of tight glucose control approach in larger patient populations given that the implementation of CGM and other novel technologies into the system reduced the risk of potentially harmful hypoglycemia.
Footnotes
Abbreviations
C-EGA, Clarke error grid analysis; CGM, continuous glucose monitoring; eMPC, enhanced model of predictive control; ICU, intensive care unit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RVO-VFN64165 and SVV260019/2014.