
Abstract
Background:
The objective was to identify the presence of cardiovascular autonomic neuropathy (CAN) in a cohort of individuals with diabetes in outpatient clinics from 4 different parts of Denmark and to explore the difference between type 1 and type 2 diabetes in relation to CAN.
Methods:
The DAN-Study is a Danish multicenter study focusing on diabetic autonomic neuropathy. Over a period of 12 months, 382 type 1 and 271 type 2 individuals with diabetes were tested for CAN. Patients were randomly recruited and tested during normal visits to outpatient clinics at 4 Danish hospitals. The presence of CAN was quantified by performing 3 cardiovascular reflex tests (response to standing, deep breathing, and valsalva). To describe possible associations, multivariate analysis with CAN as the dependent variable was performed.
Results:
The prevalence of CAN was higher among patients with type 2 diabetes (35%) compared to patients with type 1 diabetes (25%). Multivariate analysis revealed significant associations between CAN and different risk markers in the 2 populations. In type 1 diabetes patients CAN was associated with microalbuminuria (P < .001), macroalbuminuria (P = .011), simplex retinopathy (P < .001), proliferative retinopathy (P < .001), and peripheral neuropathy (P = .041). Among type 2 diabetes patients CAN was independently associated with high pulse pressure (P < .01), BMI (P = .006), and smoking (P = .025).
Conclusion:
In this cross-sectional observational study CAN was independently associated with microvascular complication in type 1, whereas in type 2 CAN was associated with macrovascular risk factors.
Keywords
Autonomic neuropathy affects both the sympathetic and parasympathetic nervous system, which provides a rapidly responding mechanism to control a wide range of functions such as cardiovascular, respiratory, gastrointestinal, renal, endocrine, and other systems.1,2 The balance/imbalance in the autonomic nervous system can be determined by computer-assisted and complex analyses of variations in blood pressure and in electrocardiographic measurements. 2 For clinical use the gold standard tests are heart rate response to (1) change from supine to upright position, (2) deep breathing, and (3) the Valsalva manoeuvre. 3 In the diabetic population abnormal results in 2 or more of the gold standard tests constitutes a surrogate measure and a subclinical diagnostic marker of cardiovascular autonomic neuropathy (CAN). 3 We have recently published a feasibility study, showing that tests for CAN, as a routine examination in an outpatient clinic, is possible with a handheld device. 4 The prevalence of CAN is estimated to be approximately 20-70%, depending on the test used and the population investigated.5,6 The prevalence is higher among patient with type 2 as compared to type 1 diabetes. Different pathophysiological and progression mechanisms may account for the onset and progression of neuropathy in type 1 and type 2 diabetes.7,8 A recent publication suggests that CAN in normoalbuminuric type 1 patients is associated with distinct signs of subclinical cardiovascular disease. 9 In this context early testing of CAN is an important risk marker and predictive for future stroke and (cardiovascular) death, both in the general population and in patients with diabetes.10,11 Adding to this, there is a link between hypoglycemia and CAN. A patient with hypoglycemia may encounter the same excessive sympathetic cardiac activation as a patient with severe heart failure.12,13 Therefore, the aim of this study was in a large-scale clinical setting to identify the presence of CAN in a cohort of individuals with diabetes in outpatient clinics covering 4 geographical regions in Denmark and to explore the difference between type 1 and type 2 diabetes in relation to CAN.
Methods
The study was performed as a multicenter cross-sectional observational study covering 4 geographical regions in Denmark (n = 5.5 million). Approximately 5% of the Danish population suffers from diabetes. Over a period of 12 months, patients were recruited consecutively 1 day each week on a volunteer basis from outpatient clinics at the following hospitals: Aalborg University Hospital, Aarhus University Hospital, Odense University Hospital, and Steno Diabetes Center. All patients with diabetes attending the 4 outpatient clinics were a priori eligible for participation and patients who met the inclusion criteria were offered an examination for CAN when appearing at the outpatient clinics. The investigation was logistically planned as an integrated part of the regular visits to the clinics, and the investigation was performed at the end of each visit. Beside the new handheld point-of-care test for CAN, all tests performed in this study reflect the normal clinical produces in the participating outpatient clinics.
Inclusion criteria were: age above 18 years, type 1 diabetes duration of more than 5 years, or type 2 diabetes from the time of diagnosis. Exclusion criteria were: overuse of alcohol (women 14 units per week and men 21 units per week), congestive heart failure (NYHA classification 3 and 4), arrhythmias preventing calculations of heart rate variability, and inability to undertake active examinations.
Definition of CAN
CAN was defined using the American Diabetes Association (ADA) criteria and the Toronto Consensus Panel on Diabetic Neuropathy as follows: CAN 0, all tests are normal; CAN 1, 1 test is abnormal, signifying the presence of borderline or early stage CAN; CAN 2-3, 2 or 3 abnormal tests signifying manifest CAN.3,14 At least 2 of the 3 tests should be performed to provide adequate diagnostic information. 15 All the heart rate-based tests were evaluated according to age-dependent cutoff levels. 6
Experimental Procedure
Smoking, food, and caffeine-containing liquids were prohibited 2 hours prior to laboratory testing. All tests of CAN were performed between 9
Laboratory Tests in Outpatients Clinics in Denmark
Peripheral neuropathy was examined using either age-related biothesiometry or Semmes-Weinstein monofilament (10 g) and test results were classified as normal or abnormal. Examination for diabetic retinopathy was performed by an ophthalmologist using retinal digital cameras. Retinopathy was classified as: none, simplex or proliferative retinopathy. Urine albumin-to-creatinine ratio (ACR) was used to classify kidney affection: normal (ACR < 30 mg/g), microalbuminuria (30 mg/g ≤ ACR ≤ 300 mg/g), and macroalbuminuria (ACR > 300 mg/g). Glycated hemoglobin (HbA1c) was determined by high-performance liquid chromatography (HPLC). Total cholesterol, triglycerides, and high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol were measured by enzymatic methods. All laboratory tests were performed in accredited laboratories guaranteeing comparable results.
Statistical Analysis
Patient characteristics are presented as unadjusted means. Comparison between patients without CAN and patients with CAN were performed using ANOVA for normally distributed measures whereas the Kruskal–Wallis test was used for nonparametric tests. Calculation of natural logarithms was performed to obtain a normal distribution where appropriate. To describe possible associations between patient characteristics and CAN score (form 0-3), ordinal logistic regression analysis with CAN score as the dependent variable were used. This multivariate analysis enables analysis of categorical data with more than 2 categories. P values of less than .05 were considered statistically significant. To assess the statistical difference between type 1 and type 2 diabetes, interaction terms with type of diabetes corresponding to each risk variable were added to the multivariate analysis. For statistical data processing, MATLAB (version 7.0.0.19920; MathWorks, Massachusetts, USA), SigmaPlot 11.0 (Systat Software, Inc, California, USA), and STATA 11 (StataCorp LP, Texas, USA) were used where appropriate.
Results
A total of 664 patients were included. Subsequently, 11 patients (1.6%) were excluded due to nonsinus atrial rhythm preventing heart rate variability calculations, or due to the inability to complete at least 2 active tests. Compared to the analyzed population, the excluded patients were older (P < .01), but otherwise comparable.
A minimum of 2 CARTs were successfully examined in the remaining 653 patients. Among these patients the Valsalva maneuver was not performed in 7.8% due to proliferative retinopathy and/or inability to perform the test correctly. The response to standing and the deep breathing test were not performed in 1.8% and 1.1% of cases accordingly. Manifest CAN was higher among type 2 diabetes patients (35%) compared to type 1 diabetes patients (25%). The same applies for early stage CAN (30% in type 2 vs 25% in type 1). In both type 1 and type 2 diabetes the prevalence of any CAN (type 2: 65% vs type 1: 50%) was comparable or more prevalent than any retinopathy (type 2: 56% vs type 1: 58%), micro- and macroalbuminuria (type 2: 39% vs type 1: 23%), and any peripheral neuropathy (type 2: 47% vs type 1: 31%). Patient characteristics are shown in Table 1. In the 2 populations we found no differences in CAN between genders.
Patients with Type 1 and Type 2 Diabetes Subgroups by Cardiovascular Autonomic Neuropathy (CAN) Score.
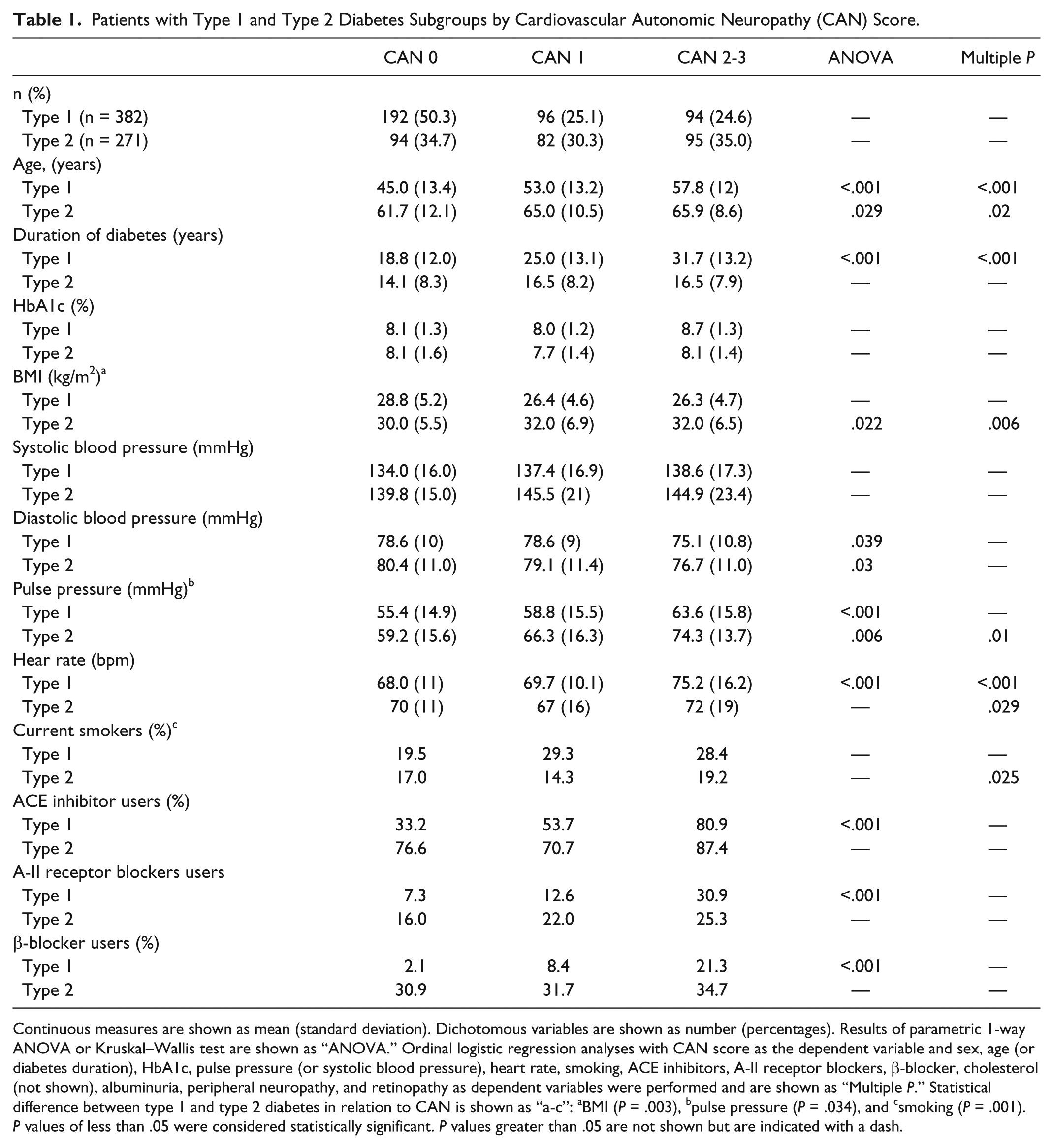
Continuous measures are shown as mean (standard deviation). Dichotomous variables are shown as number (percentages). Results of parametric 1-way ANOVA or Kruskal–Wallis test are shown as “ANOVA.” Ordinal logistic regression analyses with CAN score as the dependent variable and sex, age (or diabetes duration), HbA1c, pulse pressure (or systolic blood pressure), heart rate, smoking, ACE inhibitors, A-II receptor blockers, β-blocker, cholesterol (not shown), albuminuria, peripheral neuropathy, and retinopathy as dependent variables were performed and are shown as “Multiple P.” Statistical difference between type 1 and type 2 diabetes in relation to CAN is shown as “a-c”: aBMI (P = .003), bpulse pressure (P = .034), and csmoking (P = .001). P values of less than .05 were considered statistically significant. P values greater than .05 are not shown but are indicated with a dash.
Multiple ordinal logistic regression analysis revealed significant associations between CAN and different risk markers in the 2 populations. Type 1 diabetes patients with CAN were more frequently micro- (P < .001) or macroalbuminuric (P = .011) and had simplex retinopathy (P < .001), proliferative retinopathy (P < .001), or peripheral neuropathy (P = .041). CAN scores and microvascular complications are shown in Table 2. Type 2 diabetes patients with CAN had a higher pulse pressure (P < .01) and BMI (P = .006) and were more often smokers (P = .025). Furthermore, age and heart rate were associated with CAN in both type 1 and type 2 diabetes patients. Associations remained statistically significant after adjustment for sex, HDL, LDL, and total cholesterol, and systolic BP. Adjusting for drugs with potential beneficial effect on the cardiovascular system (ACE inhibitors and β-blockers) did not alter associations. Statistical difference between type 1 and type 2 diabetes in relation to CAN was tested by adding an interaction terms corresponding to each risk variable. This test revealed that CAN is associated with different clinical variables in type 1 and type 2 diabetes, respectively. Results shows that BMI (P = .003), pulse pressure (P = .034), and smoking (P = .001) are more important for CAN in type 2 compared to type 1 diabetes.
Cardiovascular Autonomic Neuropathy (CAN) Score and Microvascular Complications.
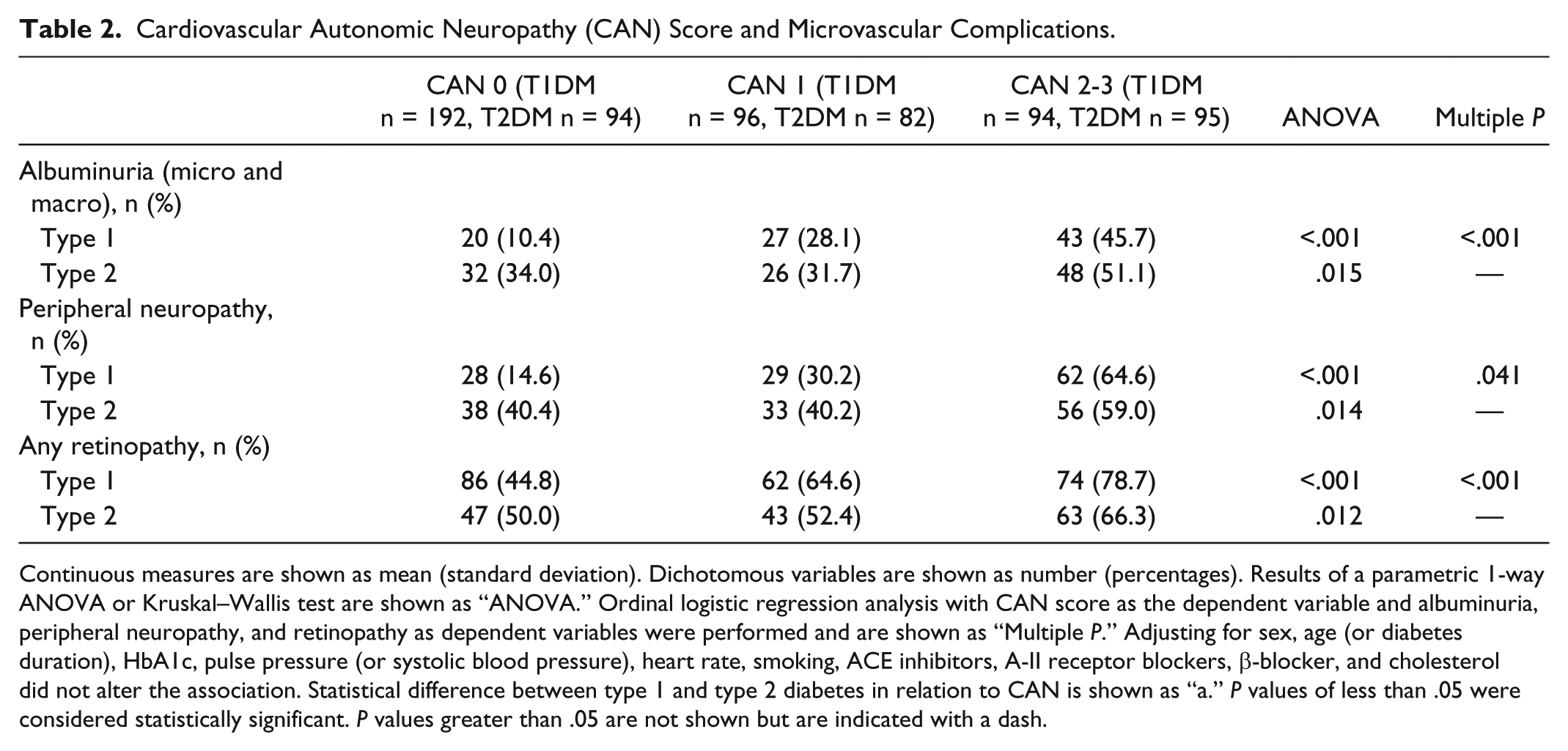
Continuous measures are shown as mean (standard deviation). Dichotomous variables are shown as number (percentages). Results of a parametric 1-way ANOVA or Kruskal–Wallis test are shown as “ANOVA.” Ordinal logistic regression analysis with CAN score as the dependent variable and albuminuria, peripheral neuropathy, and retinopathy as dependent variables were performed and are shown as “Multiple P.” Adjusting for sex, age (or diabetes duration), HbA1c, pulse pressure (or systolic blood pressure), heart rate, smoking, ACE inhibitors, A-II receptor blockers, β-blocker, and cholesterol did not alter the association. Statistical difference between type 1 and type 2 diabetes in relation to CAN is shown as “a.” P values of less than .05 were considered statistically significant. P values greater than .05 are not shown but are indicated with a dash.
Discussion
Large-scale screening in routine clinical practice in 4 outpatient clinics with the Vagus™ device was feasible. The study demonstrated that CAN is prevalent in patients with type 1 and type 2 diabetes from outpatient clinics in Denmark. Furthermore, the study demonstrated that CAN was independently associated with microvascular complication in type 1, whereas in Type 2 CAN was associated with macrovascular risk factors. The reported prevalence has been estimated to approximately 20-70% depending on the test cohort,3,5,6 and is higher among individuals with type 2 diabetes compared to individuals with type 1 diabetes. Using the examination guidelines from the ADA 14 and age-dependent cutoff levels, 6 we found a prevalence of manifest CAN in 35% among type 2 diabetes patients, and a prevalence of 25% among type 1 diabetes patients. In a feasibility study of the new handheld device used for performing CARTs, we used the same examination guidelines from ADA, but did not use age-dependent cutoff levels. 4 Without adjusting for age we found a lower prevalence of manifest CAN (28% in type 2 and 21% in type 1). Therefore, an age-dependent cutoff should always be used when analyzing CARTs. In the Danish arm of the ADDITION study, the 6-year prevalence of manifest CAN in people with screen-detected type 2 diabetes was 7%. 6 This study was performed using the same technical setup and the same age-dependent cutoff levels. The high prevalence of CAN found in type 2 diabetes patients in the present study may be due to the fact that diabetes patients participating in this study all were selected from tertiary reference centers and therefore generally had long duration of diabetes and were affected by complications, probably more than individuals with diabetes from a population-based sample. In this regard we demonstrated in a substudy of the ADDITION population that signs of autonomic nervous system dysfunction, measured by heart rate variability, are present already at the time of screen detected diabetes. 20 Therefore the higher prevalence of CAN in patients with type 2 as compared to type 1 diabetes may be due to longer duration of metabolic abnormalities before diagnosis. It can also be speculated that different progression and pathophysiological mechanisms may account for the onset and development of CAN in type 1 and type 2 diabetes patients. The reported prevalence of CAN, albuminuria, peripheral neuropathy, and retinopathy found in this study appear to be in agreement with findings from other studies.3,5,21-23
Improvement in glycemic control is one important step in minimizing the progression of CAN.24 -26 The DCCT study showed that intensive glycemic control in type 1 diabetes patients induces a reduction in the incidence of microvascular complications and a reduction in both the incidence and progression of abnormal CARTs. 27 In the Steno 2 study multifactorial intervention involving focus on continued patient education, motivation and individualized risk assessment, have proved to reduce the risk of cardiovascular and microvascular events by about 50% in patient with type 2 diabetes and CAN by about 60%. 28 In line with this the UKPDS study showed that antihypertensive treatment (AHT) has a preventive effect on the development of microalbuminuria in type 2 diabetes patients. 24 Adding to this, it has been proposed that individuals with diabetes may benefit from cardioprotective drugs since ACE-inhibitors and beta-blockers have a protective effect on the kidneys and reduce the risk of cardiovascular complications by restoration of autonomic balance.7,29 In our study, ACE inhibitors were widely used in patients with manifest CAN (81% in type 1 vs 87% in type 2 patients). The general use of AHT in manifest CAN may be controversial because these patients suffer from impairment or reduced baroreflex sensitivity and in worst case orthostatic hypotension. Therefore, use of AHT in patients with CAN requires a careful and gradual dose titration and it may be appropriate to consider CARTs before AHT is initiated.
The Hoorn prospective study of glucose tolerance in a general population of Caucasian subjects (50-75 years of age) showed that autonomic dysfunction in patients already at risk (hypertension or history of cardiovascular disease) may be particularly hazardous. 30 From our results, obesity and smoking should also be added to the list of risk factors for manifest CAN. The association between BMI and CAN in type 2 diabetes patients is in line with the recommendations in the Toronto consensus report. 3 With regard to intervention in patients suffering from CAN, weight loss from both surgically induced and weight reduction programs have been reported to have a favorable effect on the cardiovascular autonomic profile in obese subjects with and without diabetes.31,32 Therefore non-weight-gaining antidiabetic medication like GLP-1 receptor agonists or DPP-4 inhibitors 33 might be favorable in obese patients with both early and manifest CAN.
The present study was designed as a cross-sectional observational study. Thus, it was not possible to control for all confounding factors. Most important, and in line with other prevalence studies, no direct adjustment was made for drugs affecting the cardiovascular system like β-blockers, which has previously been shown to be associated with improved parasympatic modulation and reduced heart rate. In spite of this possible beneficial intervention a high prevalence of patients with manifest CAN was observed. Furthermore, adjusting for age, mean heart rate and medications with a potential beneficial effect on the cardiovascular system (ACE inhibitors and β-Blocker) did not alter the association between CAN and macrovascular risk factors in type 2, or CAN and microvascular complication in type 1.
It has been shown that early detection of autonomic imbalance and focus on diabetes control and elimination of risk factors for autonomic neuropathy especially in patients with type 2 diabetes (obesity, smoking, and hypertension) can delay or slow the progression of diabetic neuropathy. 2 This observational study supports the view that drugs with beneficial effect on the cardiovascular system, lifestyle changes, and non-weight-gaining antidiabetic medication may be considered, but given the observational nature of this study these recommendations need to be confirmed in a prospective study. In conclusion, CAN is associated with different clinical variables in type 1 and type 2 diabetes, respectively. Macrovascular risk factors including BMI, pulse pressure, and smoking are more important for CAN in type 2 compared to type 1 diabetes.
Footnotes
Acknowledgements
The authors thank Dr Ulrick Espelund and Karin Ørbæk Kristensen, MSc for valuable comments. Parts of this study were presented in abstract form at the Eleventh Annual Diabetes Technology Meeting, San Francisco, California, October 27-29, 2011. Furthermore, this study was presented at ADA’s Scientific Sessions 2012.
Abbreviations
ADA, American Diabetes Association; CAN, cardiac autonomic neuropathy; CARTs, cardiovascular reflex tests.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JF is coinventor of Vagus™ and hold stocks in Medicus Engineering. No other potential conflicts of interest relevant to this article were reported.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.