
Abstract
Introduction:
Patients’ knowledge of their insulin pumps and glucose control during hospitalization has not been studied.
Aim:
The aim was to study the determinants of glycemic control in patients using continuous subcutaneous insulin infusion (CSII) in the hospital.
Methods:
Three groups of patients were identified: those who did not need any inpatient education and continued on CSII (gorup A), those who received education then continued on CSII (group B), and those for whom CSII was not appropriate and were treated with multiple daily insulin injections (gorup C). We compared the measures of glycemic control between the 3 groups and analyzed which variables impacted glucose control.
Results:
There were 50 patients, with 51 hospital admissions, 57% males, mean age 48 ± 13 years, 86% had type 1 diabetes (T1DM). The mean DM duration was 26 ± 14 years, mean duration of CSII use was 8.7 ± 6 years, and mean HbA1c was 7.6 ± 1.4%. The mean duration of hospital stay was 5.6 ± 4.6 days. Mean blood glucose (BG) and frequency of hyperglycemia and hypoglycemic events among the 3 groups adjusted for their duration of hospital stay were not statistically different. None of the patients developed diabetic ketoacidosis while using their pump. Stepwise multivariate analysis revealed knowledge of hypoglycemia correction was the single most important predictor of mean BG (P < .001).
Conclusion:
Patients who received inpatient education performed similarly to patients who did not need inpatient education. Patients who receive inpatient education on CSII fare similar as patients who did not require inpatient education.
Background
Over the past 30 years, there has been remarkable improvement in the delivery of insulin enhancing the management of diabetes. Delivery of insulin via continuous subcutaneous insulin infusion (CSII) or insulin pump has gained wide acceptance among physicians and patients with diabetes (DM). CSII is a sophisticated method of managing diabetes and requires commitment and understanding from both the patient and their care providers. As per the FDA report in 2007, approximately 375 000 patients are currently using CSII. 1 A majority of the health care providers who have type 1 diabetes (T1DM) use CSII for intensive control of their DM. 2 Use of insulin pump among patients with type 2 diabetes is also increasing.
Patients with DM are 3 times more likely to be hospitalized than patients without DM. 3 Of adult patients admitted to the hospitals, 20% to 30% have a known diagnosis of DM. 4 It is therefore to be expected that patients on CSII will be more commonly seen in the hospital setting. This leads to potential difficulties: hospital health care providers may not be familiar with insulin pumps, and patients who may be capable of, and comfortable with, the use of CSII in the ambulatory setting, may not be aware of potential problems posed by continued pump usage in the hospital.
When patients using CSII are hospitalized, a decision has to be made as to whether the patient can continue on the insulin pump or not. This depends on the ability of the patient to safely operate the pump and the health care provider’s familiarity with the CSII. 5 Patient satisfaction has been reported to be better if they are allowed to use their pump while in the hospital. 6 However use of the insulin pump in the hospital could also be source of medication errors, confusion among the hospital staff, and potentially harmful patient outcomes. It cannot be assumed that patients on CSII are always fully equipped to manage their insulin pump when faced with challenges during hospitalization. They may also not be aware that insulin pumps have to be removed for certain radiographic studies and not carry enough supplies (including tubing insertion sets and batteries). The characteristics of patients on CSII and their role in glucose control during hospitalization have not been studied.
The aim was to study the determinants of glycemic control in CSII-using patients in the hospital.
Methods
Current Insulin Pump Protocol in Our Institution
At our institution, an algorithm has been devised to identify hospitalized patients on insulin pumps and the option to consult endocrinology service in the management of those patients. There is a standardized order set for insulin pump order entry and endocrine consultation. The bedside nurse goes over the standardized patient instructions for safe use of the insulin pump in the hospital. All patients are placed on carbohydrate controlled diet, that is, 45-75 grams of carbohydrates per meal. Patients on the insulin pump who are referred for endocrine consultation are assessed for suitability of pump use in the hospital, and are seen by the endocrine team (physician and nurse practitioner [NP] or endocrine fellow, as well as a certified diabetes educator [CDE] and nutritionist). The endocrine team members, especially the CDEs, evaluate the patient’s familiarity with and comfort level in operating the insulin pump in the hospital in an effort to ensure to guide the CDEs in reeducating patients on pump use as needed. The CDEs assess the ability and willingness of the patients to count carbohydrates, dose prandial insulin, use the built-in pump calculator, give correction boluses, suspend the pump, set a temporary basal rate, and use the hospital point-of-care testing result to determine their correction bolus. Hypoglycemia management and insertion site changes are also discussed. Knowledge gaps are filled by the CDE as appropriate for the inpatient setting. If there are physical and cognitive limitations or gaps in knowledge that might impact the patient safety during the hospitalization, or if the patient prefers, the endocrine consult service discusses this with the patient and the primary team and CSII is discontinued with patient approval and use of multiple daily insulin injections is initiated.
Patient Data
Patients were identified through an institutional review board (IRB)–approved registry of patients referred to the endocrine service on CSII. A retrospective review of the 50 consecutive electronic charts from Jan 2012 to July 2012 was done to obtain data on demographics, medical history, pump characteristics, insulin dosage/settings in the pump, pump-related knowledge, and glucose control while in the hospital. CSII discontinuation was noted including reasons for this decision. Included patients were 18 years of age and older and evaluated by the CDEs. Patients who came in to the hospital with uncontrolled hyperglycemia, diabetic ketoacidosis (DKA) related to malfunctioning insulin pumps were excluded from the study. During this period the inpatient insulin orders had a preselected endocrine consult order and the nursing staff were educated to seek the help of the endocrinology service when handling patients on insulin pumps. All included patients had a bedside assessment of their knowledge on the insulin pumps. This assessment is recorded by the CDEs in the charts, which were reviewed as part of our study.
Definitions
The type of diabetes (type 1, type 2, or other) was determined from the endocrine team’s consult note. Point-of-care (POC) blood glucose values performed during their hospital stay was recorded. Hyperglycemia was defined as any value >200 mg/dl and hypoglycemia was defined as any value <70 mg/dl. When glucose was measured at multiple times within a 3 hour period, the highest value for hyperglycemia or lowest value for hypoglycemia was taken into account. Frequency of hyper/hypoglycemia was measured as number of hyper/hypoglycemic events out of the total number of POC glucose measurements. Patients were assessed for their ability to demonstrate important pump settings, use the built-in pump calculator program, suspend the pump, set a temporary basal, deliver correction boluses, correct for hypoglycemia, count carbohydrates, and use back-up insulin in case of pump malfunction. On the basis of the education given to the patients and the endocrine team’s decision, patients fell into 3 categories: group A comprised patients who did not need further education from the endocrine consult team and continued to use the pump in the hospital, group B were patients who needed some education from the endocrine team and continued to use their insulin pump in the hospital, and group C consisted of patients who had to come off the insulin pump and were placed on subcutaneous insulin injections. The assessment was only made at baseline before any teaching was provided and patients were not reclassified after education. Some patients in group A and group B had to have their insulin pumps removed during the perioperative period for logistical reasons. POC glucose measurements for these patients were recorded separately as periods of CSII use (on pump) and nonuse (off pump) were recorded. Outcomes included mean blood glucose and frequencies of hyperglycemia and hypoglycemia. A waiver of consent was granted by the institution IRB.
Statistical Analysis
The blood glucose data were recorded as mean ± standard deviation (SD), while hyper/hypoglycemic events as frequencies. Mean BG between the 3 groups were compared using the ANOVA test and mean BG during periods of on pump and off pump by paired t test. Stepwise multivariate analysis for various measured patient characteristics was calculated using stepwise logistic regression (JMP software). Further analysis was done by attempting to do a linear score. The 8 items assessed were added for a composite score of 8. Spearman’s correlation with mean glucose was calculated for patients.
Results
Baseline characteristics of the patients are listed in Table 1. There were 50 patients, with 51 hospital admissions, 57% males, mean age 48 ± 13 years, 86% T1DM. The mean DM duration was 26 ± 14 years, mean duration of CSII was 8.7 ± 6 years, mean A1c was 7.6 ± 1.4 % (range 5.2-13.2 %), and 78% were followed by endocrinologists. The mean duration of the hospital stay was 5.6 ± 4.6 days. The patient’s pump-related knowledge is shown in Table 2. Almost a quarter of patients could not demonstrate vital pump features, suspend their pump, or deliver bolus insulin, and about half of the patients could not demonstrate how to set a temporary basal rate. The mean blood glucose (BG), frequency of hyperglycemic and hypoglycemic events among the 3 groups both during CSII use and non-use are shown in Table 3. Mean BG was not statistically different among the 3 groups of patients. The frequency of hyperglycemia and hypoglycemic events was not different among the 3 groups.Though there was a higher mean frequency of hypoglycemia (10%) when using the pump as compared to when they were not using their pump (0.5%) in group B, this did not reach statistical significance. None of the patients in group A or group B developed DKA while on their insulin pump.
Baseline Characteristics of Patients.
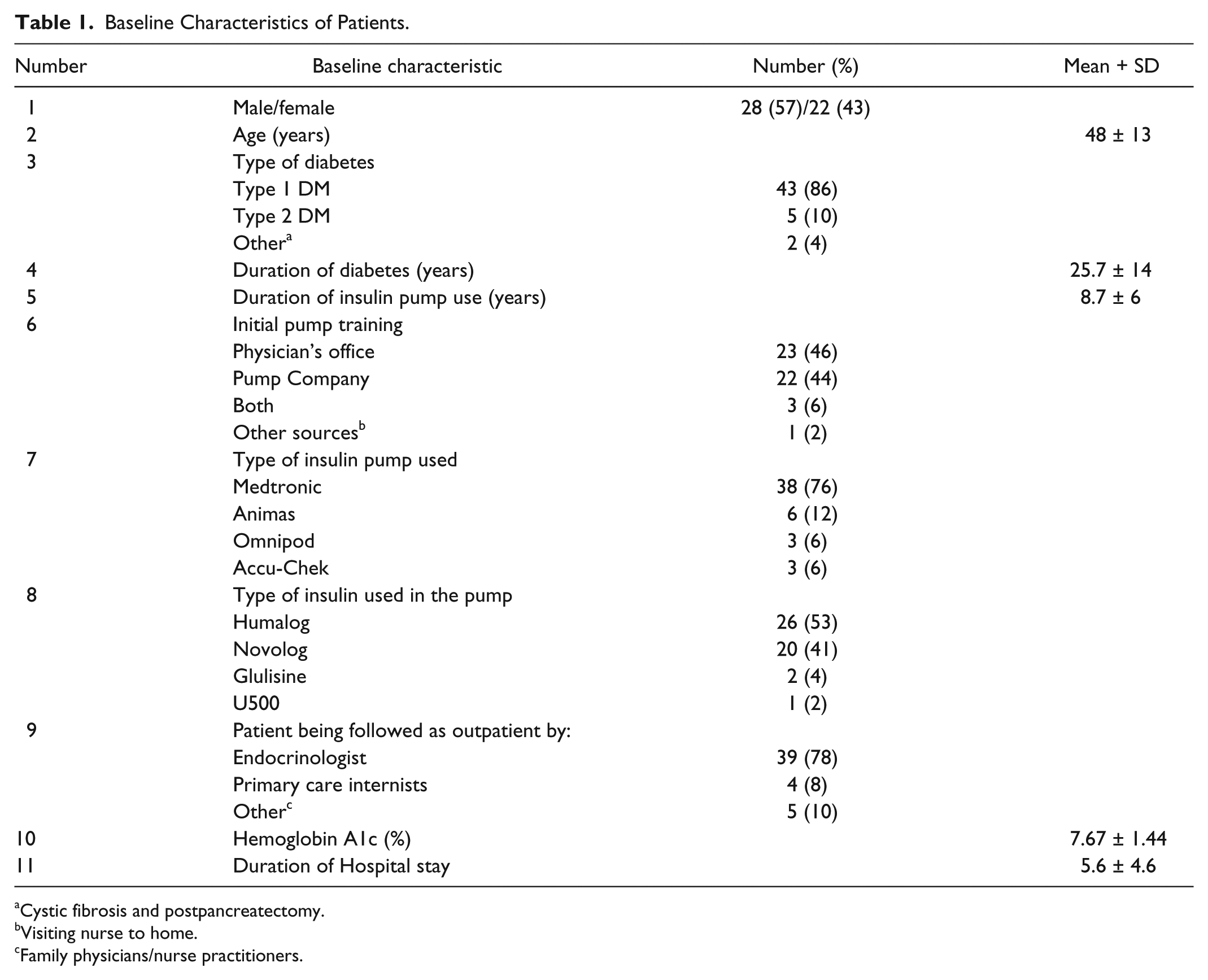
Cystic fibrosis and postpancreatectomy.
Visiting nurse to home.
Family physicians/nurse practitioners.
Patients’ Knowledge Metrics Evaluation.
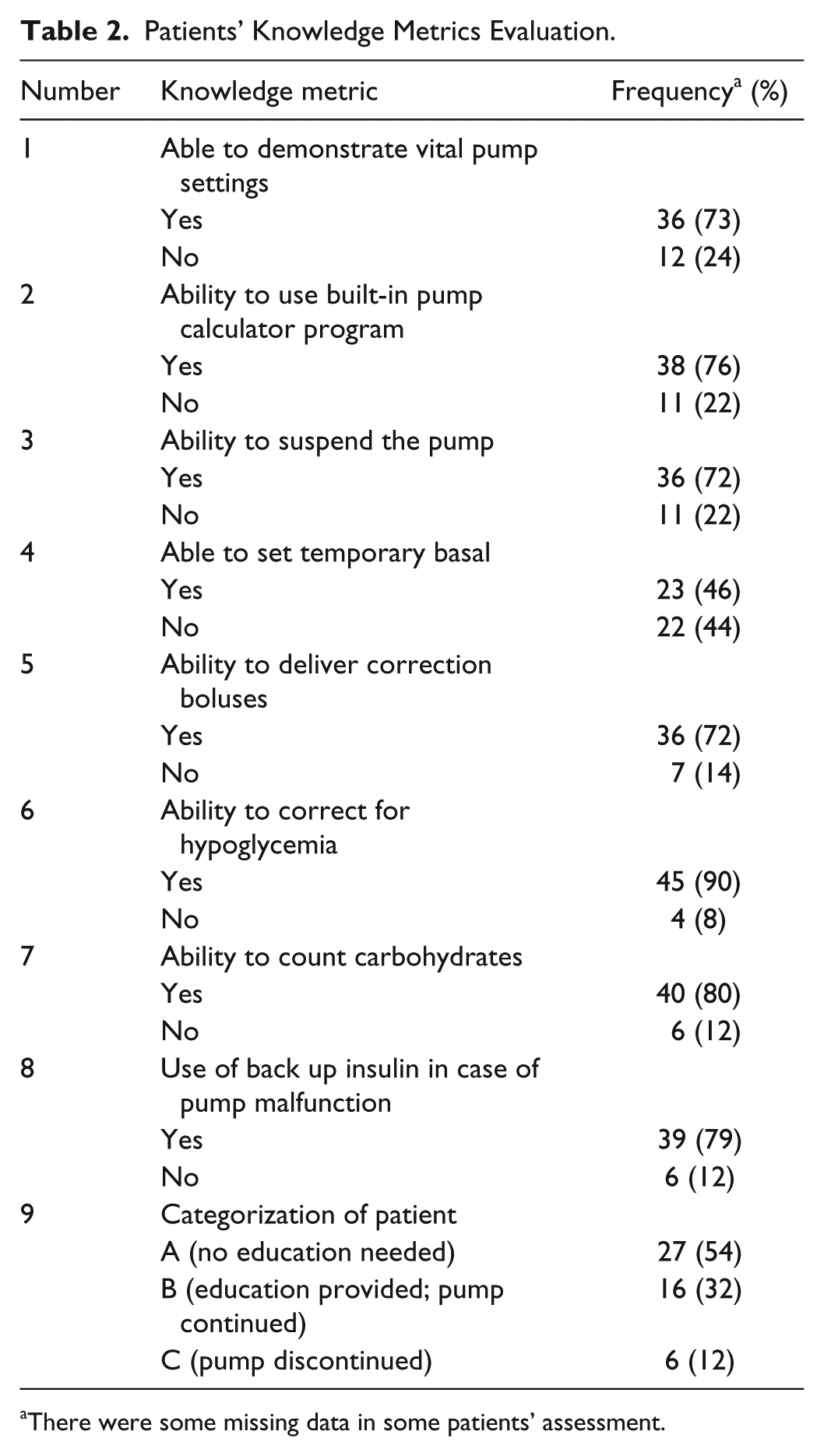
There were some missing data in some patients’ assessment.
Distribution of Mean Blood Glucose and Frequency of Hyperglycemia (>200) and Hypoglycemia (<70) Among the 3 Categories of Patients.
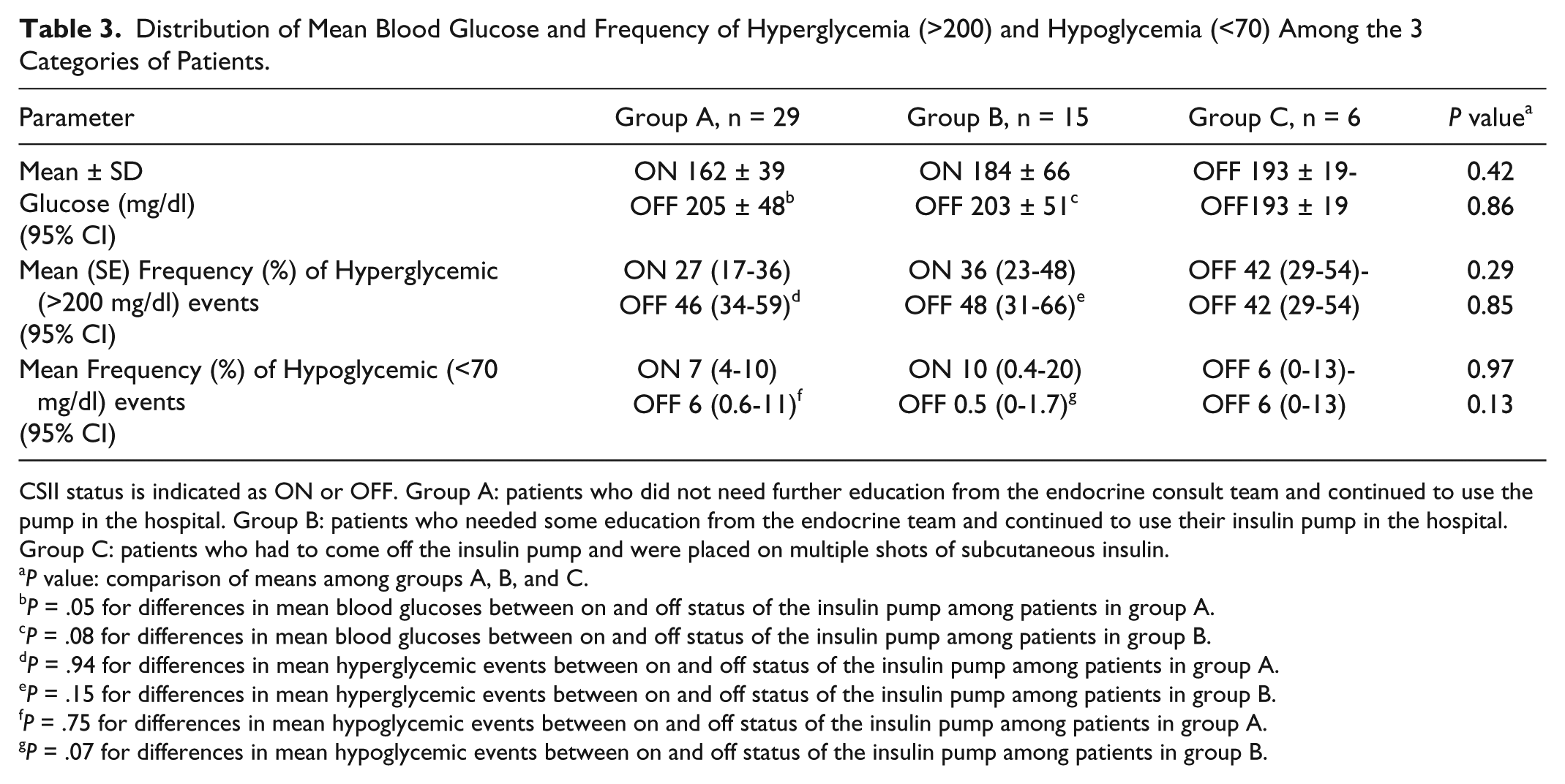
CSII status is indicated as ON or OFF. Group A: patients who did not need further education from the endocrine consult team and continued to use the pump in the hospital. Group B: patients who needed some education from the endocrine team and continued to use their insulin pump in the hospital. Group C: patients who had to come off the insulin pump and were placed on multiple shots of subcutaneous insulin.
P value: comparison of means among groups A, B, and C.
P = .05 for differences in mean blood glucoses between on and off status of the insulin pump among patients in group A.
P = .08 for differences in mean blood glucoses between on and off status of the insulin pump among patients in group B.
P = .94 for differences in mean hyperglycemic events between on and off status of the insulin pump among patients in group A.
P = .15 for differences in mean hyperglycemic events between on and off status of the insulin pump among patients in group B.
P = .75 for differences in mean hypoglycemic events between on and off status of the insulin pump among patients in group A.
P = .07 for differences in mean hypoglycemic events between on and off status of the insulin pump among patients in group B.
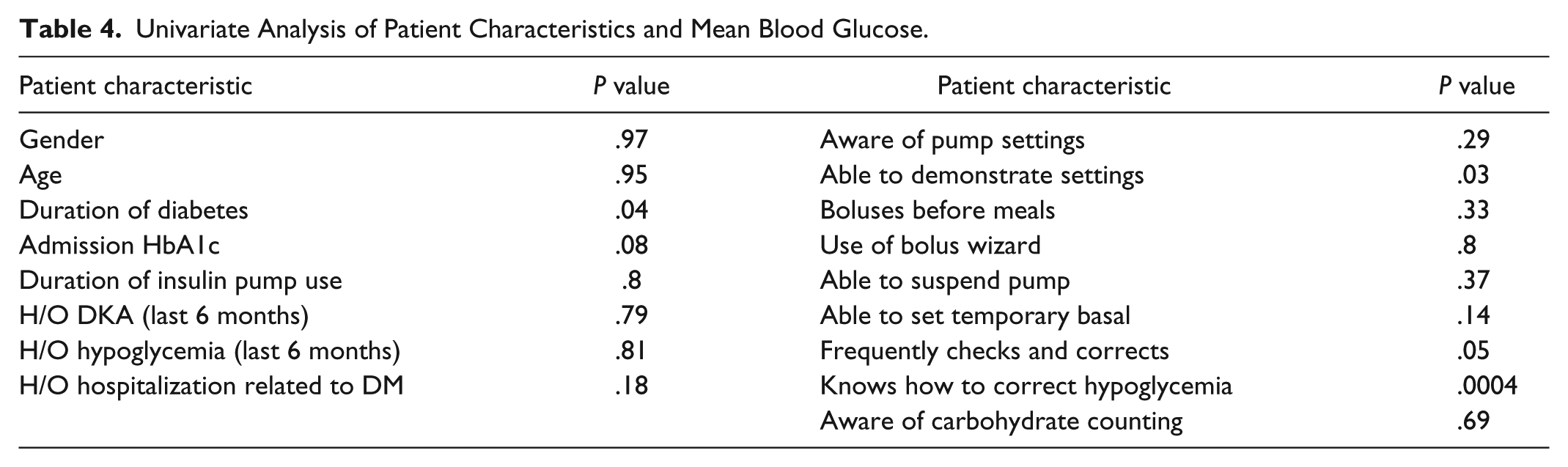
The reasons for discontinuation of the CSII in group C patients included patient preference (n = 3), inability to safely demonstrate pump settings (n = 2), and inexperienced due to recent initiation of CSII (n = 1). On discharge 3 out of the 6 patients were not restarted on their insulin pump. In 2 of the patients, the inability to correctly demonstrate appropriate pump settings and lack of family support resulted in discharging them on insulin injections, while in the third patient, postop mental status precluded use of the insulin pump. Among the various patient characteristics, the ability to demonstrate the pump settings (P = .03), duration of DM(P = .04), and knowledge of hypoglycemia correction (P = .0004) were significantly related to mean BG while on CSII (Table 4). Stepwise multivariate analysis revealed knowledge of hypoglycemia correction was the single most important predictor of mean BG (P < .001). Spearman’s rho was –.30 (95% CI –.58, –.02; P = .037) for all patients and was –.28 (95% CI –.61, .05; P = .091) for the patients whose data on the knowledge patients were complete. Cronbach’s alpha for the sum score was .83.
Univariate Analysis of Patient Characteristics and Mean Blood Glucose.
Discussion
Our study demonstrated that the mean BG and frequency of hyper/hypoglycemic events were not different in the 3 groups. Knowledge of hypoglycemia correction significantly correlated with mean BG during hospitalization. Patients who received inpatient pump education (group B) safely continued CSII during hospitalization, similar to patients who did not have knowledge gaps (group A). The American Diabetes Association advocates allowing patients who are physically and mentally able to continue using their pumps when hospitalized, having a hospital policy for CSII use, and having hospital personnel with expertise on pumps. 7 The American Association of Clinical endocrinologists echoes similar sentiment, and suggests contacting the specialist responsible for the pump in the ambulatory setting for decisions on adjustments while in the hospital, which may not be feasible at times. 8 CSII represents one of the best available method of delivering basal-bolus insulin and it makes sense to continue CSII while patients are in hospital if they are able to manage their pumps. Studies on insulin pumps in the hospital are sparse. One group has been reporting their updated experience over the years. In their latest retrospective study of 136 patients involved in 253 hospitalizations over a 6-year period, endocrinology consults and use of the insulin pump order set rose to 100% by 2011. 9 CSII was continued for the entire duration of the hospital stay in 65% of the hospitalizations, was used intermittently in 20%, and was discontinued with alternative insulin regimens given in 15%. The mean glucose level of these patients was 178 ± 47 mg/dL (mean + SD), with no significant difference between groups. There were significantly less episodes of severe hyperglycemia (glucose >350 mg/dL) among those who continued on the pump compared to intermittent users and to those taken off the pump, and less episodes of hypoglycemia (glucose < 40 mg/dL) in those who continued on the pump compared to those taken off the pump. Our study also noted lower mean BG in groups A and B while they were on the pump and a higher mean BG while not on their insulin pump. The higher mean BG in both groups A and B when they were not on the insulin pump stresses the importance of transition of CSII to basal bolus regimen. This may be fraught with difficulties including underestimation of insulin requirements, inability to fine-tune basal requirements, and lack of correctional boluses in between meals may result in higher mean BG when they are not on the pump. It also takes a few days in the transition to get accustomed to the patient’s insulin requirements in the hospital resulting in hyperglycemia. Early involvement of the endocrine consult service during this transition period is crucial.
Hypoglycemia rates while on the pump versus off the pump were not statistically different. However, since this may be due to a small sample size, we felt this merited some comment, especially in group B. Hypoglycemia on the insulin pump could be due to carbohydrate-controlled diet during the hospitalization, higher basal rates as outpatient (which sometimes compensates for lack of adequate meal bolus), and improved compliance with insulin boluses. Although not formally tested in this study, we feel education of this cohort not only on the operation of insulin pump but also on hypoglycemia is crucial, and these patients may benefit from frequent glucose checks and adjustment of their insulin pump parameters while in the hospital.
The items in the assessment of pump knowledge were determined as a result of evolving patient care and education that the physicians and CDEs frequently interviewed their patients and found it useful. Although our CDEs were not trained to administer these questionnaire, the answers given by patients were not weighed and there was no minimal score that was needed to qualify to use the pump in the hospital. Credit for partially correct responses was also not given. Future clinical studies with standardized questionnaire can help health care providers.
There has been scant literature on the assessment of patient knowledge of their insulin pumps during their stay in the hospital. Although this is a hypothesis-generating study, this is one of the first in its kind to look into the patient characteristics and its impact on glycemic control. There are multiple limitations in this study. First, the assessment form is not a validated questionnaire, and there is an element of subjectivity in the assessment of CSII knowledge; we feel standardizing a questionnaire for each institution will help decide and manage pump patients admitted to the hospital. Second is the small sample size, the inability to include all covariates that affect BG control (severity of illness, steroid use, nutrition, etc), and the look at the impact of insulin pump education on inpatient glucose control. Third, this was an initial exploratory study, and the small sample size in group C in comparison to all 3 groups was not statistically feasible.
Conclusions
Patients who receive inpatient pump education can safely continue CSII during hospitalization, similar to patients who did not have knowledge gaps. Knowledge of hypoglycemia correction significantly correlated with mean BG during hospitalization.
Footnotes
Acknowledgements
The authors would like to acknowledge James Bena, MS, for acting as consultant for our statistical analyses. A part of this research was presented as a poster at the ADA meeting in 2013.
Abbreviations
BG, blood glucose; CDE, certified diabetes educator; CSII, continuous subcutaneous insulin infusion; DKA, diabetic ketoacidosis; NP, nurse practitioner; T1DM, type 1 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Lansang is part of the advisory board for Sanofi Aventis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.