
Abstract

Continuous insulin infusion (CII) protocols with glycemic targets 110-140 mg/dl are suggested following cardiac surgery in patients with and without diabetes provided that these targets can be achieved with low risk for moderate (MH) and severe (SH) hypoglycemia.1-4 The purpose of this investigation was to investigate differences in efficacy and safety of these targets according to diabetes status.
Glycemic data were collected from 247 consecutive patients treated with 1 of 2 published CII protocols (P1 and P2) targeting blood glucose (BG) 110-140 mg/dl for ≤48 hours following cardiac surgery. 5 Diabetes status was defined by medical record documentation or preoperative A1c ≥ 6.5%. 6 Protocol efficacy was measured by time to BG target; percentage of BG 70-109, 110-140, 141-180, and >180 mg/dl; and percentage of patients with BG in target after goal achieved. Glycemic variability was determined as the BG coefficient of variation (CV). Protocol safety was defined as percentage of BG 40-69 mg/dl (MH) and <40 mg/dl (SH) and percentage of patients experiencing MH or SH. Statistical analysis was performed using SPSS version 17 software (SPSS Inc, Chicago, IL).
With the exception of older age in P1 subjects without diabetes, and higher A1c in P1 patients with and without diabetes, no differences were observed in clinical characteristics (Table 1). Glycemic outcomes were similar for patients with and without diabetes treated with P1, but not P2, where diabetes patients were less likely to have BG within goal, with higher mean BG and more glycemic variability than P2 patients without diabetes. P2 diabetes patients were older, were more obese, required more pressors, and took longer to achieve goal than those without diabetes. When comparing P1 and P2 diabetes groups, there were no differences in the percentage of patients treated with insulin (31% vs 42%) or oral agents (39% vs 49%) prior to admission. P1 diabetes patients had fewer valve procedures, received less pressor therapy, had lower baseline and mean BG, and had more BG within and below goal (Table 1). When comparing nondiabetes groups, P1 patients had more coronary artery bypass grafting (CABG) and fewer valve procedures. P1 versus P2 patients had lower mean BG and more BG below goal. The frequency of both MH and SH was low in all patients, expressed as percentage of BG measures, or as the number of patients experiencing hypoglycemia (Table 1). There were no differences in hospital LOS between the P1 and P2 diabetes (11.6 ± 5.5 vs 13.2 ± 7.4 days, P = .25) and nondiabetes (10.5 ± 4.5 vs 10.8 ± 8.7 days, P = .85) groups.
Clinical Characteristics of the Study Population.
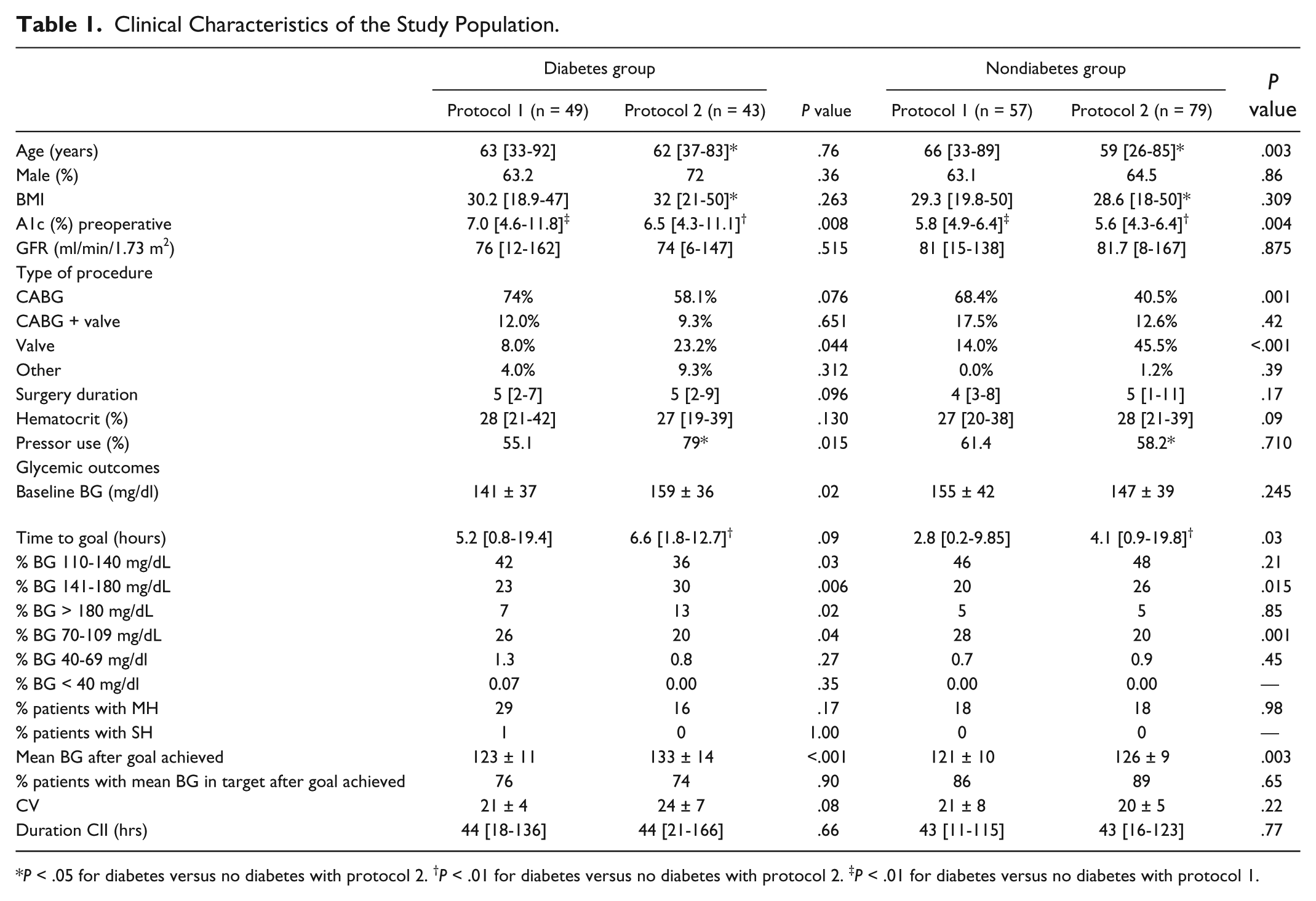
P < .05 for diabetes versus no diabetes with protocol 2. †P < .01 for diabetes versus no diabetes with protocol 2. ‡P < .01 for diabetes versus no diabetes with protocol 1.
In summary, this study demonstrates the efficacy and safety of 2 CII protocols with glycemic targets of 110-140 mg/dl in patients with and without diabetes following cardiac surgery.1,2,4 Despite noted differences in glycemic outcomes between protocols, mean BG was well within the desired range in all subgroups. The ability to achieve desired BG targets with low incidence of MH and SH in patients with and without diabetes supports suggested glycemic targets of 110-140 mg/dL following cardiac surgery, meeting the criterion that these goals be safely achieved. 5
Footnotes
Abbreviations
BG, blood glucose; BMI, body mass index; CABG, coronary artery bypass grafting; CII, continuous insulin infusion; CV, coefficient of variation; GFR, glomerular filtration rate; MH, moderate hypoglycemia; SH, severe hypoglycemia; P1, protocol 1; P2, protocol 2.
Authors’ Note
This study was presented as an abstract at the 2012 meeting of the American Diabetes Association.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MTK receives grant support from Sanofi-Aventis. JJ is on the speaker’s bureau for Sanofi, Lilly, and Medtronic.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by NIDDK—T35DK065521, Training in Renal, GI, Endocrine and Epithelial Biology.