
Abstract
Background:
Health care professionals (HCPs) routinely review handwritten blood glucose (BG) logbooks during office visits of patients with diabetes.
Method:
In this study, 64 HCPs were asked to assess glycemic patterns and estimate BG averages in six simulated handwritten logbooks. The HCPs then reviewed the pattern logs and averages in six OneTouch® Verio™IQ meters containing corresponding data sets.
Results:
The average time needed for pattern review was 7.3 min for handwritten logbooks versus 0.9 min using the meter. The total error rate for logbook pattern identification was 43.0% compared with the meter. The mean percentage deviation between HCP estimates of 30-day BG averages and actual values was 14.5%.
Conclusions:
The meter is associated with faster and more accurate pattern analysis compared with handwritten logbooks.
Introduction
In a 2012 survey of 24,216 U.S. physicians, 50% reported that the duration of each patient visit was ≥16 min. 1 For patients with diabetes who perform self-monitoring of blood glucose (SMBG), a portion of each patient office visit should include interpretation of retrospective data using logbooks, or downloaded data from glucose meters, and the assessment of resultant glycemic patterns.2,3 Given the short duration of patient office visits, health care professionals (HCPs) who provide diabetes care might benefit from technological advances that provide accurate blood glucose (BG) averages and reliable identification of glycemic patterns.
The OneTouch® Verio™IQ BG monitoring system (“meter”; LifeScan Inc., Milpitas, CA) incorporates PatternAlert™ technology, which analyzes BG readings in the meter's memory and alerts the user with a message when a glycemic pattern has been identified. 4 This study evaluated whether HCP use of this meter improves the accuracy and shortens the time of pattern analysis compared with conventional review of handwritten logbooks.
Methods
This study was an open evaluation conducted with 64 U.S. HCPs who had experience reviewing diabetes patient logbooks and making treatment decisions for their patients who use insulin based partly on logbook review.
Low and premeal high BG patterns were prospectively defined based on the algorithms used by the meter, and HCPs were asked to identify only those patterns in six logbooks containing 30 days of SMBG data. Logbooks were based on representative SMBG data from insulin patients with the particular low and high patterns in mind. The time to complete pattern identification and estimate BG average in logbooks (the “assessment”) was compared with the same assessment using a meter containing identical BG data. HCPs were given a maximum of 15 min to review each logbook and meter. Average assessment times were calculated for each HCP, and the overall mean assessment time was calculated using the average HCP times.
For each logbook, the percentage of missed low and high patterns was based on the number of patterns displayed by the meter. For example, a HCP may have missed 1/5 (20%) low and 2/8 (25%) high patterns. Note that the percentage of all (low and high) missed patterns is (1 + 2) / (5 + 8) = 23% and does not equal the sum of the percentage of missed low and missed high patterns. Falsely marked patterns were calculated in the same manner. The total error rate was the sum of the overall (high and low) missed and falsely marked pattern error rates.
The HCP-estimated 30-day BG average for each of the six logbooks was compared with the BG averages shown on the meter (deviation). Average percentage deviation was determined for each HCP, and overall deviation was calculated using the average HCP deviations.
After conducting the logbook and meter assessments, HCPs completed a survey regarding the potential value of the features of the meter to them and their patients.
Results
A total of 64 HCPs, including 11 endocrinologists, 25 primary care physicians (PCPs), and 28 diabetes educators (DEs) completed the study. The average reported experience with logbook review was 11.1 years (19.0, 10.2, and 8.8 years for endocrinologists, PCPs, and DEs, respectively).
The 64 HCPs reviewed 384 logbooks that contained a total of 4435 low and high patterns. Mean assessment time to review a logbook was 7.3 min [95% confidence interval (CI) 6.8–7.9 min] compared with 0.9 min (95% CI 0.8–1.0 min) using the meter (
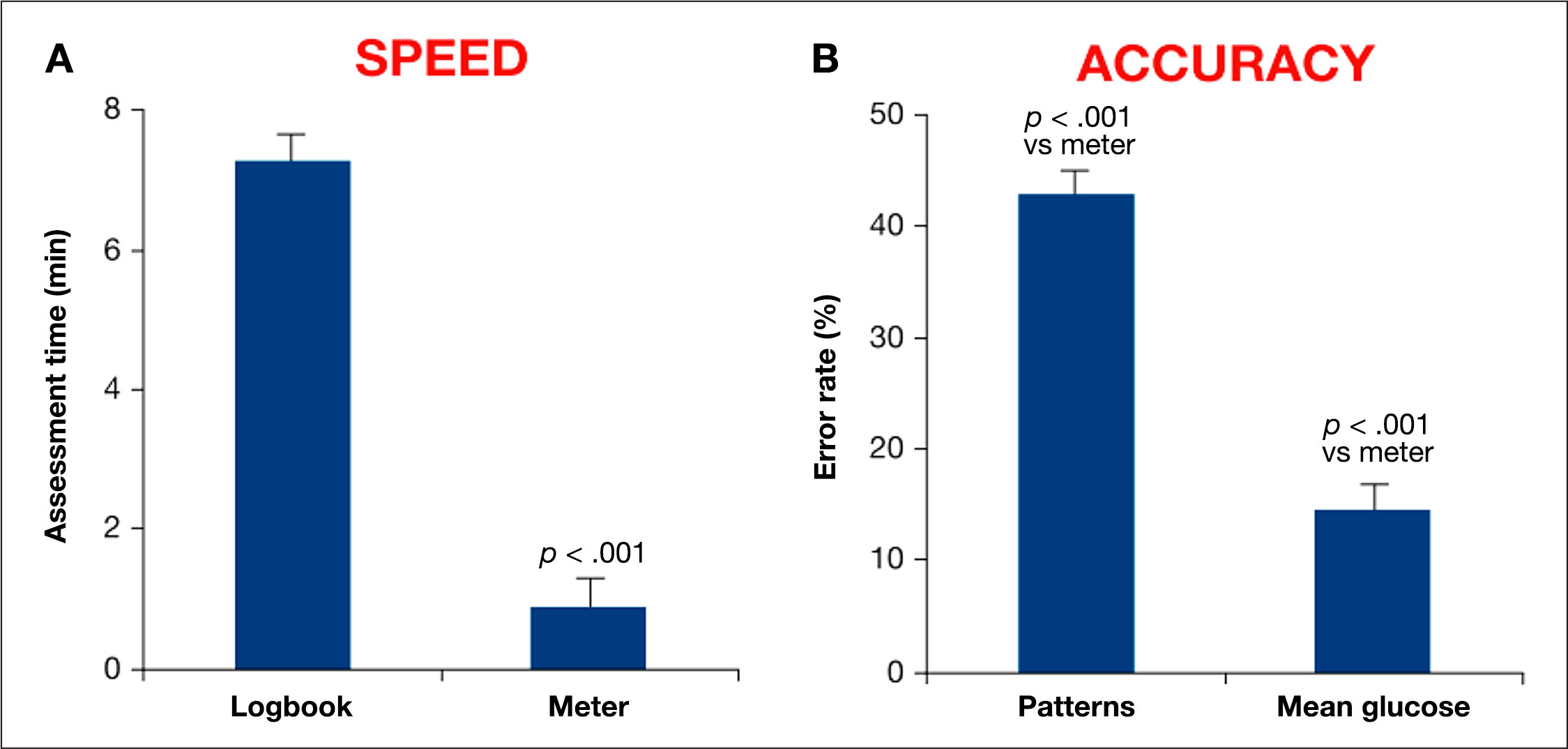
The mean percentage of missed and falsely marked patterns during logbook review compared with the patterns shown on the meter was 26.2% (95% CI 22–31%; p < .001) and 16.8% (95% CI 13–21%; p < .001), respectively. The total error rate (sum of missed and falsely marked patterns) was 43.0% (95% CI 31–55%; p < .001;
The mean 30-day BG average from the 384 meters was 146.8 ± 8.8 mg/dl. The HCP estimates deviated from meter values by 21.0 mg/dl (95% CI 7.9–24.1 mg/dl; p < .001) or by 14.5% (95% CI 12–17%; p < .001).
This study was not powered to detect differences among subgroups, but the 95% CI of the mean assessment times, BG estimates, and pattern identification error rates for endocrinologists, PCPs, and DEs overlapped, indicating similarity in results among subgroups.
Between 81% and 97% of the 64 HCPs gave favorable responses (agree or strongly agree) to the statements presented to them in a survey instrument
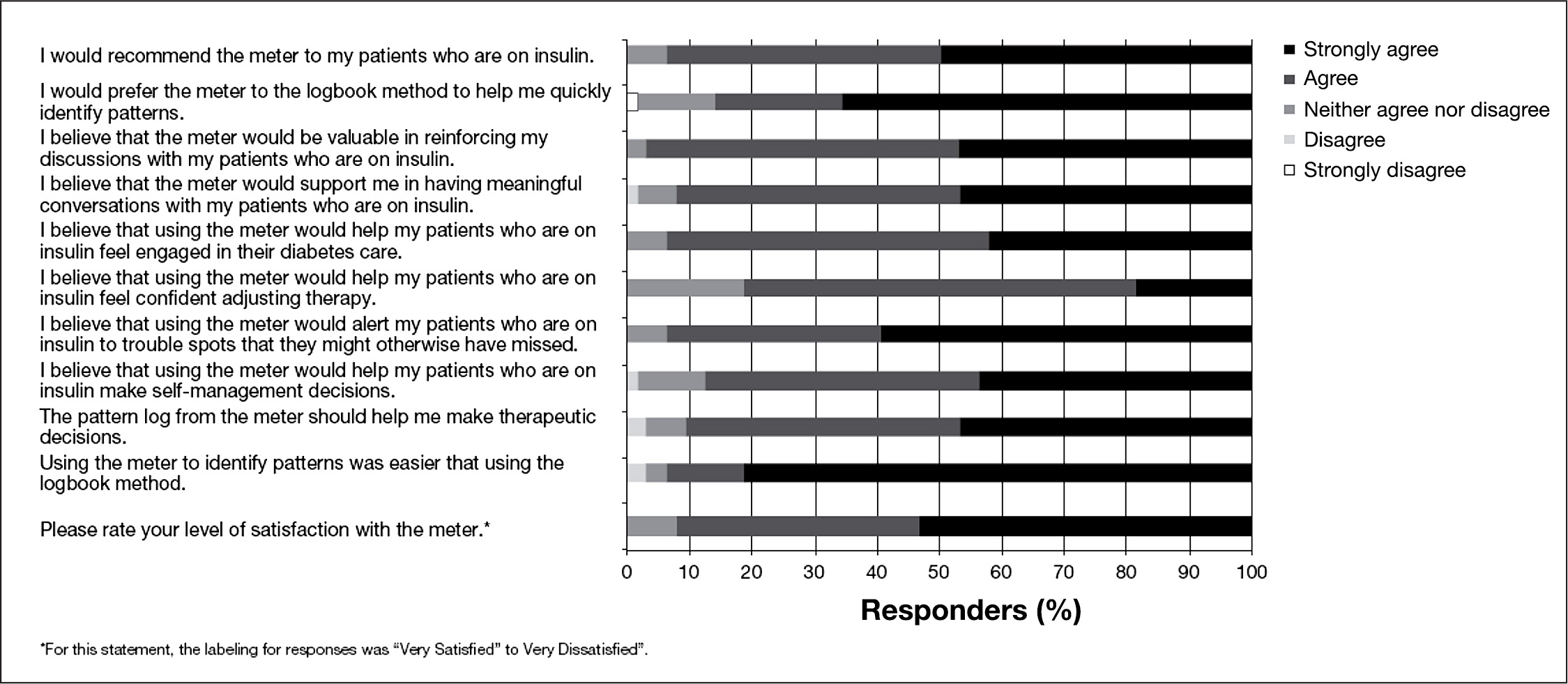
Response of 64 HCPs to survey statements regarding the features and potential use of the meter.
Discussion
Pattern management is the systematic interpretation of SMBG data over time to determine whether changes are needed to optimize BG control. 2 Pattern management involves (1) establishing preprandial and postprandia glycemic target values, (2) obtaining retrospective data and associated therapeutic information (e.g., BG, carbohydrate intake, medication, and lifestyle factors), (3) identifying glycemic patterns, (4) assessing influencing factors, and (5) taking appropriate actions. 3 Therefore, diurnal hyperglycemia and hypoglycemia patterns can provide valuable clinical insight.
The American Diabetes Association recommends proper interpretation of patient BG data. 5 The results of this study suggest that routine HCP reviews of handwritten logbook data may not be optimal. Using a meter with PatternAlert technology was associated with significant time-savings for HCPs and greater accuracy of pattern assessment and average BG estimation compared with manual logbook review. This study using simulated data focused on two BG patterns that are automatically detected by the meter, namely, low and premeal high BG patterns. Clearly there are other glycemic patterns that may be present in a patient. A future study will focus on these additional patterns as detected by off-device diabetes management software.
The survey completed by the participating HCPs suggested that using the meter might be useful to help them rapidly assess BG data and to make better management decisions for patients who are on insulin. Additionally, patient engagement with their clinicians regarding their diabetes management may improve with the use of the meter because of the increased accuracy of the tool and the time-savings for the clinicians. The use of the meter may facilitate greater, deeper, and more meaningful discussions between clinicians and their patients who are on insulin. Patients may feel more confident in managing their diabetes and more likely to follow their clinicians' recommendations. The survey also suggested that satisfaction with the meter is likely to be very high with those clinicians whose patients are using it.
Conclusions
When HCPs reviewed simulated handwritten BG logbooks, the pattern identification error rate compared with a glucose meter was 43.0%, and the mean deviation was 14.5% for estimates of BG averages. Using a meter with PatternAlert technology is associated with faster and more accurate pattern reviews compared with handwritten logbooks.
Footnotes
Abbreviations:
This study was funded by LifeScan Inc.
All authors are employees of LifeScan Inc.
Acknowledgments:
Parts of this study were presented as a poster at the International Clinical Diabetes Technology Meeting, Los Angeles, CA, April 20–21, 2012. The authors acknowledge Michael Pfeifer, John Bradford, Praveen Raja, and Jan Stegmann for their contributions to the development and/or evaluation of this study. The authors received editorial support from Excerpta Medica.